在麻醉工作区有效实施循证基础感染控制措施可以显著减少病原体传播和手术部位感染。可采用这些措施提升患者安全。本简要综述分析了实施阻碍较少的基础预防措施,并强调了其重要实施特点。
引言
 考虑到 COVID-19、1猴痘、2耳念珠菌3等感染性疾病的肆虐,以及与患者发病率和死亡率升高相关的手术部位持续感染 (SSI) ,因此在 2022 年预防感染对麻醉专业人士来说至关重要。4-6此外,由于任何感染都可能导致脓毒症,因此预防感染也意味着预防脓毒症。7在麻醉工作区采用循证的基础围手术期感染控制措施对病毒8和细菌病原体具有经证实的疗效,可显著减少病原体的传播和后续感染。8-10麻醉专业人士一直是患者安全领域的领导者,现在是时候利用已公布的数据,通过预防感染来提高患者安全。11
考虑到 COVID-19、1猴痘、2耳念珠菌3等感染性疾病的肆虐,以及与患者发病率和死亡率升高相关的手术部位持续感染 (SSI) ,因此在 2022 年预防感染对麻醉专业人士来说至关重要。4-6此外,由于任何感染都可能导致脓毒症,因此预防感染也意味着预防脓毒症。7在麻醉工作区采用循证的基础围手术期感染控制措施对病毒8和细菌病原体具有经证实的疗效,可显著减少病原体的传播和后续感染。8-10麻醉专业人士一直是患者安全领域的领导者,现在是时候利用已公布的数据,通过预防感染来提高患者安全。11
本综述强调了基础预防措施(实施阻碍较少)的重要实施特点。这些方法基于现有文献和相关感染控制指南(美国卫生保健流行病学学会 [SHEA]、12感染控制专业协会 [APIC]、13美国疾病控制和预防中心 [CDC]、14美国麻醉医师协会 [ASA]、15和美国麻醉护士协会 [AANA][AANA]16)。本文描述了适用于所有围手术期医务人员的围手术期感染控制措施的四大支柱,包括患者去定殖、手部卫生、血管护理及通过监测和反馈优化环境清洁。8,12
推荐的干预措施代表了旨在解决以下主要感染途径的最佳实践:1) 伤口直接污染,2) 在现有感染或患者护理所致感染引起的患者皮肤污染后出现的连续传播,3) 由各种麻醉工作区贮存器(如受污染的环境表面/设备)产生的病原体污染的微粒雾化,以及 4) 通过注射端口、针头和/或药瓶污染注入细菌病原体而引起的血源性传播。17重要的是,这些建议考虑到成本效益、18符合实际9且经证实具有实施的可行性。10
虽然这些预防措施中的每一项听起来可能都很熟悉,您和您的同事可能从一开始已在采用这些措施,但请仔细考虑每项建议的实施特点。使用正确的干预“剂量”对使患者从中获益至关重要。8-10,19图 1 的信息图表旨在描述感染预防如何在围手术期的一系列流程中延伸。对细菌传播的围手术期流行病学进行的缜密研究20-24支持在患者护理流程中同时实施通过反馈优化的多维方法(包括患者去定殖、手部卫生、血管护理和环境清洁改善措施),且该方法的疗效已得到证实。8-10但对于单一干预措施(如手部卫生、25,26患者去定殖27或环境清洁28),如果不进行反馈优化,很容易失败。
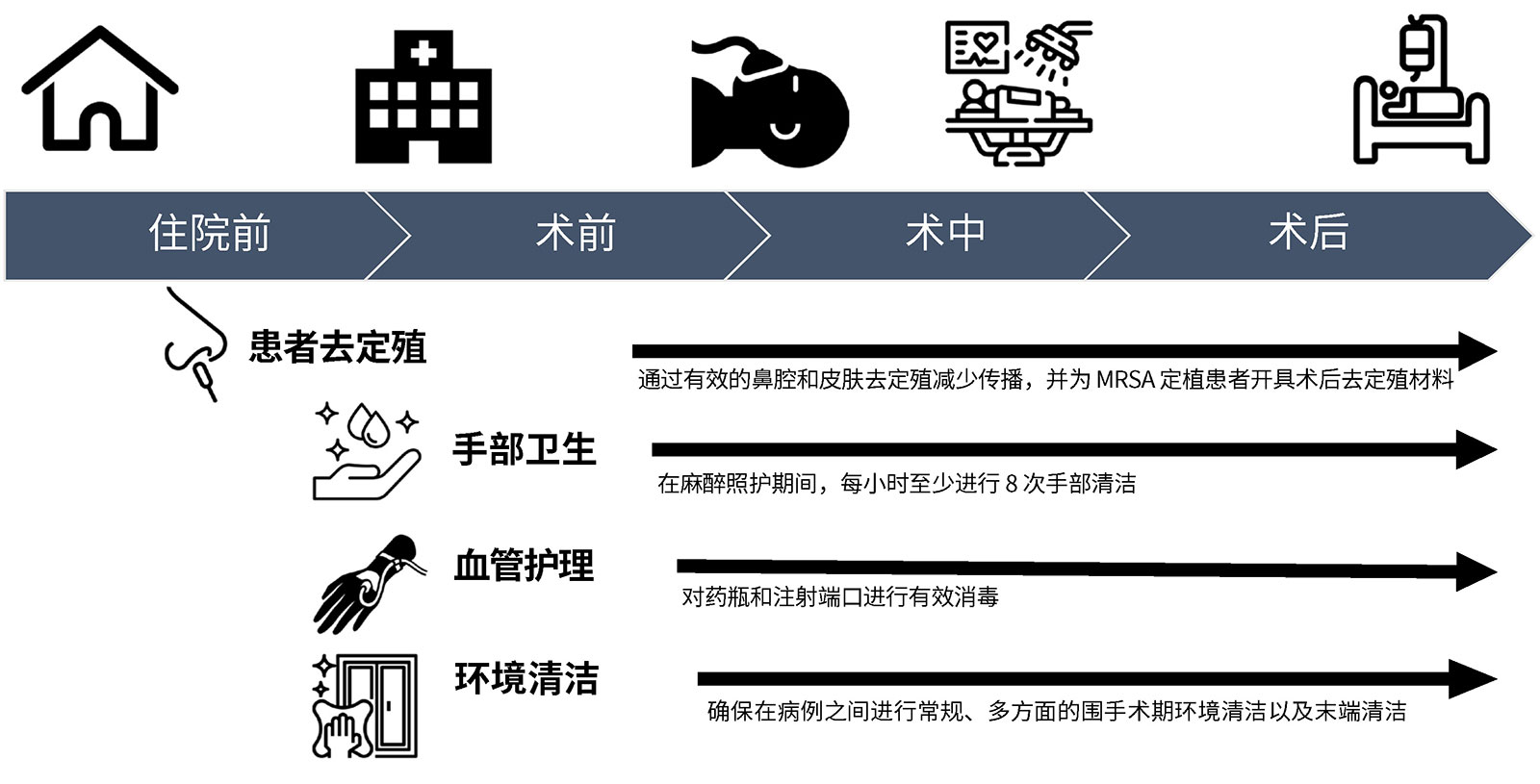
图 1:在围手术期一系列流程中减少感染传播的循证高价值机会。
患者去定殖:
建议:
- 在手术切口后一小时内给予两剂 5% 鼻用聚维酮碘,8,29并在手术当天早上使用 2% 葡萄糖酸氯己定擦拭纸。8,10,30
或者 - 用 5% 莫匹罗星鼻用软膏联合 2% 葡萄糖酸氯己定擦拭纸或 4% 洗涤剂至少治疗两天(最好是在手术前一天和手术当天)。30-32
- 为因医疗暴露而定殖耐甲氧西林金黄色葡萄球菌 (MRSA) 的患者开具出院后去定殖药物。32
依据:围手术期金黄色葡萄球菌传播的流行病学涉及患者皮肤部位(鼻孔、腋窝和/或腹股沟)的病原体定殖。8,10,33-35术后感染的出现与这些部位的金黄色葡萄球菌定殖密切相关。20,34,35如上文建议 1 和 2 所述,对患者皮肤部位去定殖可减少手术部位感染。8,10,30-32去定殖干预的最佳时机仍需更多研究。对医疗暴露所致 MRSA 定殖患者进行术后去定殖可显著降低医疗暴露后一年内发生侵袭性感染的风险。32对导致定殖的围手术期传播进行预防可强化这一效果。8,10
重要实施特点:随着抗生素耐药性的增强以及全球死亡率的增加,去定殖药物的选择变至得关重要。36,37碘和莫匹罗星均可有效预防 SSI。29-31鼻用莫匹罗星在某种程度上与耐药性增强有关,38而碘却无此作用。39,40碘可由麻醉专业人士在制造切口前给予两剂以进行术前管理。8,29而鼻用莫匹罗星需要进行 2-5 天的治疗。30,31对患者和医务人员是否依从开具的去定殖成分进行特定监测十分重要。
对患者和医务人员是否依从开具的去定殖成分进行特定监测十分重要。向医务人员提供有针对性的反馈,并监测去定殖用品的预期使用情况也很重要。8,10
手部清洁
建议:
- 增加麻醉照护期间的手部清洁频率。在麻醉照护期间每小时至少进行 8 次手部清洁41,在重症监护环境中提供照护时每小时至少进行 4 次手部清洁。42
- 提高环境清洁的频率和质量,以帮助改善手部卫生。8-10,43,44
 依据:在提供麻醉照护期间,会频繁且快节奏地接触手术室环境,往往涉及同时触摸患者和环境/设备。45考虑到手部和环境储存器之间已得到证明的联系,41改善手部卫生可以减少潜在的环境传染病传播事件。41,43,46最好在接触患者前后、体液暴露后、接触受污染环境后以及执行清洁/无菌任务前进行手部清洁:41,47这些是世界卫生组织 (WHO) 规定的“五大手部清洁时间点”。在麻醉照护期间,必须经常仔细地进行手部清洁,以尽可能多地抓住机会,减少病原体的传播。虽然不太可能在 WHO 指南确定的每次事件后都进行手部清洁,但麻醉专业人士必须尽可能多地进行手部清洁,以减少手术室病原体的传播。根据公布的数据推断,每小时进行至少八次手部清洁将显著减少潜在的传播事件。41在相关步骤中,进行更频繁和更高质量的环境清洁可以减少发生与手部污染相关的传播事件的可能性。8,10,41,43,46在诱导期间佩戴双手套可能有助于加强WHO 规定的手部卫生工作,但此方法仅在模拟环境中进行过测试,因此还需开展进一步的临床研究才可投入使用。45
依据:在提供麻醉照护期间,会频繁且快节奏地接触手术室环境,往往涉及同时触摸患者和环境/设备。45考虑到手部和环境储存器之间已得到证明的联系,41改善手部卫生可以减少潜在的环境传染病传播事件。41,43,46最好在接触患者前后、体液暴露后、接触受污染环境后以及执行清洁/无菌任务前进行手部清洁:41,47这些是世界卫生组织 (WHO) 规定的“五大手部清洁时间点”。在麻醉照护期间,必须经常仔细地进行手部清洁,以尽可能多地抓住机会,减少病原体的传播。虽然不太可能在 WHO 指南确定的每次事件后都进行手部清洁,但麻醉专业人士必须尽可能多地进行手部清洁,以减少手术室病原体的传播。根据公布的数据推断,每小时进行至少八次手部清洁将显著减少潜在的传播事件。41在相关步骤中,进行更频繁和更高质量的环境清洁可以减少发生与手部污染相关的传播事件的可能性。8,10,41,43,46在诱导期间佩戴双手套可能有助于加强WHO 规定的手部卫生工作,但此方法仅在模拟环境中进行过测试,因此还需开展进一步的临床研究才可投入使用。45
重要实施特点:将手部消毒液放置在术中医务人员易拿取处很重要,最好放置在麻醉工作区周围的几个地点,以便医务人员在快节奏的患者照护过程中随时消毒。41,43,44考虑将含酒精的手部消毒液放在麻醉机上,安装在静脉注射杆上8,10并佩戴在医务人员腰部。41手部卫生的重要性不仅限于麻醉团队成员。围手术期团队的所有成员(即循环护士、手术技术员、外科医生、临床麻醉技术员、受训人员和设备代表)在提供围手术期患者护理时均应采用建议的措施。
血管护理
建议:
- 使用 70%-90% 异丙醇对注射端口进行消毒,然后再进入。建议用力擦洗以产生 5-30 秒的摩擦,然后干燥。48-53如果使用设计用于清洁无针连接器的盖子,请使用经临床验证有效的产品,并遵循生产商的建议。其中一些设备需要至少 10 秒的接触时间才能有效发挥作用。49
- 避免使用开放式管腔(例如,无盖旋塞阀),因为其具有较高的污染风险,一旦受到污染就无法有效消毒,50且污染已一再与患者死亡率增加相关。20,52
- 在从药瓶上取下防尘盖后,在进入药瓶之前,先用酒精擦拭纸清洁所有药瓶,以防止出现污染和感染。53保持注射端口、注射器尖端和静脉导管远离地面。49
依据:每次连接之前,应使用 70%-90% 异丙醇拭子擦洗注射端口和药瓶,以对其进行消毒。8,10 虽然对于用乙醇拭子擦洗注射端口的持续时间并无一致意见,但我们建议将总时间保持在 5-30 秒,并用力擦拭以产生摩擦,然后风干。48-53在一项随机体外研究中,以这种方式进行擦洗并干燥 30 秒可避免注射过程中受到麻醉专业人士手部细菌的污染。48
研究表明,如果不遵循上述的良好血管通路无菌操作实践,多达 5 万个活菌菌落形成单位会被注入静脉 (IV) 液体通道。48这是出现手术部位和血流感染的主要途径54,可能会使患者死亡率增加几倍。55重要的是,术中旋塞阀污染已多次与患者死亡率增加相关,且与其直接相关(通过对术后感染进行先进的分子分型确定)。20,56在多个中心进行的随机对照临床试验41表明,通过使用安装在静脉杆上的带消毒帽的注射端口改善血管护理可以显著减少病原体传播和感染并发症。随着最近证实一名患者的静脉旋塞阀被 SARS-CoV-2 污染9,使得这些建议的重要性超出了细菌病原体的范畴。
重要实施特点:在医务人员附近放置酒精垫和酒精消毒帽,方便其使用消毒工具。44每种消毒方法确定合适的消毒时间。48-50
环境清洁
建议:
- 使用 2 次清洗法进行诱导后/镇静后清洁,擦拭所有湿巾含至少一种酒精和季铵盐化合物。43,46使用超细纤维布增加对生物负荷的去除。28
- 将环境分为成清洁/污染区。46
- 使用功效、有效性和实施可行性经证实的紫外线进行照射,加强表面消毒清洁效果。9进行监控,以有针对性地实施更先进的清洁程序。10,21,57
依据:围手术期环境清洁涉及多个方面,包括常规清洁、病例间清洁和末端清洁。环境污染在麻醉诱导和苏醒期间达到峰值,这两个时期与手卫生依从性的最低相关。43麻醉工作区环境(以麻醉机的可调限压阀和麻醉机刻度盘为代表)是强力传播媒介,且传播事件与感染的出现直接相关。20,53手术期间,至少有 50% 的金黄色葡萄球菌 SSI 与 ≥ 1 个麻醉工作区储存器有关。21在 Dartmouth Hitchcock Medical Center 进行的一项研究中,诱导后清洁、确认清洁/污染区、超细纤维布的使用以及多模式表面消毒纸的使用与测量的每个取样表面区域超过 100 CFU 的储存器数量显著减少相关,46该值是与后续发生感染相关高风险传播事件有关的污染阈值。8,10,20,56这些结果与一项在 ICU 环境中进行的精心设计的交叉试验的结果相似,该试验结果显示,增加清洁频率和超细纤维布的使用可以减少细菌污染。28将紫外线 C 光(UV-C) 作为循证多维方法(包括提升表面消毒环境清洁的频率和质量并使用 UV-C 予以增强、患者去定殖、血管护理和手部卫生)的一部分时,可以大幅减少金黄色葡萄球菌的传播、SARS-CoV-2 的传播以及 SSI。⁹
重要实施特点:采用诱导后/镇静清洁来解决环境污染的重要峰值,区分清洁/污染区,43,46并使用循证 UV-C 加强表面消毒清洁效果。8-10,58重要的是,所选 UV-C 设备应考虑手术室时间的重要性,59应制定实施策略,并证明其在预防术中细菌和病毒病原体传播方面具有有效性。
结论
麻醉团队可以很好地与围手术期手术/护理团队合作,以最大限度地减少围手术期细菌传播和后续感染。已制定相应的基础感染控制措施,并经过严格检验,其效果、有效性以及实施可行性和实用性均得到证明。麻醉专业人士可选择根据这些信息采取行动,以提高围手术期的患者安全。
Jonathan E. Charnin(医学博士)是梅奥诊所(明尼苏达州罗契斯特)的麻醉学副教授。
Melanie Hollidge(医学博士、哲学博士)是罗切斯特大学(纽约州罗切斯特)的麻醉学副教授。
Raquel Bartz(医学博士、MMCi)是 Brigham and Women’s Hospital(马萨诸塞州波士顿)的麻醉学副教授。
Desiree Chappell (CRNA) 是 NorthStar Anesthesia(德克萨斯州欧文)的临床质量副总裁。
Jonathan M. Tan(医学博士、MPH、MBI、FASA)是洛杉矶儿童医院(加利福尼亚州洛杉矶)、加利福尼亚大学(加利福尼亚州洛杉矶)凯克医学院以及空间科学研究所的麻醉学和空间科学副教授。
Morgan Hellman(RN、BSN)是 Pall Corporation(纽约州华盛顿港)的临床销售经理。
Sara McMannus(RN、BSN、MBA)是脓毒症联盟(加州圣地亚哥)的临床顾问。
Richard A. Beers(医学博士)是 Upstate Medical University(纽约州锡拉丘兹)上州医科大学的麻醉学教授。
Michelle Beam(DO、MBA、FASA)是宾夕法尼亚大学医学院(宾夕法尼亚州西切斯特)的麻醉学副教授。
Randy Loftus(医学博士)是爱荷华大学(爱荷华州爱荷华城)的麻醉学副教授。
利益冲突:Randy Loftus(医学博士)报告该研究的经费来自 NIH R01 AI155752-01A1“BASIC 试验:改进循证方法和监督的实施以防止细菌传播和感染”,并已获得麻醉患者安全基金会、Sage Medical Inc.、BBraun、Draeger、Surfaceide 和 Kenall 的资助,有一项或多项专利正在申请中,是 RDB Bioinformatics, LLC 和 1055 N 115th St #301, Omaha, NE 68154(OR PathTrac 母公司)的合作伙伴,曾在 Kenall 和 BBraun 赞助的教育会议上发言。爱荷华大学使用 RDB Bioinformatics PathTrac 系统测量细菌传播。
Jonathan Tan(医学博士、MPH、MBI、FASA)接受麻醉患者安全基金会 (APSF) 和麻醉教育与研究基金会 (FAER) 的研究资助。
Desiree Chappell (CRNA,) 是 Speakers Bureau for Medtronic and Edwards LifeSciences 以及 Advisory Board for ProVation 的成员。
Jonathan Charnin、Melanie Hollidge、Raquel Bartz、Morgan Hellman、Sarah McMannus、Richard Beers 和 Michelle Beam 报告无利益冲突。
参考文献
- Dexter F, Parra MC, Brown JR, et al. Perioperative COVID-19 defense: an evidence-based approach for optimization of infection control and operating room management. Anesth Analg. 2020;131:37–42. PMID: 32217947.
- Centers for Disease Control and Infection Prevention. Guidance for Tecovirimat use under expanded access investigational new drug protocol during 2022 U.S. monkeypox cases. https://www.cdc.gov/poxvirus/monkeypox/clinicians/Tecovirimat.html. Published 2022. Accessed July 26, 2022.
- Centers for Disease Control and Infection Prevention. Candida auris. Published 2022. https://www.cdc.gov/fungal/candida-auris/index.html. Accessed July 26, 2022
- Magill SS, Hellinger W, Cohen J, et al. Prevalence of healthcare-associated infections in acute care hospitals in Jacksonville, Florida. Infect Control Hosp Epidemiol. 2012;33:283–291. PMID: 22314066.
- Vogel TR, Dombrovskiy VY, Lowry SF. Impact of infectious complications after elective surgery on hospital readmission and late deaths in the U.S. Medicare population. Surg Infect (Larchmt). 2012;13:307–311. PMID: 23082877.
- Awad SS. Adherence to surgical care improvement project measures and post-operative surgical site infections. Surg Infect (Larchmt). 2012;13(4):234-237. PMID: 22913334.
- Centers for Disease Control and Infection Prevention. How can I get ahead of sepsis? https://www.cdc.gov/sepsis/prevention/index.html. Published 2022. Accessed July 26, 2022.
- Loftus RW, Dexter F, Goodheart MJ, et al. The effect of improving basic preventive measures in the perioperative arena on Staphylococcus aureus transmission and surgical site infections: a randomized clinical trial. JAMA Netw Open. 2020;3:e201934. PMID: 32219407.
- Loftus RW, Dexter F, Evans L, et al. Evidence-based intraoperative infection control measures plus feedback are associated with attenuation of severe acute respiratory syndrome coronavirus-2 detection in operating rooms. Br J Anaesth. 2022;129:e29–e32. PMID: 35643533.
- Wall RT, Datta S, Dexter F, et al. Effectiveness and feasibility of an evidence-based intraoperative infection control program targeting improved basic measures: a post-implementation prospective case-cohort study. J Clin Anesth. 2022;77:110632. PMID: 34929497.
- Warner MA, Warner ME. The evolution of the anesthesia patient safety movement in america: lessons learned and considerations to promote further improvement in patient safety. Anesthesiology. 2021;135:963–974. PMID: 34666350.
- Munoz-Price LS, Bowdle A, Johnston BL, et al. Infection prevention in the operating room anesthesia work area. Infect Control Hosp Epidemiol. 2019;40:1–17. PMID: 30526699.
- Association for Professionals in Infection Control. Infection preventionist’s guide to the OR. https://apic.org/infection-preventionists-guide-to-the-or/. Published 2018. Accessed July 29, 2022.
- Berrios-Torres SI, Umscheid CA, Bratzler DW, et al. Centers for Disease Control and Prevention guideline for the prevention of surgical site infection, 2017. JAMA Surg. 2017;152:784–791. PMID: 28467526.
- American Society of Anesthesiologists. Infection control and prevention. https://www.asahq.org/shop-asa/e020s10w02. Published 2022. Accessed July 26, 2022.
- American Association of Nurse Anesthesiology. Infection prevention and control guidelines for anesthesia care. https://www.aana.com/docs/default-source/practice-aana-com-web-documents-(all)/professional-practice-manual/infection-prevention-and-control-guidelines-for-anesthesia-care.pdf?sfvrsn=850049b1. Published 2015. Accessed July 26, 2022.
- Menz BD, Charani E, Gordon DL, et al. Surgical antibiotic prophylaxis in an era of antibiotic resistance: common resistant bacteria and wider considerations for practice. Infect Drug Resist. 2021;14:5235–5252. PMID: 34908856.
- Dexter F, Epstein RH, Loftus RW. Quantifying and interpreting inequality of surgical site infections among operating rooms. Can J Anaesth. 2021;68:812–824. PMID: 33547628.
- Dexter F, Ledolter J, Wall RT, et al. Sample sizes for surveillance of S. aureus transmission to monitor effectiveness and provide feedback on intraoperative infection control including for COVID-19. Perioper Care Oper Room Manag. 2020;20:100115. PMID: 32501426.
- Loftus RW, Brown JR, Koff MD, et al. Multiple reservoirs contribute to intraoperative bacterial transmission. Anesth Analg. 2012;114:1236–1248. PMID: 22467892.
- Loftus RW, Dexter F, Robinson ADM, Horswill AR. Desiccation tolerance is associated with Staphylococcus aureus hypertransmissibility, resistance and infection development in the operating room. J Hosp Infect. 2018;100:299–308. PMID: 29966756.
- Loftus RW, Brown JR, Patel HM, et al. Transmission dynamics of gram-negative bacterial pathogens in the anesthesia work area. Anesth Analg. 2015;120:819–826. PMID: 25790209.
- Hadder B, Patel HM, Loftus RW. Dynamics of intraoperative Klebsiella, Acinetobacter, Pseudomonas, and Enterobacter transmission. Am J Infect Control. 2018;46:526–532. PMID: 29395508.
- Loftus RW, Muffly MK, Brown JR, et al. Hand contamination of anesthesia providers is an important risk factor for intraoperative bacterial transmission. Anesth Analg. 2011;112:98–105. PMID: 20686007.
- Rupp ME, Fitzgerald T, Puumala S, et al. Prospective, controlled, cross-over trial of alcohol-based hand gel in critical care units. Infect Control Hosp Epidemiol. 2008;29:8–15. PMID: 18171181.
- Koff MD, Brown JR, Marshall EJ, et al. Frequency of hand decontamination of intraoperative providers and reduction of postoperative healthcare-associated infections: a randomized clinical trial of a novel hand hygiene system. Infect Control Hosp Epidemiol. 2016;37:888–895. PMID: 27267310.
- Konvalinka A, Errett L, Fong IW. Impact of treating Staphylococcus aureus nasal carriers on wound infections in cardiac surgery. J Hosp Infect. 2006;64:162–168. PMID: 16930768.
- Wilson APR, Smyth D, Moore G, et al. The impact of enhanced cleaning within the intensive care unit on contamination of the near-patient environment with hospital pathogens: a randomized crossover study in critical care units in two hospitals. Crit Care Med. 2011;39:651–658. PMID: 21242793.
- Phillips M, Rosenberg A, Shopsin B, et al. Preventing surgical site infections: a randomized, open-label trial of nasal mupirocin ointment and nasal povidone-iodine solution. Infect Control Hosp Epidemiol. 2014;35:826–832. PMID: 24915210.
- Schweizer ML, Chiang HY, Septimus E, et al. Association of a bundled intervention with surgical site infections among patients undergoing cardiac, hip, or knee surgery. JAMA. 2015;313:2162–2171. PMID: 26034956.
- Bode LGM, Kluytmans JAJW, Wertheim HFL, et al. Preventing surgical-site infections in nasal carriers of Staphylococcus aureus. N Engl J Med. 2010;362:9–17. PMID: 20054045.
- Huang SS, Singh R, McKinnell JA, et al. Decolonization to reduce postdischarge infection risk among MRSA carriers. N Engl J Med. 2019;380:638–650. PMID: 30763195.
- von Eiff C, Becker K, Machka K, et al. Nasal carriage as a source of Staphylococcus aureus bacteremia. Study Group. N Engl J Med. 2001;344:11–16. PMID: 11136954.
- Kluytmans JA, Mouton JW, VandenBergh MF, et al. Reduction of surgical-site infections in cardiothoracic surgery by elimination of nasal carriage of Staphylococcus aureus. Infect Control Hosp Epidemiol. 1996;17:780–785. PMID: 8985763.
- Bhalla A, Aron DC, Donskey CJ. Staphylococcus aureus intestinal colonization is associated with increased frequency of S. aureus on skin of hospitalized patients. BMC Infect Dis. 2007;7:105. 17848192.
- Murray CJL, Ikuta KS, Sharara F, et al. Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399:629–655. PMID: 35065702.
- Laxminarayan R, Duse A, Wattal C, et al. Antibiotic resistance—the need for global solutions. Lancet Infect Dis. 2013;13:1057–1098. PMID: 24252483.
- Patel JB, Gorwitz RJ, Jernigan JA. Mupirocin resistance. Clin Infect Dis. 2009;49:935–941. PMID: 19673644.
- Houang ET, Gilmore OJ, Reid C, Shaw EJ. Absence of bacterial resistance to povidone iodine. J Clin Pathol. 1976;29:752–755. PMID: 821972.
- Bigliardi PL, Alsagoff SAL, El-Kafrawi HY, et al. Povidone iodine in wound healing: a review of current concepts and practices. Int J Surg. 2017;44:260–268. PMID: 28648795.
- Koff MD, Loftus RW, Burchman CC, et al. Reduction in intraoperative bacterial contamination of peripheral intravenous tubing through the use of a novel device. Anesthesiology. 2009;110:978–985. PMID: 19352154.
- Koff MD, Corwin HL, Beach ML, et al. Reduction in ventilator associated pneumonia in a mixed intensive care unit after initiation of a novel hand hygiene program. J Crit Care. 2011;26:489–495. PMID: 21439767.
- Rowlands J, Yeager MP, Beach M, et al. Video observation to map hand contact and bacterial transmission in operating rooms. Am J Infect Control. 2014;42:698–701. PMID: 24969122.
- Bischoff WE, Reynolds TM, Sessler CN, et al. Handwashing compliance by health care workers: The impact of introducing an accessible, alcohol-based hand antiseptic. Arch Intern Med. 2000;160:1017–1021. PMID: 10761968.
- Birnbach DJ, Rosen LF, Fitzpatrick M, et al. Double gloves: a randomized trial to evaluate a simple strategy to reduce contamination in the operating room. Anesth Analg. 2015;120:848–852. PMID: 24836472.
- Clark C, Taenzer A, Charette K, Whitty M. Decreasing contamination of the anesthesia environment. Am J Infect Control. 2014;42:1223–1225. PMID: 25444268.
- Boyce JM, Pittet D, Healthcare Infection Control Practices Advisory Committee. Society for Healthcare Epidemiology of America. Association for Professionals in Infection Control. Infectious Diseases Society of America. Hand Hygiene Task F. Guideline for hand hygiene in health-care settings: recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Infect Control Hosp Epidemiol. 2002;23:S3–40. PMID: 12515399.
- Loftus RW, Patel HM, Huysman BC, et al. Prevention of intravenous bacterial injection from health care provider hands: the importance of catheter design and handling. Anesth Analg. 2012;115:1109–1119. PMID: 23051883.
- Loftus RW, Brindeiro BS, Kispert DP, et al. Reduction in intraoperative bacterial contamination of peripheral intravenous tubing through the use of a passive catheter care system. Anesth Analg. 2012;115:1315–1323. PMID: 23144441.
- Greene ES. Challenges in reducing the risk of infection when accessing vascular catheters. J Hosp Infect. 2021;113:130–144. PMID: 33713758.
- Moureau NL, Flynn J. Disinfection of needleless connector hubs: clinical evidence systematic review. Nurs Res Pract. 2015;2015:796762. PMID: 26075093.
- Lamberg JJ YL. Swab all vials with alcohol. APSF Newsletter. https://www.apsf.org/article/swab-all-vials-with-alcohol/. Published 2012. Accessed July 26, 2022.
- Bennett SN, McNeil MM, Bland LA, et al. Postoperative infections traced to contamination of an intravenous anesthetic, propofol. N Engl J Med. 1995;333:147–154. PMID: 7791816.
- Centers for Disease Control and Infection Prevention. Checklist for prevention of central line associated blood stream infections. https://www.cdc.gov/HAI/pdfs/bsi/checklist-for-CLABSI.pdf. Published 2014. Accessed July 26, 2022.
- Agency for Healthcare Research and Quality. Central line-associated bloodstream infections (CLABSI). https://www.ahrq.gov/topics/central-line-associated-bloodstream-infections-clabsi.html. Published 2022. Accessed July 26, 2022.
- Loftus RW, Koff MD, Burchman CC, et al. Transmission of pathogenic bacterial organisms in the anesthesia work area. Anesthesiology. 2008;109:399–407. PMID: 18719437.
- Robinson ADM, Dexter F, Renkor V, et al. Operating room PathTrac analysis of current intraoperative Staphylococcus aureus transmission dynamics. Am J Infect Control. 2019;47:1240–1247. PMID: 31036398.
- Loftus RW, Dexter F, Evans LC, et al. An assessment of the impact of recommended anesthesia work area cleaning procedures on intraoperative SARS-CoV-2 contamination, a case-series analysis. J Clin Anesth. 2021;73:110350. PMID: 34098391.
- Birchansky B, Dexter F, Epstein RH, Loftus RW. Statistical design of overnight trials for the evaluation of the number of operating rooms that can be disinfected by an ultraviolet light disinfection robotic system. Cureus. 2021;13:e18861. PMID: 34804714.
