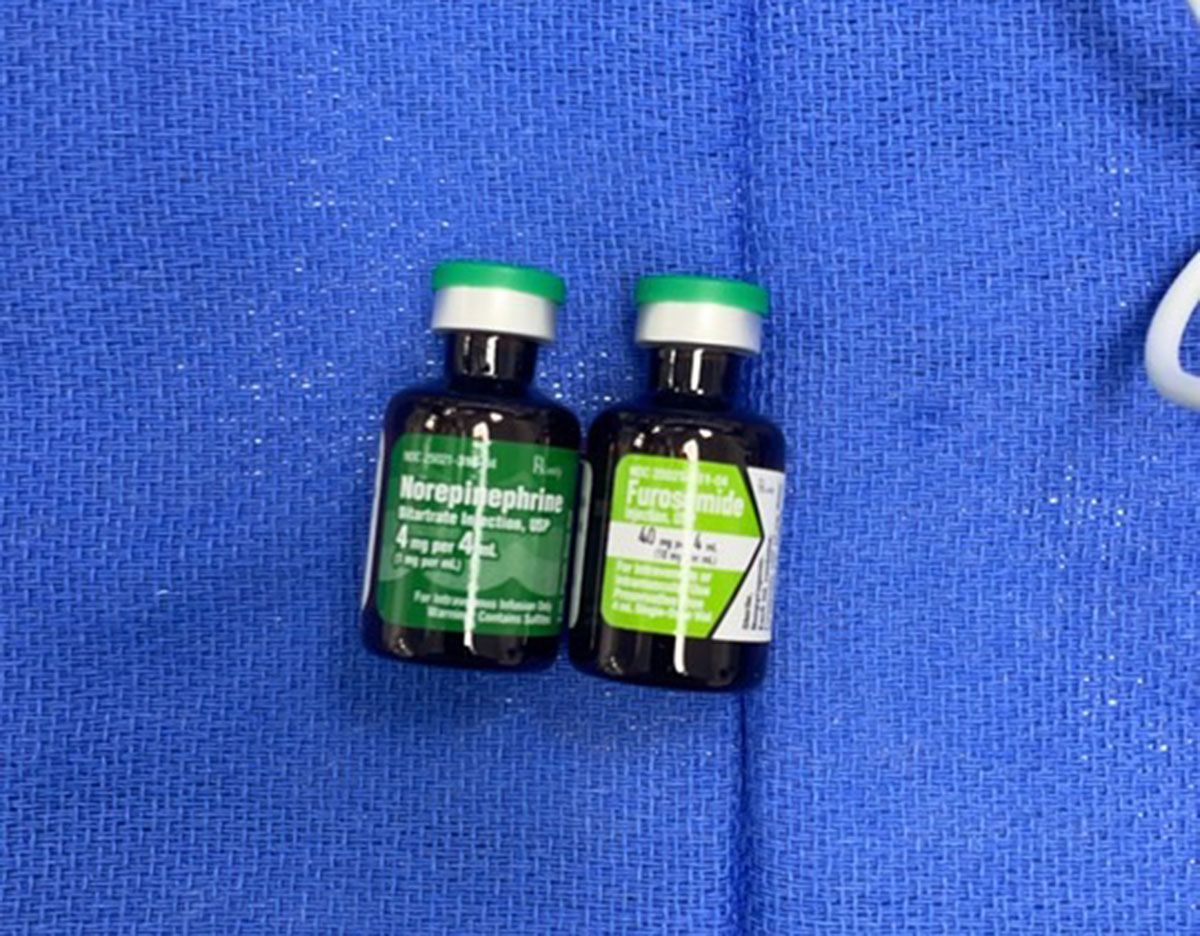
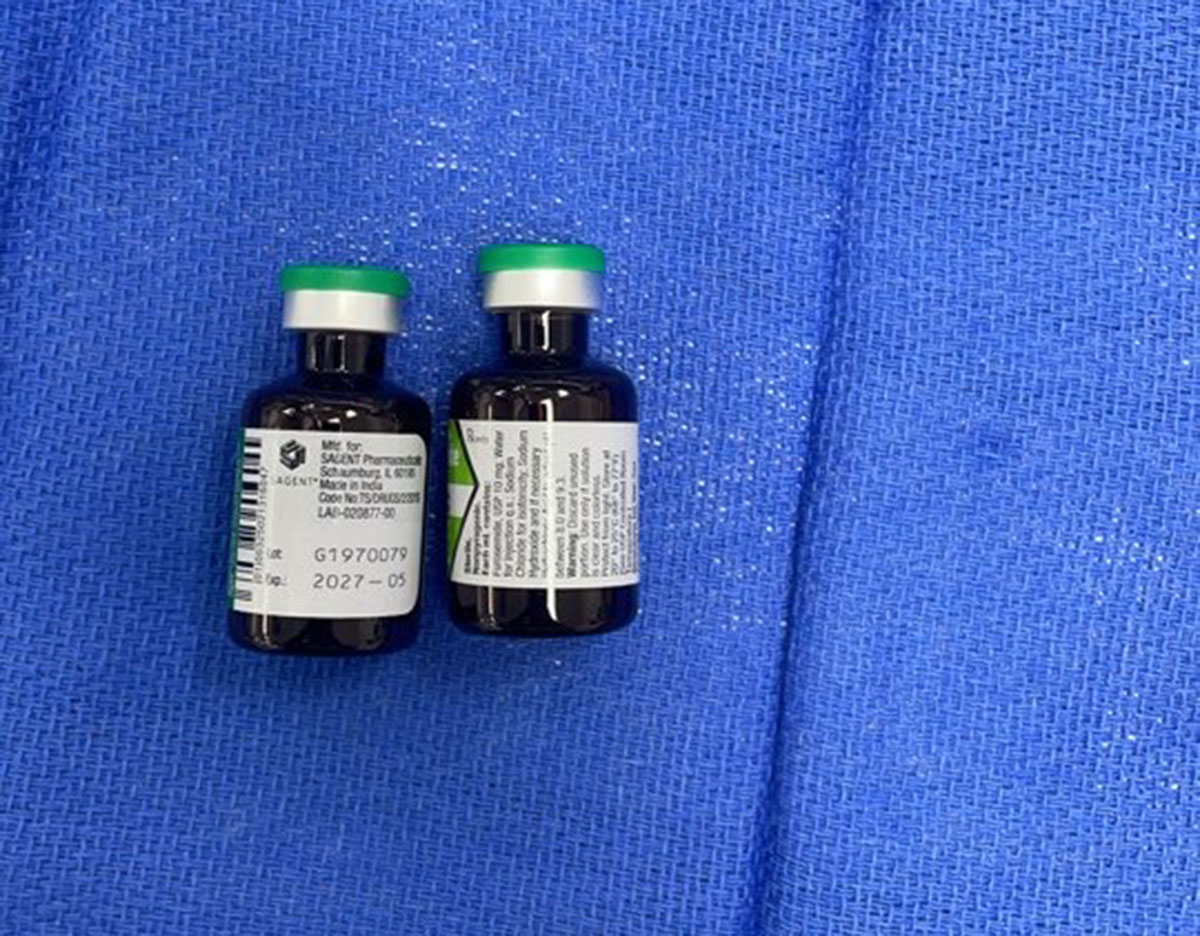
Very resembling Furosemide and Norepipnephrine, you don’t really want to use one when you need the other.
Furosemide, Norepipnephrine
Furosemide, Norepipnephrine
Submitted by Yonathan Delouya, MD
Jackson Memorial Hospital, Miami, FL
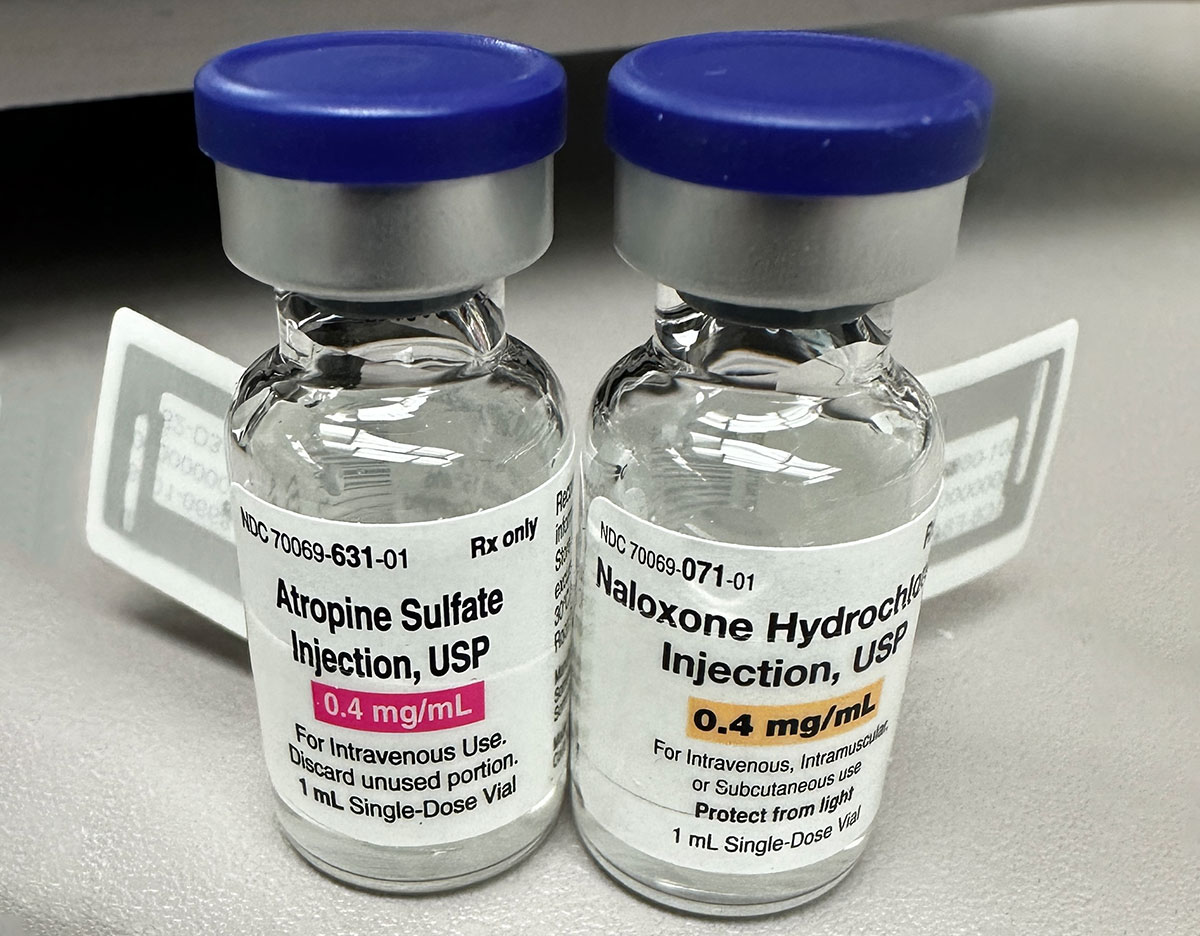
Atropine Sulfate, Naloxone Hydrochloride July 27, 2026
This is the most similar Look-Alike pair I have personally seen in my whole career. Thank you for letting others know!
Atropine Sulfate, Naloxone Hydrochloride
Submitted by Mark Gjolaj, MD, MBA
Kaiser Permanente
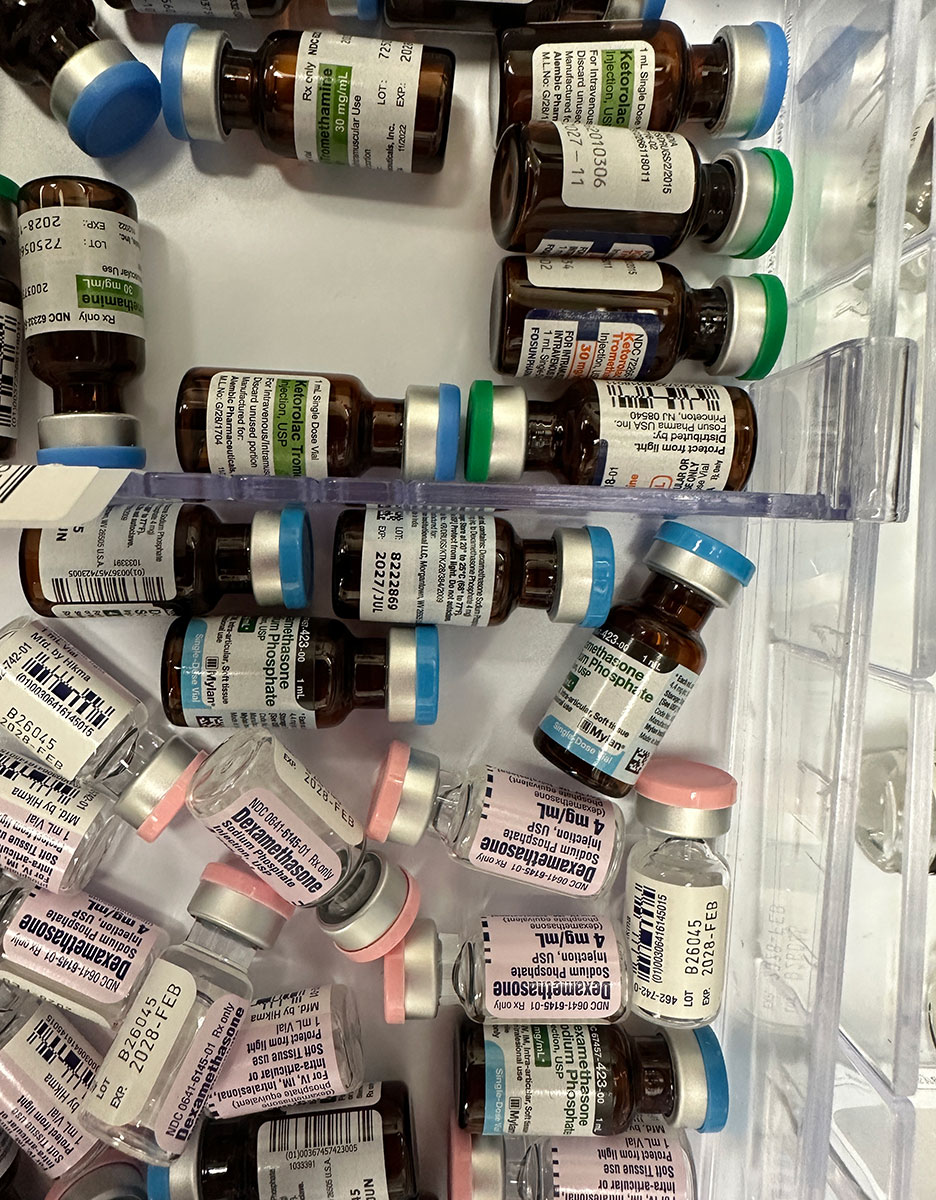
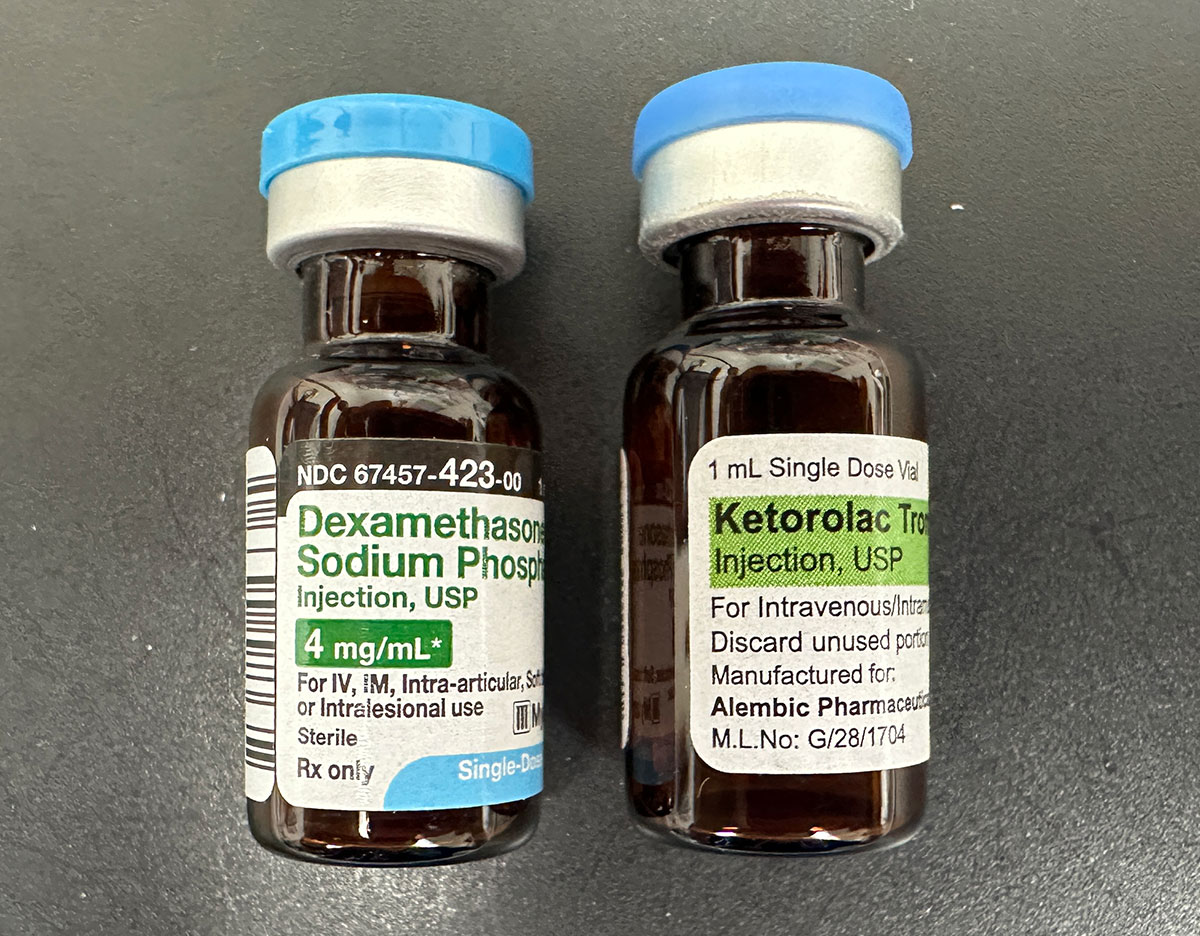
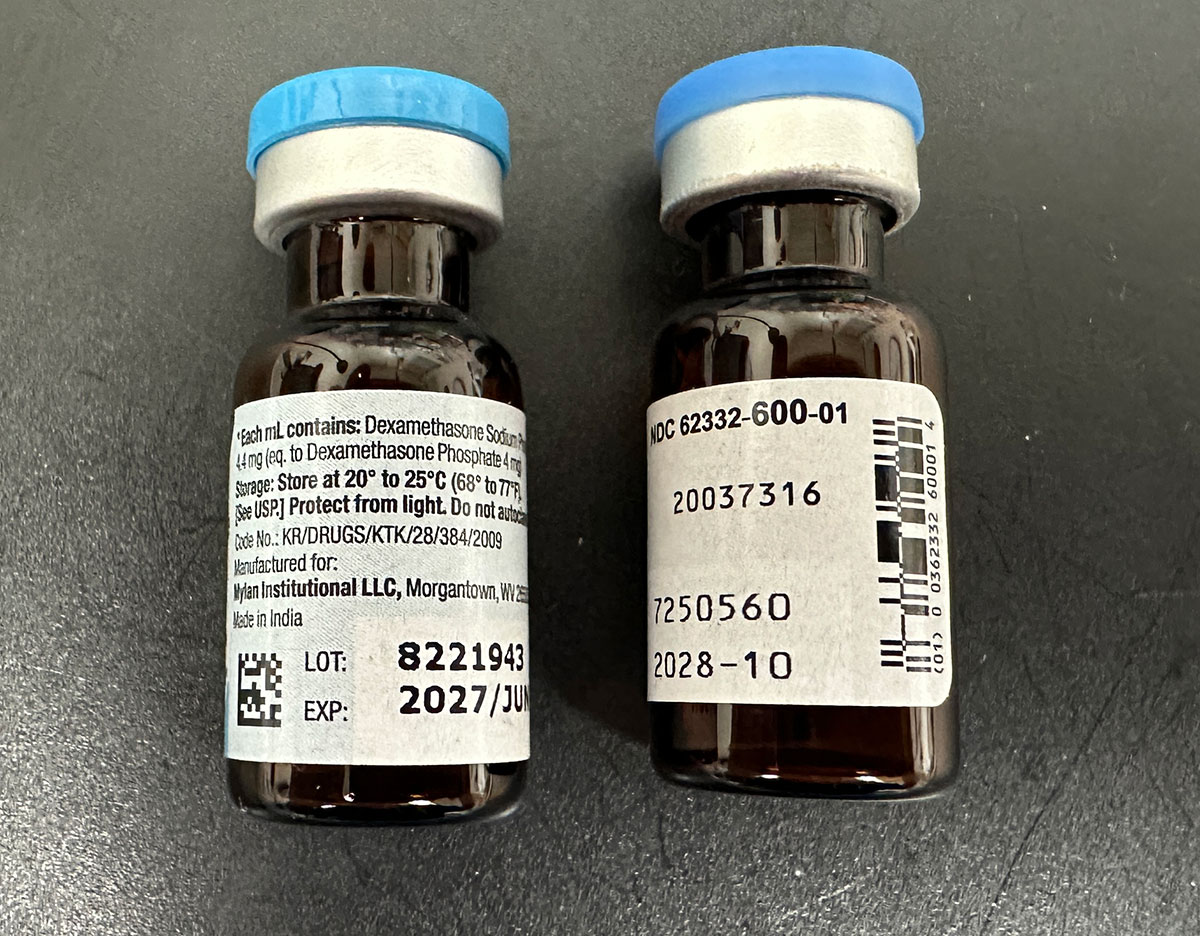
Ketorolac, Dexamethasone July 12, 2026
Strikingly similar ketorolac and dexamethasone vials in adjacent medication bins.
Vials Bin – Ketorolac, Dexamethasone
Vials Front – Ketorolac, Dexamethasone
Vials Back – Ketorolac, Dexamethasone
Submitted by Hedwig Schroeck, MD, FAAP
Dartmouth Health, Lebanon, New Hampshire, USA
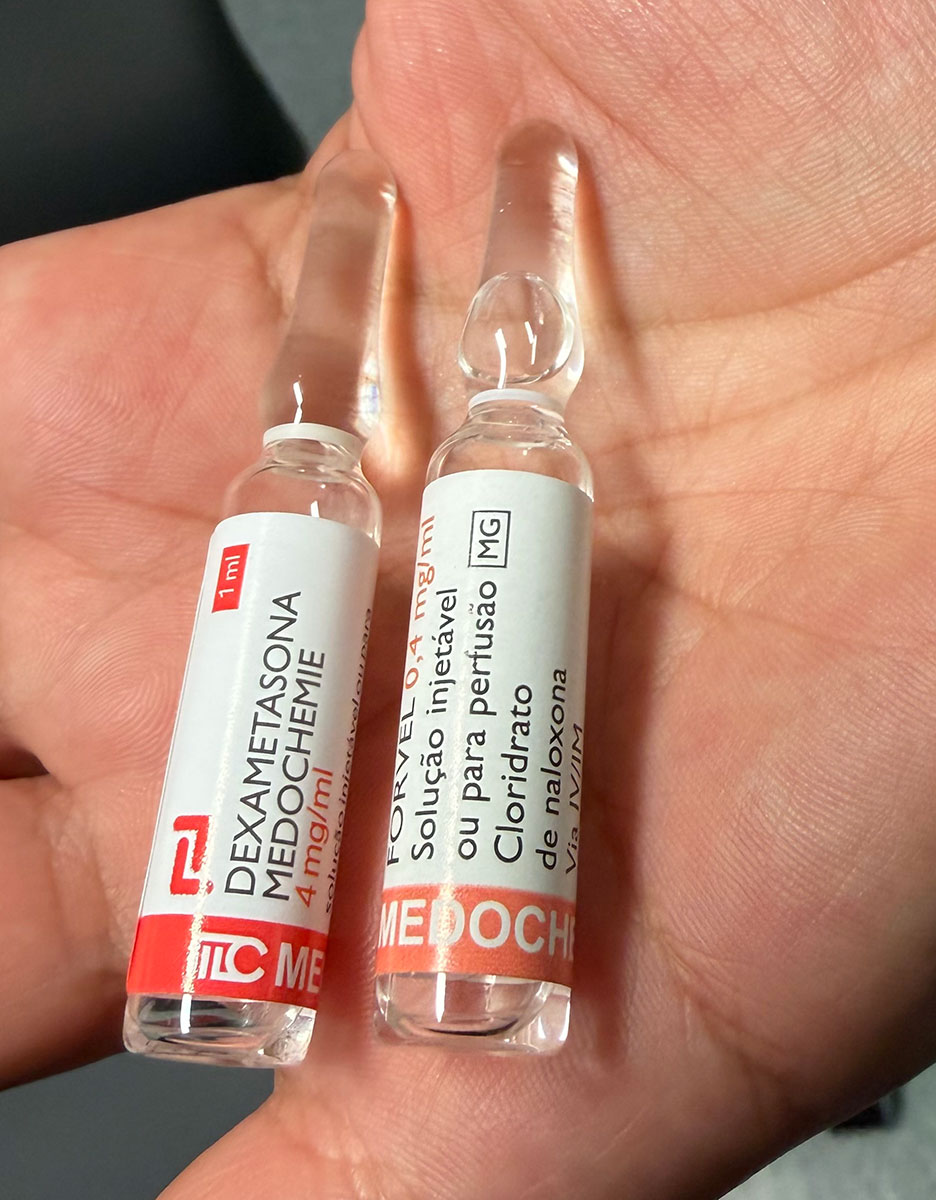
Dexamethasone, Naloxone June 12, 2026
The vial of dexamethasone and naloxone are much alike
Dexamethasone, Naloxone
Submitted by Ana Margarida zeferino de Sousa Gaspar
Instituto português de oncologia de Lisboa, Francisco gentil
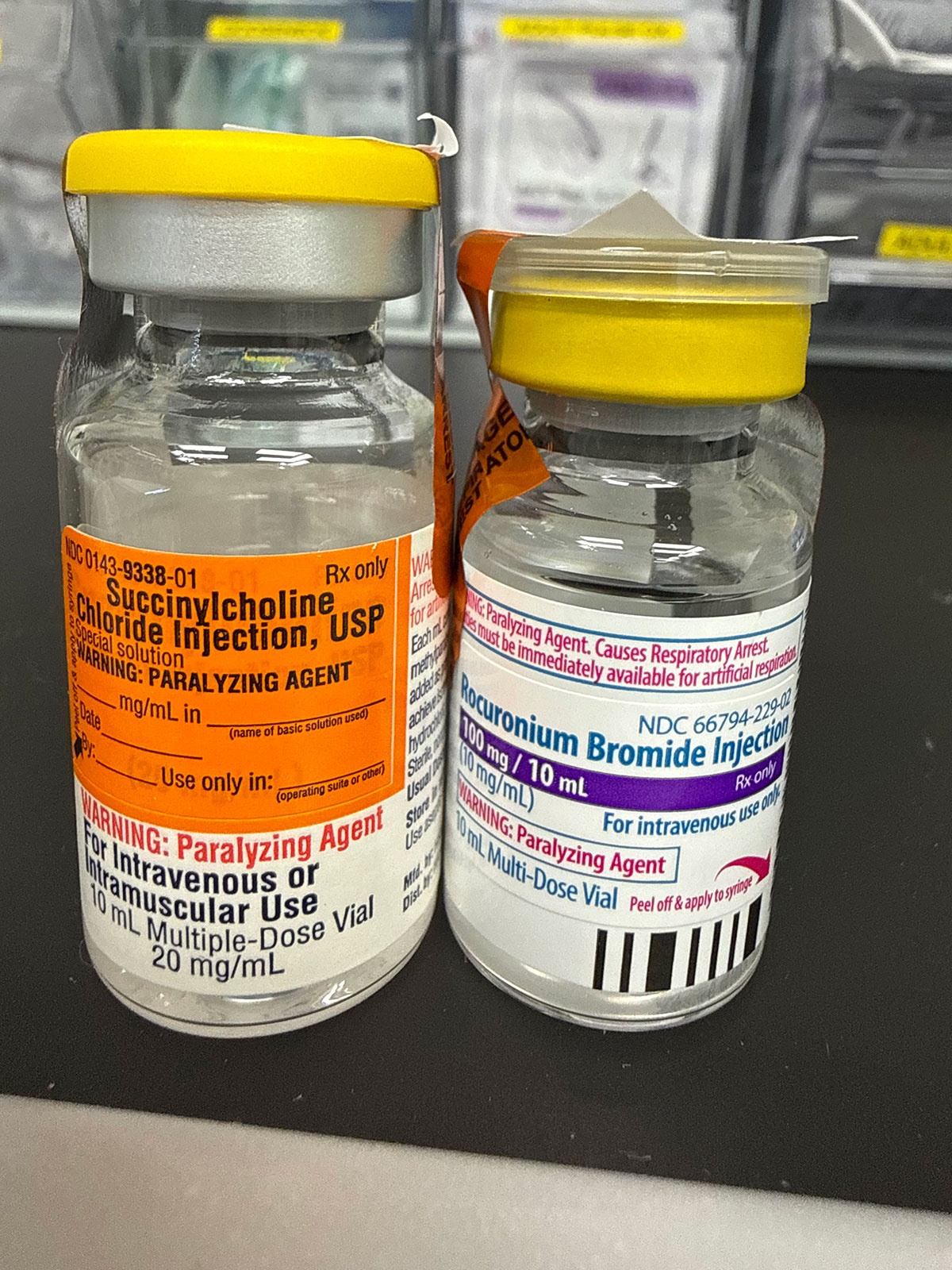
Succinylcholine, Rocuronium Bromide April 3, 2026
These two paralytics have distinct mechanisms of action, durations, and contraindications, thus their vials should have well established visual differences. Accidental vial swaps of these two medications could potentially be catastrophic.
Succinylcholine, Rocuronium Bromide
Submitted by Jeremy Grayson
St. Joseph’s University Medical Center Paterson, NJ
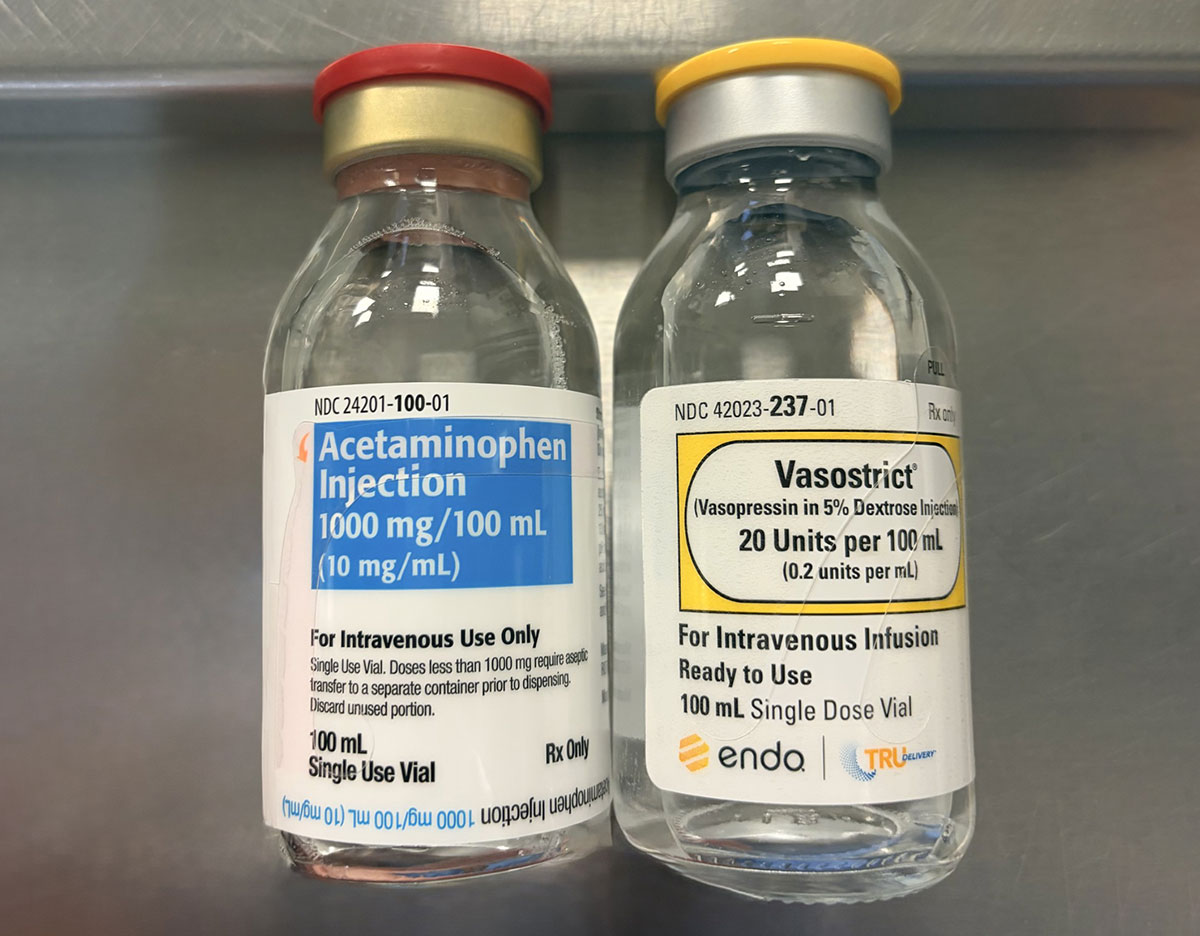
Vasopressin, Acetaminophen February 13, 2026
Mix-ups between IV acetaminophen and vasopressin have occurred due to their similar presentation, leading to an incident in which patients intended to receive vasopressin received IV acetaminophen instead.
Vasopressin, Acetaminophen
Submitted by Bruna Maria Castro de Oliveira, MD
Massachusetts General Hospital
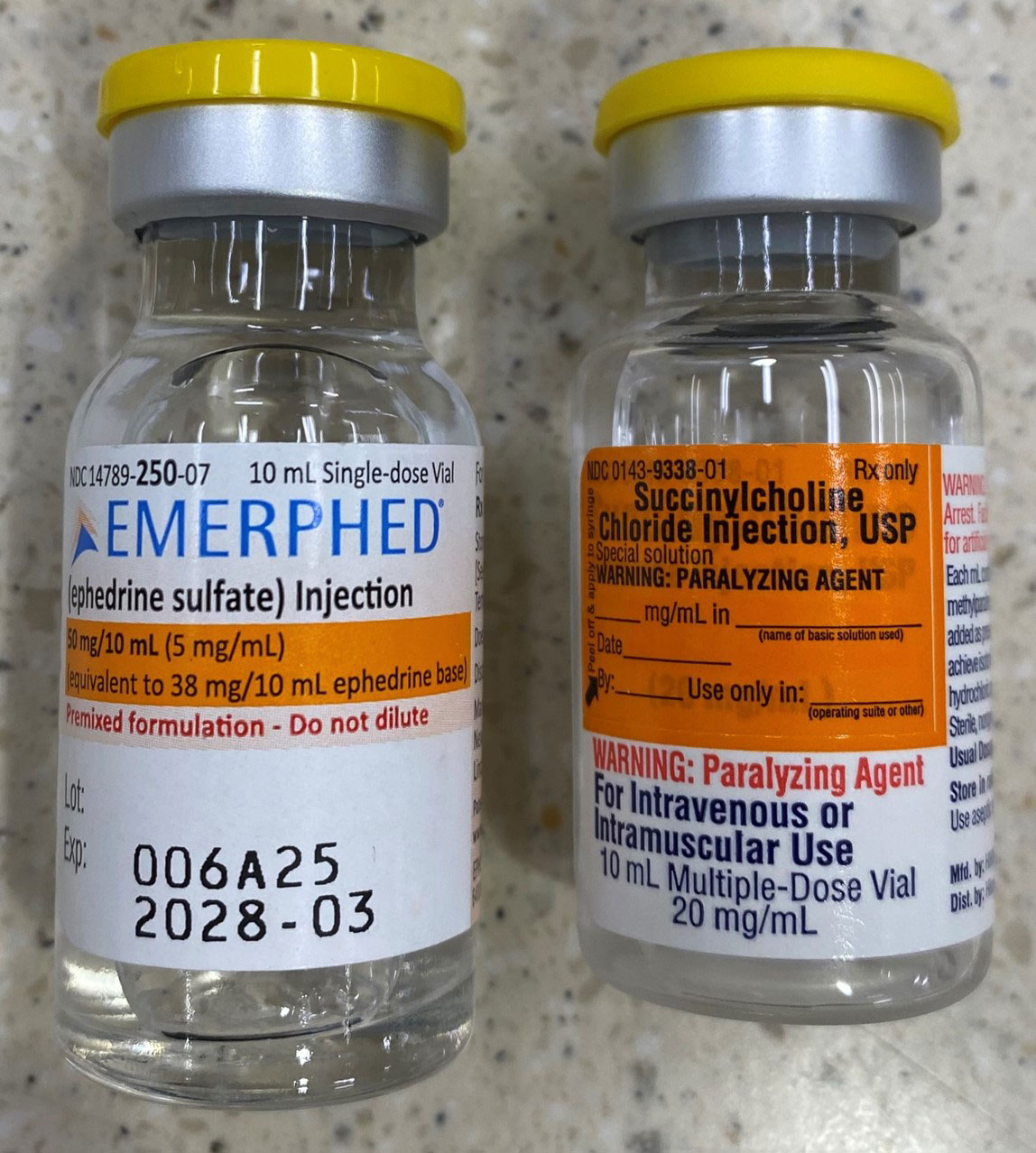
Succinylcholine, Ephedrine December 31, 2025
Succinylcholine vials made by Hikma (NDC: 0143-9338-25) have a yellow cap, which is a departure from the unofficial standard practice of using red caps for succinylcholine.
These yellow-capped succinylcholine vials with orange labeling are strikingly similar to ephedrine vials, as shown in the attached photo.
Succinylcholine, Ephedrine
Submitted by Perry Shafner, PharmD
Greater Baltimore Medical Center
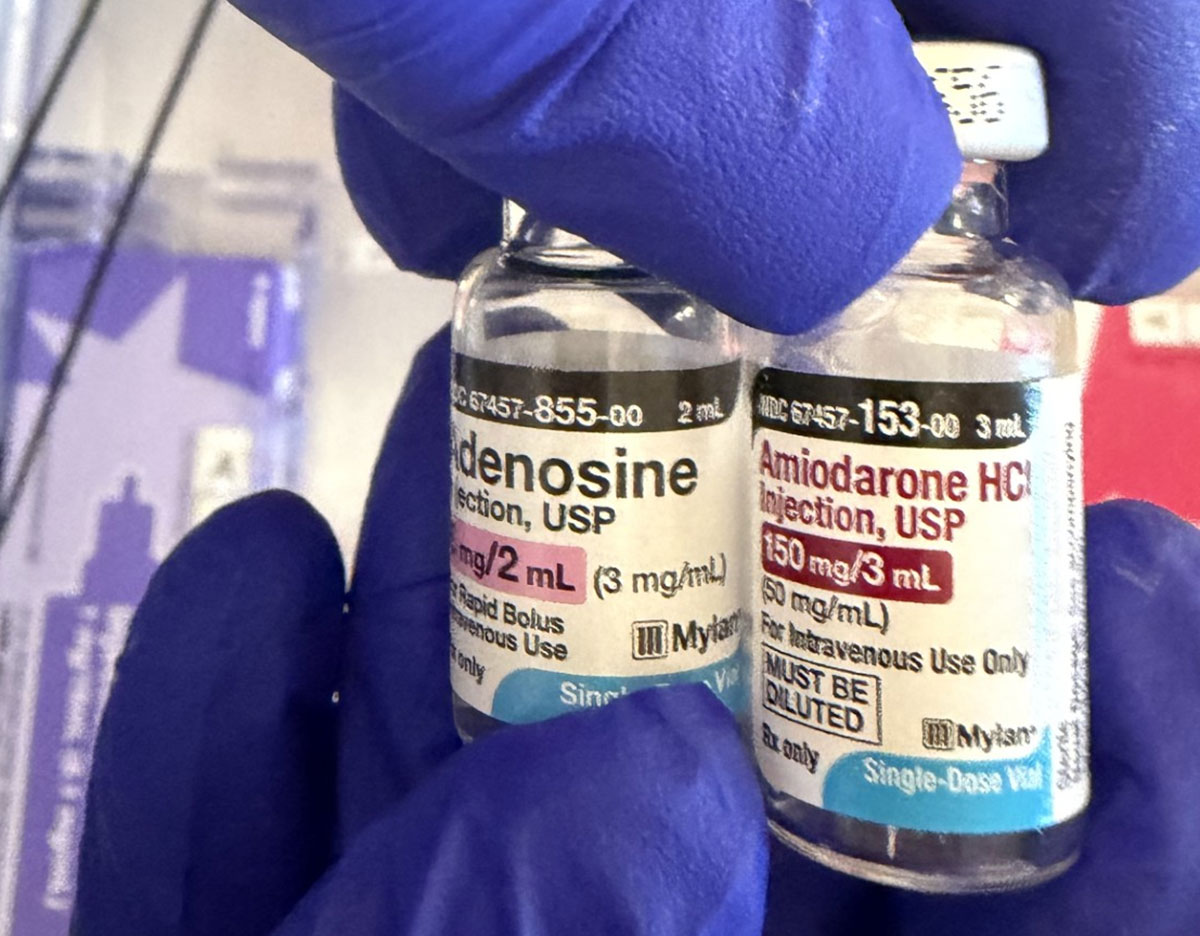
Adenosine, Amiodarone December 29, 2025
These two vials of Adenosine and Amiodarone were stored next to each other in a crash cart. The adenosine manufacturer was recently updated, resulting in the look-alike packaging. Adenosine was pulled in error during a code blue, but the error was detected before reaching the patient.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of all cookies. However you may visit Cookie Settings to provide a controlled consent.
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Cookie
Description
PHPSESSID
This cookie is native to PHP applications. The cookie is used to store and identify a users' unique session ID for the purpose of managing user session on the website. The cookie is a session cookies and is deleted when all the browser windows are closed.
viewed_cookie_policy
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
__stripe_mid
This cookie is set by Stripe payment gateway. This cookie is used to enable payment on the website without storing any payment information on a server.
__stripe_sid
This cookie is set by Stripe payment gateway. This cookie is used to enable payment on the website without storing any payment information on a server.
_wpfuuid
This cookie is used by the WPForms WordPress plugin. The cookie is used to allow the paid version of the plugin to connect entries by the same user and is used for some additional features like the Form Abandonment addon.
__cfduid
The cookie is set by CloudFare. The cookie is used to identify individual clients behind a shared IP address and apply security settings on a per-client basis. It does not correspond to any user ID in the web application and does not store any personally identifiable information.
Analytics cookies help us understand how our visitors interact with the website. It helps us understand the number of visitors, where the visitors are coming from, and the pages they navigate. The cookies collect this data and are reported anonymously.
Cookie
Description
GPS
This cookie is set by Youtube and registers a unique ID for tracking users based on their geographical location
_ga
This cookie is installed by Google Analytics. The cookie is used to calculate visitor, session, campaign data and keep track of site usage for the site's analytics report. The cookies store information anonymously and assign a randomly generated number to identify unique visitors.
_gid
This cookie is installed by Google Analytics. The cookie is used to store information of how visitors use a website and helps in creating an analytics report of how the website is doing. The data collected including the number visitors, the source where they have come from, and the pages visited in an anonymous form.
Collects anonymous data about how visitors use our site and how it performs. We use this to improve our products, services and user experience.
Cookie
Description
YSC
This cookies is set by Youtube and is used to track the views of embedded videos.
__utmz
This cookie is set by Google analytics and is used to store the traffic source or campaign through which the visitor reached your site.
__utmb
The cookie is set by Google Analytics. The cookie is used to determine new sessions/visits. The cookie is created when the JavaScript library executes and there are no existing __utma cookies. The cookie is updated every time data is sent to Google Analytics.
__utma
This cookie is set by Google Analytics and is used to distinguish users and sessions. The cookie is created when the JavaScript library executes and there are no existing __utma cookies. The cookie is updated every time data is sent to Google Analytics.
__utmc
The cookie is set by Google Analytics and is deleted when the user closes the browser. The cookie is not used by ga.js. The cookie is used to enable interoperability with urchin.js which is an older version of Google analytics and used in conjunction with the __utmb cookie to determine new sessions/visits.
_gat
This cookies is installed by Google Universal Analytics to throttle the request rate to limit the colllection of data on high traffic sites.
Advertisement cookies help us provide our visitors with relevant ads and marketing campaigns.
Cookie
Description
VISITOR_INFO1_LIVE
This cookie is set by Youtube. Used to track the information of the embedded YouTube videos on a website.
IDE
Used by Google DoubleClick and stores information about how the user uses the website and any other advertisement before visiting the website. This is used to present users with ads that are relevant to them according to the user profile.
NID
This cookie is used to a profile based on user's interest and display personalized ads to the users.










































, Calcium Chloride")







, Sodium Chloride")
























 4mg 2mL vial. Look-alike with blue tops.")
, Phenylephrine, Lidocaine and dexamethasone.")
 4mg 2mL vial drawer. This is from a different institution than Figure 1. Look-alike with blue tops.")
, Ondansetron (Zofran ®) 4 mg/2mL, and metoclopramide vial look-alike with similar green tops.")

 4mg 2mL vial and Atropine sulfate 1mg/mL vials. Look-alike with blue tops.")


