Drawing on firsthand experience during the Continuing Promise 2025 humanitarian mission aboard the USNS Comfort, patient-safety implications of reusable versus single-use airway devices in resource-limited settings are examined. Reusable rigid stylets were found to lose reliability after repeated sterilization, complicating unexpected difficult airways. Single-use devices performed more consistently but raised challenges related to waste, supply reliability, and cost, supporting the need for hybrid airway strategies in humanitarian settings.
The provision of safe anesthesia in resource-constrained humanitarian settings requires careful consideration of equipment selection, balancing clinical efficacy with logistical constraints and environmental stewardship. Continuing Promise, a recurring humanitarian mission that began in 2007, aims to provide medical assistance throughout the Caribbean, Central, and South America. During the 16th iteration of this mission, our anesthesia team aboard the USNS Comfort confronted a fundamental question with significant patient safety implications: Should airway equipment prioritize reusable or single-use devices?
This decision extends beyond simple cost considerations. In humanitarian anesthesia, equipment choices intersect with infection control protocols, environmental sustainability, supply chain reliability, and the long-term impact on host communities. As global health initiatives expand, this issue merits careful examination through the lens of patient safety and ethical practice.
SUSTAINABILITY AND ETHICAL CONSIDERATIONS
Humanitarian anesthesia must reconcile immediate patient safety requirements with long-term environmental and ethical responsibilities. Single-use devices may offer superior performance, consistency, and simplified infection control, but also contribute to environmental impacts and strain local waste management systems. Single use laryngoscope handles alone contribute 16–25 times more greenhouse gas emissions when compared to their reusable counterparts.1 Conversely, reusable equipment reduces waste generation but may compromise safety due to sterilization limitations and performance degradation.
The ethical imperative extends beyond immediate patient care to encompass our responsibility to host communities. Exporting unsustainable care models that burden local systems with unmanageable medical waste undermines humanitarian principles and long-term relationships.
AIRWAY EQUIPMENT CONSIDERATIONS IN HUMANITARIAN SETTINGS
Modern airway management tools, including laryngoscopes, video laryngoscopes, and rigid stylets, are available in both reusable and disposable configurations. While U.S. hospitals typically base equipment decisions on infection control policies, institutional preference, or cost-effectiveness, humanitarian deployments present a fundamentally different calculus involving availability, durability, sterilization capacity, and waste management.2
REUSABLE EQUIPMENT: DURABILITY AND STERILIZATION ISSUES
Our experience with reusable GlideRite® stylets revealed significant concerns regarding durability and performance consistency. Multiple sterilization cycles and routine handling led to progressive deformation, rendering stylets difficult or impossible to use effectively. During two unanticipated difficult airway scenarios, we were compelled to switch from reusable to single-use stylets mid-procedure—a delay that could compromise patient safety in time-critical situations.
Utilizing measurement standards similar to those described previously,3 our team documented significant curvature variations between least and most deformed reusable stylets. Our single-use stylets demonstrated consistent handle-to-tip angles averaging 14.92 degrees. In contrast, our 10 reusable stylets showed significant variation, ranging from 10.52 degrees (straighter) to 19.28 degrees (more curved), with statistical significance (p < 0.0001) (Figures 1 and 2). This corresponded to tip location differences ranging from -19 mm to +31.8 mm when compared to a new single-use stylet baseline. Considering that the average adult male glottis measures 21.5 mm in anteroposterior width,4 these variations represent clinically significant deviations—potentially displacing the stylet tip by nearly two glottic widths in either direction.
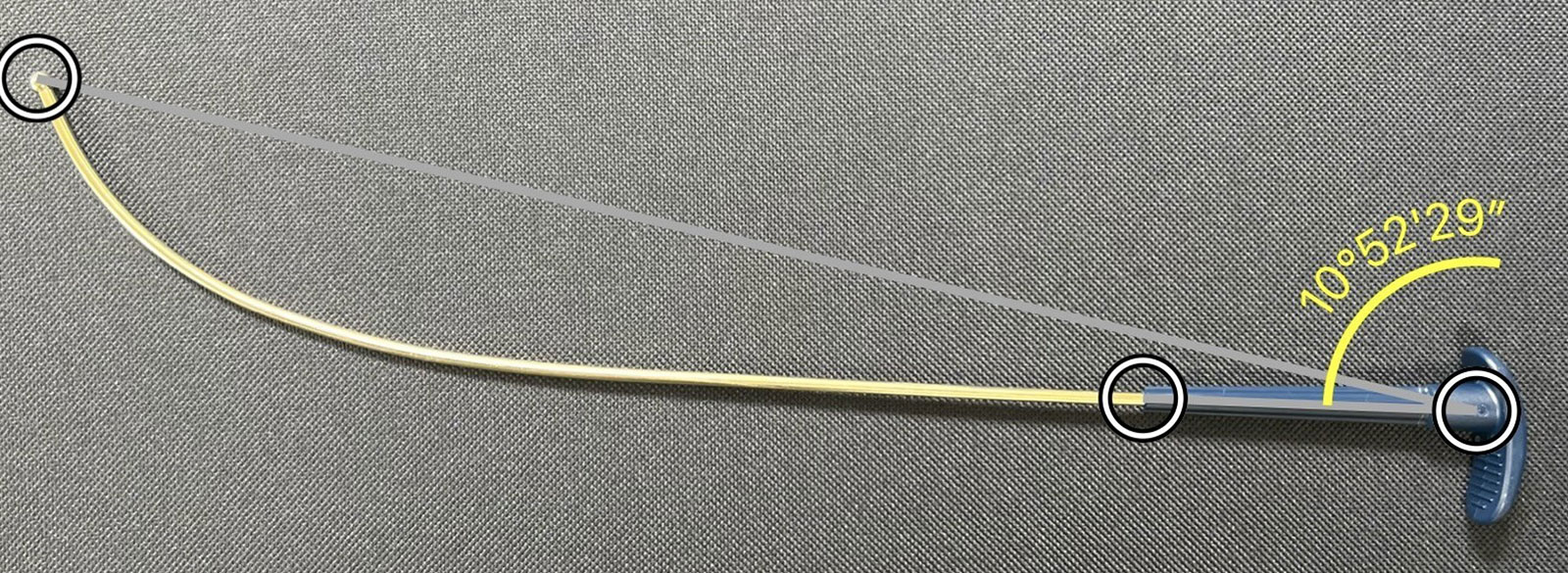
Figure 1: Measurement methodology showing handle to tip angulation to quantify deformation of reusable stylets.
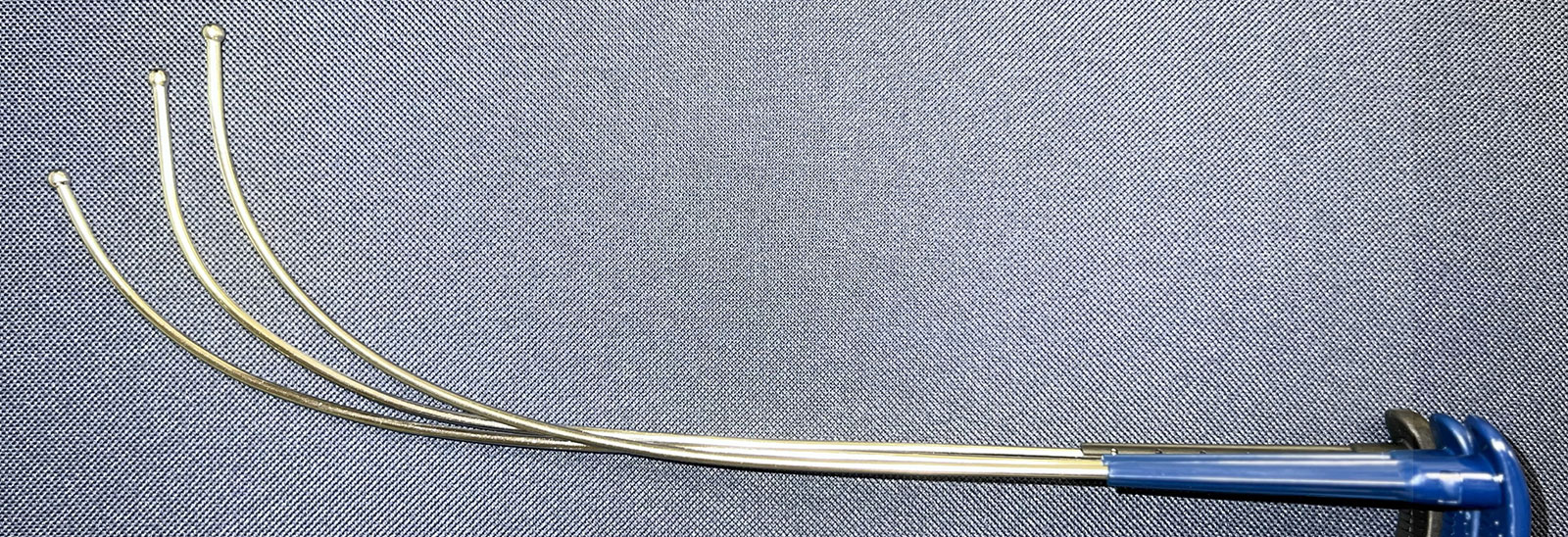
Figure 2: Comparison of single-use stylet with two reusable stylets showing varying degrees of curvature deformation.
These distortions posed significant risks to our ability to deliver safe and efficient care, particularly when managing complex airways. Despite stringent preoperative screening to avoid anticipated difficult airways, we encountered unanticipated difficult airway scenarios that required immediate equipment changes. The unreliability of deformed reusable equipment in these critical moments highlighted how equipment failure can directly compromise patient safety when seconds matter.
STERILIZATION INFRASTRUCTURE LIMITATIONS
Reusable direct laryngoscope blades required nightly reprocessing to ensure adequate supply for the following day’s cases. While manageable with our 3–4 operating rooms, any increase in surgical volume could have resulted in anesthesia delays: an unacceptable compromise to patient safety and operational efficiency, potentially impacting the number of cases that could be accomplished in the humanitarian mission.
Centralized sterilization processes can create additional vulnerabilities, including equipment maintenance issues, interdepartmental backlogs, and environmental control problems affecting storage conditions.4 These bottlenecks forced airway management planning around sterilizer availability rather than patient needs.
SINGLE-USE EQUIPMENT: PERFORMANCE AND ENVIRONMENTAL TRADE-OFFS
Clinical Advantages
Single-use GlideScope® stylets demonstrated consistent performance, maintained their designed curvature, and provided immediate readiness—particularly valuable during emergency airway management. The absence of disposable direct laryngoscope blades represented a missed opportunity to eliminate performance degradation and reprocessing delays.
Waste Management Challenges
The environmental impact of single-use devices became immediately apparent in the shipboard setting. Waste segregation, separating plastic from paper and metal components, was mandatory for proper disposal. Many host nations required meticulous waste separation as a prerequisite for acceptance, and robust disposal infrastructure was challenging to achieve.
To minimize environmental impact, we utilized the shipboard incinerator for paper products whenever possible. However, the accumulation of medical-grade plastics created both logistical challenges and ethical concerns, particularly when operating in communities ill-equipped to manage such waste streams.
Supply and Cost Limitations
Single-use disposable equipment is preferentially affected by supply chain issues. Despite extensive predeployment planning, our single-use videolaryngoscope blades arrived only days before departure for the three-month mission. The absence of reusable backup systems created unnecessary predeployment stress and highlighted a critical principle: availability supersedes preference in austere environments. Equipment that may be considered outdated in well-resourced facilities becomes invaluable if it is immediately available and sterilizable.
Midmission depletion of disposable stylets could force reliance on compromised reusable equipment, demonstrating the vulnerability inherent in single-source supply strategies. This underscores the critical importance of redundant equipment planning in austere environments. In a cost-conscious humanitarian setting, reusable airway equipment may offer up to a 10-fold cost reduction5 over the course of multiple humanitarian missions.
EVIDENCE-BASED RECOMMENDATIONS
Based on our experience and existing literature, we propose the following patient safety-focused strategies:
1. Hybrid Equipment Strategy
Maintain both reusable and single-use options for critical airway tools. This approach provides operational flexibility to respond to case complexity variations, sterilization delays, and supply chain disruptions while maintaining consistent patient safety standards.
2. Enhanced Equipment Monitoring Protocols
Implement systematic inspection protocols for reusable devices, such as rigid stylets prone to deformation. Staff training should emphasize recognition of subtle performance degradation that may not be visually apparent but could compromise clinical effectiveness.
3. Redundant Supply Chain Planning
Build significant cushion into equipment procurement, particularly for single-use devices. When primary supplies are depleted, alternative equipment options ensure continuity of safe care without compromising clinical standards.
4. Pre-Deployment Waste Management Planning
Coordinate with host nations regarding waste acceptance and disposal capabilities before deployment. Establish agreements for proper medical waste handling that minimize environmental impact while ensuring compliance with local regulations.
CONCLUSION
Airway management in humanitarian settings extends beyond technical proficiency to encompass systems thinking, environmental stewardship, and ethical responsibility. The choice between reusable and single-use equipment cannot be reduced to a binary decision but requires nuanced evaluation of clinical requirements, local context, and long-term impact.
Continuing Promise 2025 reinforced that every clinical decision—from stylet selection to waste disposal—carries implications extending far beyond the immediate patient encounter. As the global health community continues to expand humanitarian efforts, anesthesia professionals must lead in developing solutions that protect both individual patients and the communities we serve.
The path forward requires continued dialogue between clinical practitioners, equipment manufacturers, and global health organizations to develop sustainable solutions that prioritize patient safety without compromising environmental responsibility. Our commitment to “First, do no harm” must encompass not only the patient on the operating table but also the world we leave behind.
LCDR Matthew McGee, MD, MC, USN, is an assistant professor of anesthesiology at the Uniformed Services University of Health Sciences, Bethesda, MD, USA.
Matthew McGee reports no conflicts of interest.
Disclaimer: The views expressed in this article are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government.
Copyright Statement: I am a military service member. This work was prepared as part of my official duties. Title 17 U.S.C. 105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a United States Government work as a work prepared by a military service member or employee of the United States Government as part of that person’s official duties.
REFERENCES
- Sherman JD, Raibley LA IV, Eckelman MJ. Life cycle assessment and costing methods for device procurement: comparing reusable and single-use disposable laryngoscopes. Anesth Analg. 2018;127:434–443. PMID: 29324492
- Sherman J. Reusable vs. disposable laryngoscopes. APSF Newsletter. 2019;33:91. https://www.apsf.org/article/reusable-vs-disposable-laryngoscopes/ Accessed August 1, 2025.
- Smith CR, Urdaneta F, Gravenstein N. Use-dependent curvature changes in the GlideRite® Reusable Intubation Stylet. A A Case Reports. 2016;6:299–304. PMID: 27075422
- Randestad A, Lindholm CE, Fabian P. Dimensions of the cricoid cartilage and the trachea. Laryngoscope. 2000;110:1957–1961. PMID: 1108161
- Sherman JD, Hopf HW. Balancing infection control and environmental protection as a matter of patient safety: the case of laryngoscope handles. Anesth Analg. 2018;127:576-–579. PMID: 29324490
