Given the resurgence of measles and its highly contagious nature, perioperative teams must prioritize early identification and strict adherence to airborne precautions. strategies for managing patients with suspected or confirmed measles are suggested, emphasizing that elective procedures should be postponed until the infectious period has passed to protect both staff and the broader patient population.
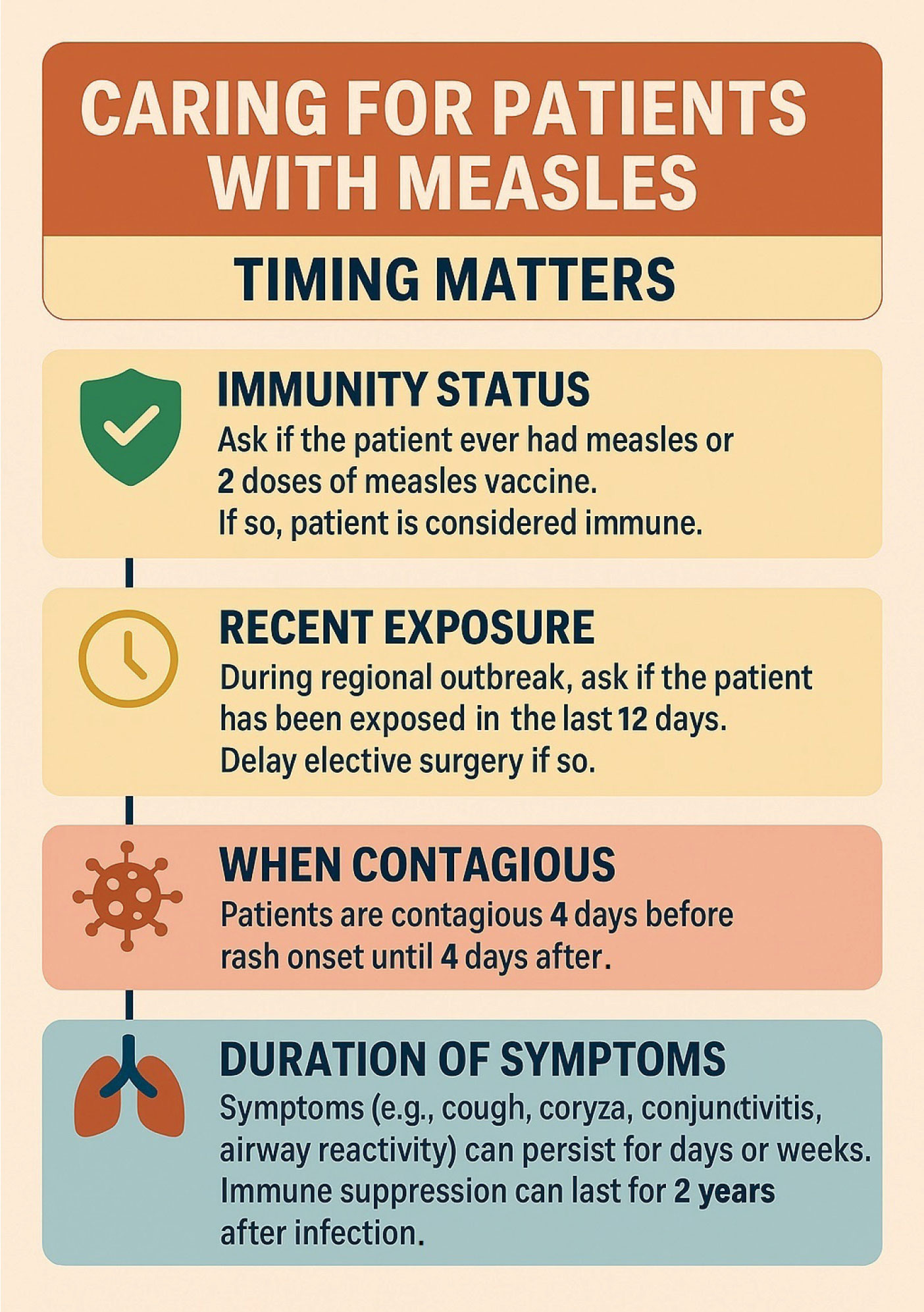
Figure 1: Measles Timing Facts. Created with the assistance of Microsoft Copilot.
Measles, also called rubeola, is a highly contagious viral illness caused by a paramyxovirus from the genus Morbillivirus. It is recognized as one of the most transmissible viruses, spreading easily through respiratory droplets, aerosols, or direct contact with bodily secretions. Following exposure, symptoms such as fever, cough, coryza, and conjunctivitis generally develop within 7 to 14 days, with an incubation period typically lasting 11 to 12 days (Figure 1).1 Although effective vaccines are available, measles has resurged both in the United States and worldwide, largely due to declining vaccination rates and increased travel to regions where the virus remains endemic. In the United States, the Centers for Disease Control (CDC) reports 1753 confirmed measles cases as of November 2025; most of these were associated with 45 outbreaks (clusters of 3 or mores cases). For comparison, 16 outbreaks were reported in 2024.2
A review of the clinical features of measles may be helpful in perioperative management (Table 1). Following initial flu-like symptoms, including cough, coryza, and conjunctivitis, patients with measles develop Koplik spots (tiny white spots inside the mouth) (Figure 2) and a maculopapular rash that spreads from the face downward. Individuals are contagious from four days before to four days after rash onset.3 Complications, such as otitis media, pneumonia, diarrhea, stomatitis, keratoconjunctivitis, encephalitis, and subacute sclerosing panencephalitis (SSPE) can occur—particularly in infants, and in pregnant, immunocompromised, and malnourished individuals.4 Measles infection can also result in prolonged immune suppression, increasing vulnerability to secondary infections and sepsis for months to years postinfection.5
Table 1: Summary of Considerations for Perioperative Measles.
| Consideration | Key Points |
| Epidemiology | Sporadic cases and outbreaks of measles are increasing in the U.S. |
| Transmission & Risk | Measles is highly contagious and spreads via secretions, droplets, and aerosols, which can linger in the air for hours. High risk for anesthesia professionals caring for infected patients. |
| Reporting Requirements | Many governments require immediate reporting of suspected or confirmed measles cases, regardless of day or hour. |
| Infectious Period | Measles is transmissible from 4 days before to 4 days after rash onset. Complications (e.g., pneumonia) may last longer and increase perioperative risk. |
| Elective Procedures | Defer elective procedures until after the infectious period and symptom resolution. |
| Urgent/Emergent Procedures | May proceed with caution; anticipate airway difficulties (mucosal swelling) and implement strict infection control measures. |
| Prevention & Post-Exposure Actions | Measles vaccine is effective. Postexposure prophylaxis with vaccine or immune globulin is also effective. |
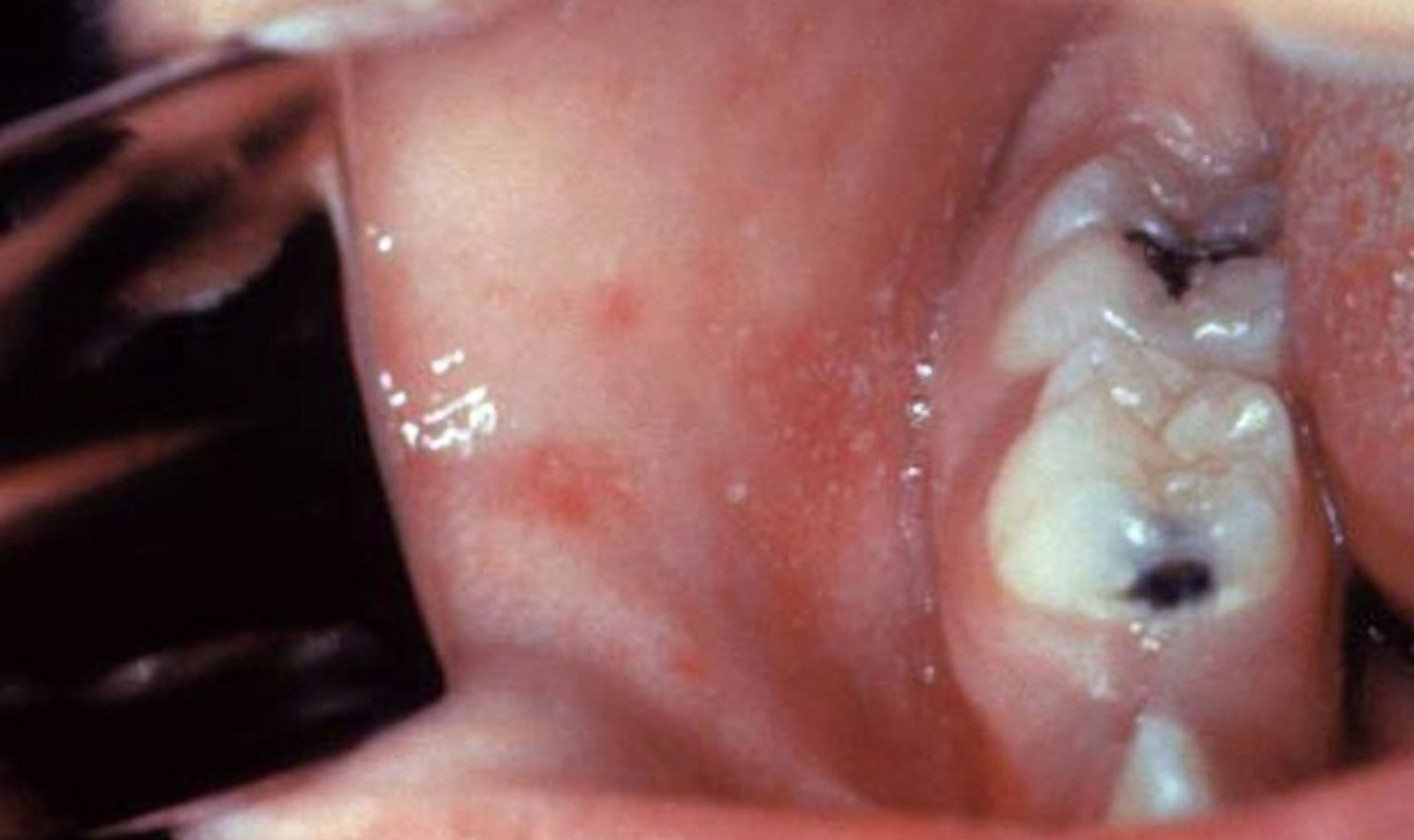
Figure 2: “Koplik spots” are irregular, bright red spots with bluish-white centers that appear on the cheeks and tongue mucosa indicating measles onset.
(Public Domain image; accessed from CDC on 11/19/2025 http://phil.cdc.gov/PHIL_Images/20040908/4f54ee8f0e5f49f58aaa30c1bc6413ba/6111_lores.jpg)
More than just an inconvenience, measles can kill. The mortality rate of measles is as low as 0.1% in high-income countries, but the mortality rate in low- or middle-income countries can reach 1.3%.6 There are no antiviral treatments for measles. Supportive care can be provided. Hydration and antipyretics are routinely used to manage fever and prevent dehydration, while carefully monitoring for secondary bacterial infections, such as pneumonia or otitis media. Vitamin A is recommended, especially for children who might be deficient, to reduce ocular complications of measles.7
For much of human history, immunity to measles was only available to those who survived the infection. Reports of symptoms consistent with measles infection date back to antiquity, with well-documented outbreaks recorded as early as the 1700s.8 Before the introduction of measles vaccines in 1963, nearly everyone was exposed to the virus at some point in their lives. Individuals who survive measles usually develop lifelong immunity; however, sustained protective antibody levels may require occasional re-exposure to the virus. Receiving two doses of the measles vaccine generally provides lifelong immunity, though some people, particularly as they age, may not maintain adequate antibody levels. Anesthesia professionals are generally considered immune to measles either through prior infection or completion of the recommended vaccination series.9
To reduce illness and complications, many industrialized countries have implemented mandatory measles vaccination policies. Maintaining high vaccination rates can effectively halt the endemic spread of the virus.6 The United States declared measles eliminated in 2000.7 However, travelers returning from areas where measles remains endemic continue to reintroduce the virus, resulting in new outbreaks.
ANESTHETIC CONSIDERATIONS
If a patient needs to undergo surgery during an active measles infection, anesthesia professionals need to remain alert for airway challenges and respiratory difficulties. There are few reports of specific problems during anesthesia for a measles patient, which may be because because precautions were appropriately taken.
When planning to anesthetize a patient with measles, one needs to consider the safety of the operating room team and other patients. Measles is highly contagious and both contact and airborne precautions are recommended with N95 or powered air purifying respirator, eye protection, gown, gloves, and hat (Figure 3).10 Although anesthesia professionals are considered immune, full personal protective gear is recommended, as immunized health care workers who have not used full protective equipment have developed measles.11
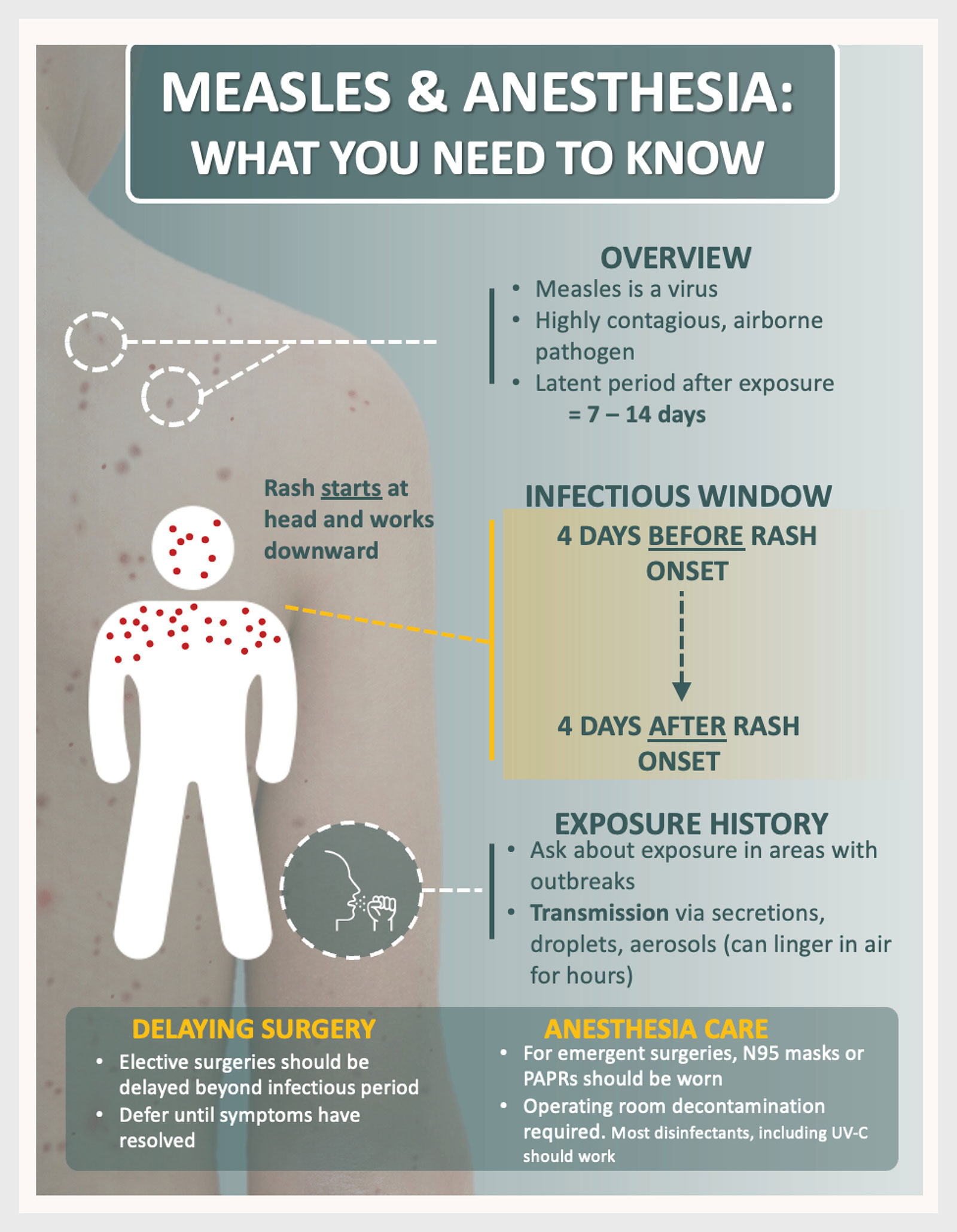
Figure 3: Important Perioperative Considerations for Measles. Created with the assistance of Microsoft Copilot.
Disinfecting an area where a patient with active measles has been treated is important to prevent further transmission of the virus. There are no published guidelines for operating room disinfection after a patient who is contagious for measles has received surgical care. Since measles is an enveloped virus, alcohol, chlorine, hydrogen peroxide, and ammonium-based cleaners are all considered effective for decontamination (nonenveloped viruses are more challenging to decontaminate). Heat or ultraviolet light treatments may also be effective.12
Although there are no antiviral treatments for measles, if a team member is exposed to measles but has uncertain immunity, there are preventative options. Because measles has an incubation time of several days, it is possible to utilize postexposure prophylaxis. Postexposure vaccination and post-exposure antibody administration are both effective at preventing or mitigating subsequent infection. It is recommended that unvaccinated or undervaccinated persons should receive the measles vaccine within 72 hours after exposure. For those with contraindications to the vaccine—such as immunocompromised individuals, pregnant persons, or infants younger than 6 months—human immune globulin is recommended within 6 days after exposure.13
Due to the difficulty of preventing the spread of measles, elective surgery should be postponed until the patient with measles has recovered and is no longer infectious, which is defined as at least four days after rash onset. This reduces the risk of transmission within health care settings and allows time for the wide range of acute complications to resolve.14
Emergency procedures can be conducted for patients with current or recent measles. The team should enforce strict contact and airborne precautions with N95 masks and, if possible, a negative-pressure room before surgery and during recovery should be utilized. It is best to limit staff to those confirmed immune if possible. The anesthesia plan should anticipate airway challenges including the potential for swollen and friable airway tissues. Preoperative assessment must include screening for measles complications and verifying the immunity of operating room staff. Postexposure prophylaxis (measles vaccine or immune globulin, depending on risk factors and timing) should be considered for exposed, nonimmune contacts.12
The period of immune suppression that follows measles infection is also a consideration. After recovering from measles there remains an increased risk of secondary infections and delayed wound healing.4 While there is no universally agreed-upon timeframe for deferral beyond the infectious period, increased monitoring may be necessary for several weeks to months following infection, particularly in high-risk individuals.
In summary, effective management of measles exposure in surgical settings requires a comprehensive approach that prioritizes infection identification, timely postexposure prophylaxis, and an understanding of the disease’s impact on perioperative care (Table 1). While supportive treatment remains the cornerstone for measles, careful consideration of patient immune status and appropriate surgical timing are crucial to minimizing complications and transmission risks. Continued vigilance, up-to-date protocols, and enhanced staff awareness will help safeguard both patients and health care professionals, ultimately supporting optimal outcomes in the perioperative environment.
Brendan Wanta, MD, is an assistant professor of anesthesiology at Mayo Clinic in Rochester, MN.
Jonathan Charnin, MD, FASA, is an assistant professor of anesthesiology at Mayo Clinic in Rochester, MN and co-chair of the APSF Patient Safety Priority Advisory Group on Infectious Diseases.
Randy Loftus, MD, is a professor of anesthesiology at Mayo Clinic in Rochester, MN and co-chair of the APSF Patient Safety Priority Advisory Group on Infectious Diseases.
Jonathan Tan, MD, MPH, MBI, FASA, is an associate professor of anesthesiology at Children’s Hospital of Philadelphia, Philadelphia, PA.
Melanie Hollidge, MD, PhD, FRCPC, is an associate professor of anesthesia at the University of Maryland R Adams Cowley Shock Trauma Center, Baltimore, MD.
Desiree Chappell, CRNA, is the vice president of clinical quality, NorthStar Anesthesia, Irving, TX.
Sara McMannus, RN, BSN, MBA is a clinical advisor, Sepsis Alliance, San Diego, CA.
Aranya Bagchi, MBBS, is an assistant professor of anesthesia at Harvard Medical School, and the clinical operations director of the Heart Center ICU at the Massachusetts General Hospital, Boston, MA.
Caitlin Bissell, MBA, is a senior portfolio manager for Solventum’s Infection Prevention and Surgical Solutions business.
Michelle Beam, DO, MBA, FASA, FACHE, is a clinical anesthesiologist at Penn Medicine, West Chester, PA.
Rich Beers, MD, is an emeritus professor of anesthesiology at Upstate Medical University, Syracuse, NY.
Raquel Bartz, MD, is a professor in the Department of Anesthesia and Pain Medicine, University of Washington School of Medicine, Seattle, WA.
Jonathan Tan receives research grant funding from the Anesthesia Patient Safety Foundation (APSF) and the Foundation for Anesthesia Education and Research (FAER).
Randy Loftus reports current research funding from NIH R01 AI155752-01A1, “BASIC trial: Improving implementation of evidence-based approaches and surveillance to prevent bacterial transmission and infection.” and has received funding from the Anesthesia Patient Safety Foundation, Sage Medical Inc., BBraun, Draeger, Surfacide, and Kenall; has one or more patents pending; and is a partner of RDB Bioinformatics, LLC, and 1055 N 115th St #301, Omaha, NE 68154, a company that owns OR PathTrac, and has spoken at educational meetings sponsored by Kenall and BBraun. The University of Iowa uses RDB Bioinformatics PathTrac system for measuring bacterial transmission.
Desiree Chappell is on the Speakers Bureau for Medtronic and Edwards LifeSciences, Advisory Board for ProVation.
Jonathan Charnin, Brendan Wanta, Richard Beers, Michelle Beam, Melanie Hollidge, Aranya Bagchi, and Sarah McMannus, report no conflicts of interest.
REFERENCES
- Centers for Disease Control and Prevention. Measles symptoms and complications. Accessed 7/29/2025, 2025. https://www.cdc.gov/measles/signs-symptoms/index.html
- Centers for Disease Control and Prevention. Measles cases in 2025. Accessed 11/25/2025. https://www.cdc.gov/measles/data-research/
- Hubschen JM, Gouandjika-Vasilache I, Dina J. Measles. Lancet. 2022;399:678–690. PMID: 35093206
- Thompson A. Child’s death shows how measles in the brain can kill years after an infection. Scientific American. September 12, 2025. Accessed 11/25/25. Available at https://www.scientificamerican.com/article/measles-death-shows-how-virus-can-hide-in-the-brain-for-years/
- Griffin DE. Measles virus-induced suppression of immune responses. Immunol Rev. 2010;236:176–189. PMID: 20636817
- Portnoy A, Jit M, Ferrari M, et al. Estimates of case-fatality ratios of measles in low-income and middle-income countries: a systematic review and modelling analysis. Lancet Glob Health. 2019;7:e472–e481. PMID: 30797735
- Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005;2005:CD001479. PMID: 16235283
- Centers for Disease Control and Prevention. History of measles. May 9 2024. Accessed 9/25/2025. Available at https://www.cdc.gov/measles/about/history.html
- Bester JC. Measles and measles vaccination: a review. JAMA Pediatr. 2016;170:1209–1215. PMID: 27695849
- Porteous GH, Hanson NA, Sueda LA, et al. Resurgence of vaccine-preventable diseases in the United States: anesthetic and critical care implications. Anesth Analg. 2016;122:1450–1473. PMID: 27088999
- Gohil SK, Okubo S, Klish S, et al. Healthcare workers and post-elimination era measles: lessons on acquisition and exposure prevention. Clin Infect Dis. 2016;62:166–172. PMID: 26354971
- Loftus RW, Dexter F, Evans L, et al. Evidence-based intraoperative infection control measures plus feedback are associated with attenuation of severe acute respiratory syndrome coronavirus-2 detection in operating rooms. Br J Anaesth. 2022;129(2):e29–e32. PMID: 35643533
- Strebel PM, Orenstein WA. Measles. N Engl J Med. 2019;381:349–357. PMID: 31184814
- Do LAH, Mulholland K. Measles 2025. N Engl J Med. 2025 Jun 25. Epub ahead of print. PMID: 40561553
