Evidence-based, basic infection control measures implemented effectively in the anesthesia work area can generate substantial reductions in pathogen transmission and surgical site infection development. These measures are indicated to improve patient safety. In this brief review, we characterize basic preventive measures with few perceived barriers to implementation and highlight key implementation features.
INTRODUCTION
 Infection prevention is of paramount importance for anesthesia professionals in 2022 given emerging infectious diseases such as COVID-19,1 Monkeypox,2 Candida auris,3 and the persistent nature of surgical site infections (SSIs) associated with increased patient morbidity and mortality.4-6 Further, as any infection can lead to sepsis, infection prevention is sepsis prevention.7 Evidence-based basic perioperative infection control measures for the anesthesia work area are of proven efficacy for viral8 and bacterial pathogens, generating substantial reductions in pathogen transmission and subsequent infection.8-10 It is time for anesthesia professionals, who have always been leaders in patient safety, to leverage the solid platform of published evidence to improve the safety of our patients through infection prevention.11
Infection prevention is of paramount importance for anesthesia professionals in 2022 given emerging infectious diseases such as COVID-19,1 Monkeypox,2 Candida auris,3 and the persistent nature of surgical site infections (SSIs) associated with increased patient morbidity and mortality.4-6 Further, as any infection can lead to sepsis, infection prevention is sepsis prevention.7 Evidence-based basic perioperative infection control measures for the anesthesia work area are of proven efficacy for viral8 and bacterial pathogens, generating substantial reductions in pathogen transmission and subsequent infection.8-10 It is time for anesthesia professionals, who have always been leaders in patient safety, to leverage the solid platform of published evidence to improve the safety of our patients through infection prevention.11
In this review we highlight important implementation features for basic preventive measures with few perceived barriers for implementation. These approaches are based on both current literature and pertinent infection control guidelines (Society for Healthcare Epidemiology of America [SHEA],12 Association for Professionals in Infection Control [APIC],13 Centers for Disease Control and Infection Prevention [CDC],14 American Society of Anesthesiologists [ASA],15 and the American Association of Nurse Anesthesiology [AANA]16). We describe four pillars of perioperative infection control measures applicable to all perioperative providers including patient decolonization, hand hygiene, vascular care, and environmental cleaning optimized by monitoring and feedback.8,12
The recommended interventions represent best practices designed to address the primary routes of infection that include 1) direct contamination of the wound, 2) contiguous spread following patient skin contamination occurring as a result of existing colonization or colonization resulting from patient care, 3) aerosolization of particles contaminated by pathogens arising from various anesthesia work area reservoirs such as contaminated environmental surfaces/equipment, and 4) hematogenous spread occurring as a result of injection of bacterial pathogens via injection port, syringe tip, and/or medication vial contamination.17 Importantly, these recommendations are cost-effective,18 practical,9 and with confirmed implementation feasibility.10
While each of these preventive measures may sound familiar, and it may initially seem that you and your colleagues are already employing these practices, please carefully consider the implementation features of each recommendation. Using the right “dose” of the intervention is important to obtain the benefits for your patients.8-10,19 Figure 1 is an infographic that was developed to depict how infection prevention extends across the perioperative continuum. A multifaceted approach involving patient decolonization, hand hygiene, vascular care, and environmental cleaning improvement efforts implemented in parallel during the process of patient care and optimized by feedback is supported by rigorous study of the perioperative epidemiology of bacterial transmission,20-24 and of proven efficacy.8-10 However, single interventions, such as hand hygiene,25,26 patient decolonization,27 or environmental cleaning28 without feedback optimization are prone to failure.
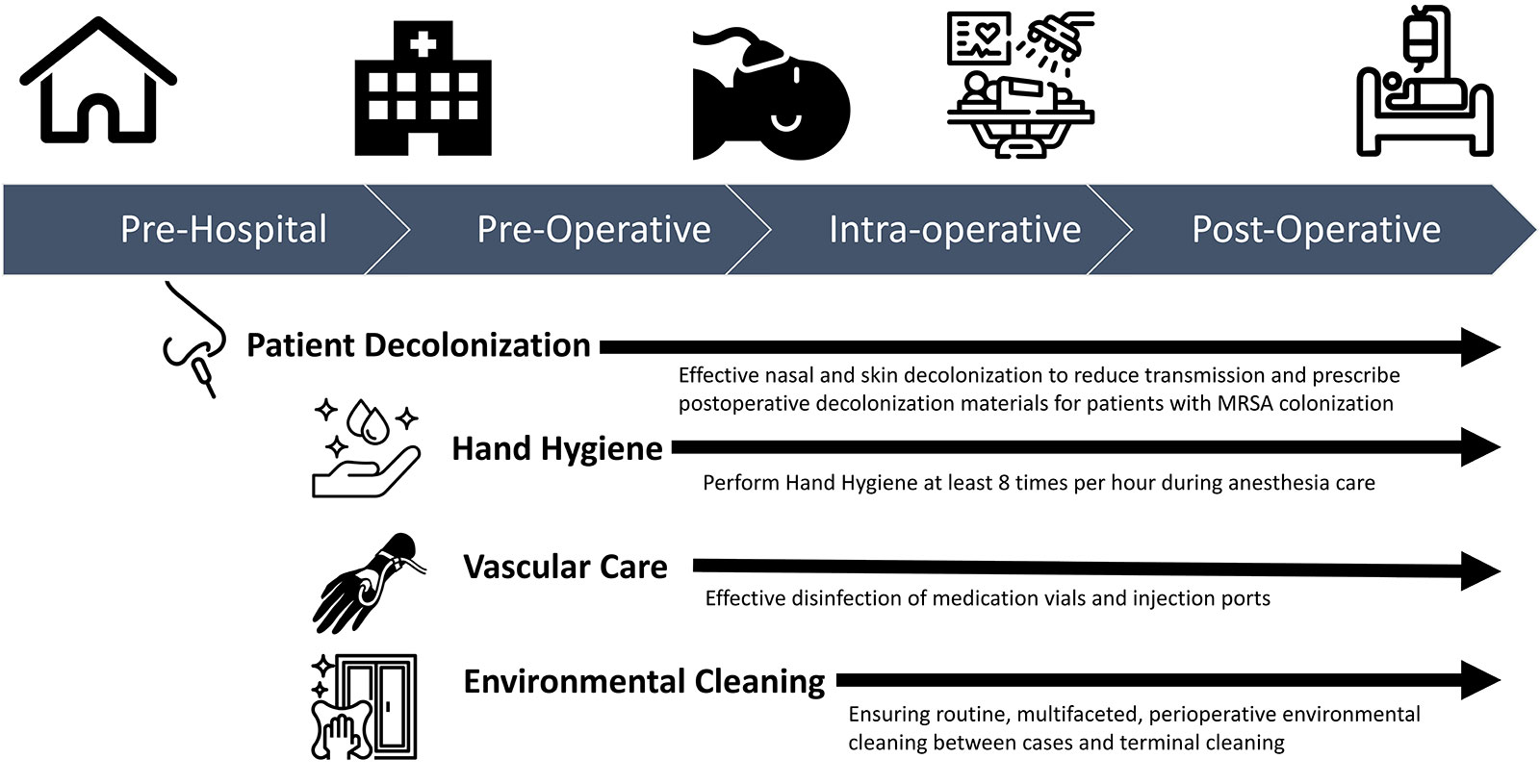
Figure 1: Evidence-based high-value opportunities to mitigate transmission of infection across the perioperative continuum.
PATIENT DECOLONIZATION:
Recommendations:
- Two doses of 5% nasal povidone iodine within one hour of the surgical incision8,29 and use of 2% chlorhexidine gluconate wipes on the morning of surgery.8,10,30
OR - At least 2 days of treatment (ideally the day before and the day of surgery) with 5% nasal mupirocin ointment with 2% chlorhexidine gluconate wipes or 4% shampoo.30-32
- Prescribe post-discharge decolonization for your patients colonized with methicillin-resistant Staphylococcus aureus (MRSA) as a result of the health care exposure.32
Rationale: The epidemiology of perioperative S. aureus transmission involves pathogen colonization of patient skin sites (nares, axilla, and/or groin). 8,10,33-35 Postoperative infection development is strongly tied to S. aureus colonization at these sites.20,34,35 As stated in recommendations 1 and 2 above, decolonization of patient skin sites reduces surgical site infections.8,10,30-32 The optimal timing of decolonization interventions still requires more research. Postoperative decolonization of patients colonized with MRSA occurring as a result of the health care exposure can significantly decrease the risk of invasive infection development up to one year following the health care exposure.32 Prevention of perioperative transmission resulting in colonization can augment the latter.8,10
Key Implementation Features: Choice of decolonization agent is important with increasing antibiotic resistance associated with an increase in worldwide mortality.36,37 Both iodine and mupirocin are efficacious for SSI prevention.29-31 Nasal mupirocin has been associated to some degree with increasing resistance,38 whereas iodine has not.39,40 Iodine can be managed preoperatively by the anesthesia professional with two doses given prior to incision.8,29 whereas nasal mupirocin requires 2–5 days of treatment.30,31
Specific monitoring of patient and provider compliance with prescribed decolonization components is important. Targeted feedback to providers and monitoring of expected utilization of decolonization supplies are also important.8,10
HAND HYGIENE
Recommendations:
- Increase hand hygiene frequency during anesthesia care. Perform hand hygiene at least 8 times per hour41 during anesthesia care and at least 4 times per hour while providing care in critical care environments.42
- Improve the frequency and quality of environmental cleaning to aid hand hygiene improvement efforts.8-10,43,44
 Rationale: Contact with the operating room environment is frequent and fast-paced during the provision of anesthesia care, often involving simultaneous touching of the patient and the environment/equipment.45 Given the demonstrated link between hand and environmental reservoirs,41 improved hand hygiene can reduce potential environmental infectious transmission events.41,43,46 Ideally, hand hygiene is performed before and after patient contact, after bodily fluid exposure, after contact with the contaminated environment, and before performing a clean/aseptic task:41,47 These are the “5 Moments of Hand Hygiene” described by the World Health Organization (WHO). During anesthesia care, hand hygiene must be performed frequently and thoughtfully to capture as many opportunities to reduce the transmission of pathogens as possible. While it may not be possible to perform hand hygiene after every event identified by the WHO guidelines, anesthesia professionals must do more to reduce the transmission of pathogens in the operating room. Inferred from published data, performing hand hygiene at least eight times hourly would significantly reduce potential transmission events.41 In a related step, more frequent and better-quality environmental cleaning can reduce the potential for transmission events associated with hand contamination.8,10,41,43,46 Double gloving during induction may augment WHO-based hand hygiene efforts, but further clinical study is indicated before adoption given only simulated environmental testing of this approach.45
Rationale: Contact with the operating room environment is frequent and fast-paced during the provision of anesthesia care, often involving simultaneous touching of the patient and the environment/equipment.45 Given the demonstrated link between hand and environmental reservoirs,41 improved hand hygiene can reduce potential environmental infectious transmission events.41,43,46 Ideally, hand hygiene is performed before and after patient contact, after bodily fluid exposure, after contact with the contaminated environment, and before performing a clean/aseptic task:41,47 These are the “5 Moments of Hand Hygiene” described by the World Health Organization (WHO). During anesthesia care, hand hygiene must be performed frequently and thoughtfully to capture as many opportunities to reduce the transmission of pathogens as possible. While it may not be possible to perform hand hygiene after every event identified by the WHO guidelines, anesthesia professionals must do more to reduce the transmission of pathogens in the operating room. Inferred from published data, performing hand hygiene at least eight times hourly would significantly reduce potential transmission events.41 In a related step, more frequent and better-quality environmental cleaning can reduce the potential for transmission events associated with hand contamination.8,10,41,43,46 Double gloving during induction may augment WHO-based hand hygiene efforts, but further clinical study is indicated before adoption given only simulated environmental testing of this approach.45
Key Implementation features: It is important to have hand sanitizers stationed in easy reach of intraoperative providers, including ideally in several places around the anesthesia work area, to facilitate use during fast-paced patient care.41,43,44 Consider placing alcohol-based hand sanitizers on the anesthesia machine, mounted to the intravenous pole8,10 and on the provider waist.41 The importance of hand hygiene is not limited to anesthesia team members. All members of the perioperative team (i.e., circulating nurses, scrub technologists, surgeons, clinical anesthesia technologists, trainees, and equipment representatives) should employ the recommended measures when providing perioperative patient care.
VASCULAR CARE
Recommendations:
- Disinfect injection ports, using 70–90% isopropyl alcohol prior to access. We suggest hard scrubbing to create friction for 5–30 seconds followed by drying.48-53 If using caps designed to clean needleless connectors, use products proven to be effective and follow manufacturer recommendations. Some of these devices require at least 10 seconds of contact time to be effective.49
- Avoid use of open lumens (e.g., uncovered stopcocks) as they are at increased risk of contamination, cannot be disinfected well once contaminated,50 and contamination has been repeatedly associated with increased patient mortality.20,52
- Clean all medication vials with an alcohol wipe after the dust cover is removed from the vial and prior to access to prevent contamination and infection.53 Keep injection ports, syringe tips, and IV tubing off the floor.49
Rationale: Injection ports and medication vials should be disinfected by scrubbing with a 70–90% isopropyl alcohol swab prior to each connection.8,10 While there is no consensus for duration of injection port scrubbing with ethanol swabs, we recommend a total time of 5–30 seconds with hard rubbing to create friction followed by air drying.48-53 Scrubbing in this manner followed by 30 seconds of drying time was shown to eliminate injection of bacteria from anesthesia professional hands in a randomized ex vivo study.48
Research has shown that up to 50,000 colony forming units of live bacteria are injected into the intravenous (IV) fluid pathway as a result of breaches in good vascular access aseptic practice as described above.48 This is a primary route of surgical site and blood stream infection development54 which can increase patient mortality severalfold.55 Importantly, intraoperative stopcock contamination has been repeatedly associated with increased patient mortality and directly linked by advanced molecular typing to postoperative infection development.20,56 Randomized controlled clinical trials at several centers41 have shown that improved vascular care through use of injection ports with disinfecting caps mounted to the IV pole can generate substantial reductions in pathogen transmission and infectious complications. With recent confirmation of intraoperative contamination of a patient intravenous stopcock with SARS-CoV-2,9 the importance of these recommendations extends beyond bacterial pathogens.
Key Implementation Features: Have alcohol pads and alcohol disinfecting caps close to providers, allowing easy access to disinfection tools.44 Use an appropriate disinfection time for each method of disinfection.48-50
ENVIRONMENTAL CLEANING
Recommendations:
- Implement postinduction/sedation cleaning using a 2-hit approach involving wipes containing at least one alcohol and a quaternary ammonium compound.43,46 Use microfiber cloth to increase removal of the bioburden.28
- Organize the environment into clean/dirty spaces.46
- Augment surface disinfection cleaning with ultraviolet irradiation with proven efficacy, effectiveness, and implementation feasibility.9 Use monitoring for targeted implementation of more advanced cleaning procedures.10,21,57
Rationale: Perioperative environmental cleaning is multifaceted, involving routine, between-case cleaning, and terminal cleaning. Environmental contamination peaks during induction and emergence of anesthesia, periods of patient care that correlate with nadirs in hand hygiene compliance.43 The anesthesia work area environment, represented by the adjustable pressure-limiting valve and agent dial of the anesthesia machine, is a potent transmission vehicle with transmission events directly linked to infection development.20,53 At least 50% of S aureus SSIs can be linked to ≥1 anesthesia work area reservoir at the time of the surgery.21 In a study performed at Dartmouth Hitchcock Medical Center, postinduction cleaning, organization of clean/dirty spaces, use of microfiber cloths, and use of multimodal surface disinfection wipes was associated with a significant reduction in the number of measured reservoirs exceeding 100 CFU per surface area sampled,46 a threshold of contamination associated with high-risk transmission events subsequently linked to infection.8,10,20,56 These results were similar to a well-designed crossover trial in the ICU environment where increased frequency of cleaning and use of microfiber cloths reduced bacterial contamination.28 When ultraviolet C light (UV-C) is employed as part of an evidence-based, multifaceted approach (including improved frequency and quality of surface disinfection environmental cleaning and augmentation with UV-C, patient decolonization, vascular care, and hand hygiene), substantial reductions in S. aureus transmission, SARS-CoV-2 transmission, and SSIs can be achieved.⁹
Key Implementation Features: Employ postinduction/sedation cleaning to address an important peak in environmental contamination, organize clean/dirty spaces,43,46 and augment surface disinfection cleaning with use of evidence-based UV-C.8-10,58 It is important that UV-C devices selected take into account the importance of operating room time,59 that implementation strategies have been delineated, and that they are of proven efficacy for prevention of intraoperative transmission of bacterial and viral pathogens.
CONCLUSION
Anesthesia teams are well positioned to work collaboratively with the perioperative surgical/nursing team to maximally attenuate perioperative bacterial transmission and subsequent infection. The basic infection control measures have been developed and rigorously tested with proven efficacy, effectiveness, and implementation feasibility and practicality. It is up to anesthesia professionals to act on this information to improve perioperative patient safety.
Jonathan E. Charnin, MD, is an assistant professor of Anesthesiology at the Mayo Clinic, Rochester, MN.
Melanie Hollidge, MD, PhD, is an associate professor of Anesthesiology at the University of Rochester, Rochester, NY.
Raquel Bartz, MD, MMCi, is an associate professor of Anesthesiology at Brigham and Women’s Hospital, Boston, MA.
Desiree Chappell, CRNA, is the vice president of Clinical Quality, NorthStar Anesthesia, Irving, TX.
Jonathan M. Tan, MD, MPH, MBI, FASA, is an assistant professor of Anesthesiology and Spatial Sciences, Children’s Hospital Los Angeles, Los Angeles, CA; Keck School of Medicine and the Spatial Sciences Institute, University of Southern California, Los Angeles, CA.
Morgan Hellman, RN, BSN, is the clinical sales manager for Pall Corporation, Port Washington, NY.
Sara McMannus, RN, BSN, MBA, is a clinical advisor, Sepsis Alliance, San Diego, CA.
Richard A. Beers MD, is a professor of Anesthesiology at Upstate Medical University, Syracuse, NY.
Michelle Beam, DO, MBA, FASA, is an associate professor of Anestheia at Penn Medicine, West Chester, PA.
Randy Loftus, MD, is an associate professor of Anesthesiology at University of Iowa, Iowa City, IA.
Conflicts of Interest: Randy Loftus, MD, reports current research funding from NIH R01 AI155752-01A1, “BASIC trial: Improving implementation of evidence-based approaches and surveillance to prevent bacterial transmission and infection” and has received funding from the Anesthesia Patient Safety Foundation, Sage Medical Inc., BBraun, Draeger, Surfacide, and Kenall, has one or more patents pending, is a partner of RDB Bioinformatics, LLC, and 1055 N 115th St #301, Omaha, NE 68154, a company that owns OR PathTrac, and has spoken at educational meetings sponsored by Kenall and BBraun. The University of Iowa uses RDB Bioinformatics PathTrac system for measuring bacterial transmission.
Jonathan Tan, MD, MPH, MBI, FASA, receives research grant funding from the Anesthesia Patient Safety Foundation (APSF) and the Foundation for Anesthesia Education and Research (FAER).
Desiree Chappell, CRNA, is on the Speakers Bureau for Medtronic and Edwards LifeSciences, and the Advisory Board for ProVation.
Jonathan Charnin, Melanie Hollidge, Raquel Bartz, Morgan Hellman, Sarah McMannus, Richard Beers, and Michelle Beam report no conflicts of interest.
References
- Dexter F, Parra MC, Brown JR, et al. Perioperative COVID-19 defense: an evidence-based approach for optimization of infection control and operating room management. Anesth Analg. 2020;131:37–42. PMID: 32217947.
- Centers for Disease Control and Infection Prevention. Guidance for Tecovirimat use under expanded access investigational new drug protocol during 2022 U.S. monkeypox cases. https://www.cdc.gov/poxvirus/monkeypox/clinicians/Tecovirimat.html. Published 2022. Accessed July 26, 2022.
- Centers for Disease Control and Infection Prevention. Candida auris. Published 2022. https://www.cdc.gov/fungal/candida-auris/index.html. Accessed July 26, 2022
- Magill SS, Hellinger W, Cohen J, et al. Prevalence of healthcare-associated infections in acute care hospitals in Jacksonville, Florida. Infect Control Hosp Epidemiol. 2012;33:283–291. PMID: 22314066.
- Vogel TR, Dombrovskiy VY, Lowry SF. Impact of infectious complications after elective surgery on hospital readmission and late deaths in the U.S. Medicare population. Surg Infect (Larchmt). 2012;13:307–311. PMID: 23082877.
- Awad SS. Adherence to surgical care improvement project measures and post-operative surgical site infections. Surg Infect (Larchmt). 2012;13(4):234-237. PMID: 22913334.
- Centers for Disease Control and Infection Prevention. How can I get ahead of sepsis? https://www.cdc.gov/sepsis/prevention/index.html. Published 2022. Accessed July 26, 2022.
- Loftus RW, Dexter F, Goodheart MJ, et al. The effect of improving basic preventive measures in the perioperative arena on Staphylococcus aureus transmission and surgical site infections: a randomized clinical trial. JAMA Netw Open. 2020;3:e201934. PMID: 32219407.
- Loftus RW, Dexter F, Evans L, et al. Evidence-based intraoperative infection control measures plus feedback are associated with attenuation of severe acute respiratory syndrome coronavirus-2 detection in operating rooms. Br J Anaesth. 2022;129:e29–e32. PMID: 35643533.
- Wall RT, Datta S, Dexter F, et al. Effectiveness and feasibility of an evidence-based intraoperative infection control program targeting improved basic measures: a post-implementation prospective case-cohort study. J Clin Anesth. 2022;77:110632. PMID: 34929497.
- Warner MA, Warner ME. The evolution of the anesthesia patient safety movement in america: lessons learned and considerations to promote further improvement in patient safety. Anesthesiology. 2021;135:963–974. PMID: 34666350.
- Munoz-Price LS, Bowdle A, Johnston BL, et al. Infection prevention in the operating room anesthesia work area. Infect Control Hosp Epidemiol. 2019;40:1–17. PMID: 30526699.
- Association for Professionals in Infection Control. Infection preventionist’s guide to the OR. https://apic.org/infection-preventionists-guide-to-the-or/. Published 2018. Accessed July 29, 2022.
- Berrios-Torres SI, Umscheid CA, Bratzler DW, et al. Centers for Disease Control and Prevention guideline for the prevention of surgical site infection, 2017. JAMA Surg. 2017;152:784–791. PMID: 28467526.
- American Society of Anesthesiologists. Infection control and prevention. https://www.asahq.org/shop-asa/e020s10w02. Published 2022. Accessed July 26, 2022.
- American Association of Nurse Anesthesiology. Infection prevention and control guidelines for anesthesia care. https://www.aana.com/docs/default-source/practice-aana-com-web-documents-(all)/professional-practice-manual/infection-prevention-and-control-guidelines-for-anesthesia-care.pdf?sfvrsn=850049b1. Published 2015. Accessed July 26, 2022.
- Menz BD, Charani E, Gordon DL, et al. Surgical antibiotic prophylaxis in an era of antibiotic resistance: common resistant bacteria and wider considerations for practice. Infect Drug Resist. 2021;14:5235–5252. PMID: 34908856.
- Dexter F, Epstein RH, Loftus RW. Quantifying and interpreting inequality of surgical site infections among operating rooms. Can J Anaesth. 2021;68:812–824. PMID: 33547628.
- Dexter F, Ledolter J, Wall RT, et al. Sample sizes for surveillance of S. aureus transmission to monitor effectiveness and provide feedback on intraoperative infection control including for COVID-19. Perioper Care Oper Room Manag. 2020;20:100115. PMID: 32501426.
- Loftus RW, Brown JR, Koff MD, et al. Multiple reservoirs contribute to intraoperative bacterial transmission. Anesth Analg. 2012;114:1236–1248. PMID: 22467892.
- Loftus RW, Dexter F, Robinson ADM, Horswill AR. Desiccation tolerance is associated with Staphylococcus aureus hypertransmissibility, resistance and infection development in the operating room. J Hosp Infect. 2018;100:299–308. PMID: 29966756.
- Loftus RW, Brown JR, Patel HM, et al. Transmission dynamics of gram-negative bacterial pathogens in the anesthesia work area. Anesth Analg. 2015;120:819–826. PMID: 25790209.
- Hadder B, Patel HM, Loftus RW. Dynamics of intraoperative Klebsiella, Acinetobacter, Pseudomonas, and Enterobacter transmission. Am J Infect Control. 2018;46:526–532. PMID: 29395508.
- Loftus RW, Muffly MK, Brown JR, et al. Hand contamination of anesthesia providers is an important risk factor for intraoperative bacterial transmission. Anesth Analg. 2011;112:98–105. PMID: 20686007.
- Rupp ME, Fitzgerald T, Puumala S, et al. Prospective, controlled, cross-over trial of alcohol-based hand gel in critical care units. Infect Control Hosp Epidemiol. 2008;29:8–15. PMID: 18171181.
- Koff MD, Brown JR, Marshall EJ, et al. Frequency of hand decontamination of intraoperative providers and reduction of postoperative healthcare-associated infections: a randomized clinical trial of a novel hand hygiene system. Infect Control Hosp Epidemiol. 2016;37:888–895. PMID: 27267310.
- Konvalinka A, Errett L, Fong IW. Impact of treating Staphylococcus aureus nasal carriers on wound infections in cardiac surgery. J Hosp Infect. 2006;64:162–168. PMID: 16930768.
- Wilson APR, Smyth D, Moore G, et al. The impact of enhanced cleaning within the intensive care unit on contamination of the near-patient environment with hospital pathogens: a randomized crossover study in critical care units in two hospitals. Crit Care Med. 2011;39:651–658. PMID: 21242793.
- Phillips M, Rosenberg A, Shopsin B, et al. Preventing surgical site infections: a randomized, open-label trial of nasal mupirocin ointment and nasal povidone-iodine solution. Infect Control Hosp Epidemiol. 2014;35:826–832. PMID: 24915210.
- Schweizer ML, Chiang HY, Septimus E, et al. Association of a bundled intervention with surgical site infections among patients undergoing cardiac, hip, or knee surgery. JAMA. 2015;313:2162–2171. PMID: 26034956.
- Bode LGM, Kluytmans JAJW, Wertheim HFL, et al. Preventing surgical-site infections in nasal carriers of Staphylococcus aureus. N Engl J Med. 2010;362:9–17. PMID: 20054045.
- Huang SS, Singh R, McKinnell JA, et al. Decolonization to reduce postdischarge infection risk among MRSA carriers. N Engl J Med. 2019;380:638–650. PMID: 30763195.
- von Eiff C, Becker K, Machka K, et al. Nasal carriage as a source of Staphylococcus aureus bacteremia. Study Group. N Engl J Med. 2001;344:11–16. PMID: 11136954.
- Kluytmans JA, Mouton JW, VandenBergh MF, et al. Reduction of surgical-site infections in cardiothoracic surgery by elimination of nasal carriage of Staphylococcus aureus. Infect Control Hosp Epidemiol. 1996;17:780–785. PMID: 8985763.
- Bhalla A, Aron DC, Donskey CJ. Staphylococcus aureus intestinal colonization is associated with increased frequency of S. aureus on skin of hospitalized patients. BMC Infect Dis. 2007;7:105. 17848192.
- Murray CJL, Ikuta KS, Sharara F, et al. Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399:629–655. PMID: 35065702.
- Laxminarayan R, Duse A, Wattal C, et al. Antibiotic resistance—the need for global solutions. Lancet Infect Dis. 2013;13:1057–1098. PMID: 24252483.
- Patel JB, Gorwitz RJ, Jernigan JA. Mupirocin resistance. Clin Infect Dis. 2009;49:935–941. PMID: 19673644.
- Houang ET, Gilmore OJ, Reid C, Shaw EJ. Absence of bacterial resistance to povidone iodine. J Clin Pathol. 1976;29:752–755. PMID: 821972.
- Bigliardi PL, Alsagoff SAL, El-Kafrawi HY, et al. Povidone iodine in wound healing: a review of current concepts and practices. Int J Surg. 2017;44:260–268. PMID: 28648795.
- Koff MD, Loftus RW, Burchman CC, et al. Reduction in intraoperative bacterial contamination of peripheral intravenous tubing through the use of a novel device. Anesthesiology. 2009;110:978–985. PMID: 19352154.
- Koff MD, Corwin HL, Beach ML, et al. Reduction in ventilator associated pneumonia in a mixed intensive care unit after initiation of a novel hand hygiene program. J Crit Care. 2011;26:489–495. PMID: 21439767.
- Rowlands J, Yeager MP, Beach M, et al. Video observation to map hand contact and bacterial transmission in operating rooms. Am J Infect Control. 2014;42:698–701. PMID: 24969122.
- Bischoff WE, Reynolds TM, Sessler CN, et al. Handwashing compliance by health care workers: The impact of introducing an accessible, alcohol-based hand antiseptic. Arch Intern Med. 2000;160:1017–1021. PMID: 10761968.
- Birnbach DJ, Rosen LF, Fitzpatrick M, et al. Double gloves: a randomized trial to evaluate a simple strategy to reduce contamination in the operating room. Anesth Analg. 2015;120:848–852. PMID: 24836472.
- Clark C, Taenzer A, Charette K, Whitty M. Decreasing contamination of the anesthesia environment. Am J Infect Control. 2014;42:1223–1225. PMID: 25444268.
- Boyce JM, Pittet D, Healthcare Infection Control Practices Advisory Committee. Society for Healthcare Epidemiology of America. Association for Professionals in Infection Control. Infectious Diseases Society of America. Hand Hygiene Task F. Guideline for hand hygiene in health-care settings: recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Infect Control Hosp Epidemiol. 2002;23:S3–40. PMID: 12515399.
- Loftus RW, Patel HM, Huysman BC, et al. Prevention of intravenous bacterial injection from health care provider hands: the importance of catheter design and handling. Anesth Analg. 2012;115:1109–1119. PMID: 23051883.
- Loftus RW, Brindeiro BS, Kispert DP, et al. Reduction in intraoperative bacterial contamination of peripheral intravenous tubing through the use of a passive catheter care system. Anesth Analg. 2012;115:1315–1323. PMID: 23144441.
- Greene ES. Challenges in reducing the risk of infection when accessing vascular catheters. J Hosp Infect. 2021;113:130–144. PMID: 33713758.
- Moureau NL, Flynn J. Disinfection of needleless connector hubs: clinical evidence systematic review. Nurs Res Pract. 2015;2015:796762. PMID: 26075093.
- Lamberg JJ YL. Swab all vials with alcohol. APSF Newsletter. https://www.apsf.org/article/swab-all-vials-with-alcohol/. Published 2012. Accessed July 26, 2022.
- Bennett SN, McNeil MM, Bland LA, et al. Postoperative infections traced to contamination of an intravenous anesthetic, propofol. N Engl J Med. 1995;333:147–154. PMID: 7791816.
- Centers for Disease Control and Infection Prevention. Checklist for prevention of central line associated blood stream infections. https://www.cdc.gov/HAI/pdfs/bsi/checklist-for-CLABSI.pdf. Published 2014. Accessed July 26, 2022.
- Agency for Healthcare Research and Quality. Central line-associated bloodstream infections (CLABSI). https://www.ahrq.gov/topics/central-line-associated-bloodstream-infections-clabsi.html. Published 2022. Accessed July 26, 2022.
- Loftus RW, Koff MD, Burchman CC, et al. Transmission of pathogenic bacterial organisms in the anesthesia work area. Anesthesiology. 2008;109:399–407. PMID: 18719437.
- Robinson ADM, Dexter F, Renkor V, et al. Operating room PathTrac analysis of current intraoperative Staphylococcus aureus transmission dynamics. Am J Infect Control. 2019;47:1240–1247. PMID: 31036398.
- Loftus RW, Dexter F, Evans LC, et al. An assessment of the impact of recommended anesthesia work area cleaning procedures on intraoperative SARS-CoV-2 contamination, a case-series analysis. J Clin Anesth. 2021;73:110350. PMID: 34098391.
- Birchansky B, Dexter F, Epstein RH, Loftus RW. Statistical design of overnight trials for the evaluation of the number of operating rooms that can be disinfected by an ultraviolet light disinfection robotic system. Cureus. 2021;13:e18861. PMID: 34804714.
