Improving perioperative safety in low- and middle-income countries requires addressing systemic barriers such as critical resource shortages, inadequate infrastructure, and a lack of standardized safety protocols. By prioritizing the implementation of evidence-based tools and fostering global partnerships, the international medical community can work toward reducing the disproportionately high rates of surgical morbidity and mortality in these regions.
Despite many international efforts, ensuring perioperative patient safety across different regions worldwide remains a major challenge. While only 6% of all surgical procedures occur in low- and middle- income countries (LMICs), over 50% of the perioperative death and disability resulting from surgery occurs in these nations.1 An estimated 95% of the annual deaths in patients under 20 years old are considered avoidable if surgical care were improved at community and district hospitals in these LMICs.2
In many LMICs, patient safety is at risk due to workforce shortages, inadequate training of anesthesia professionals, and limited access to patient safety monitors and essential medicines. This article explores recent key advances in anesthesia quality and safety initiatives in LMICs in the context of challenges and future outlooks.
ANESTHESIOLOGY WORKFORCE SHORTAGES
Globally, recent surveys reveal that of the 550,134 anesthesia professionals around the world, only 15% practice in LMICs secondary to inadequate infrastructure to support a certified, trained, or licensed workforce in these nations.3,4 In 2015, the Lancet Commission for Global Surgery (LCoGS) concluded that upwards of 5 billion people do not have access to safe, affordable surgical and anesthesia care when needed.5 Anesthesia and surgical workforce availability is one of the key indicators of underpreparedness.5 The authors also cite significant delays in accessing surgical care, which can arise from financial or geographic restrictions, limited specialized workforce, low awareness of available services, and low confidence in those services.5 Moreover, a recent report by Hendel et al. indicated that only 39% of the LMICs identified by the World Bank have representative anesthesia societies, posing significant difficulty to tracking anesthesia professionals in these countries.6 Of the LMICs with anesthesia societies such as Mozambique, Ethiopia, and Rwanda, there are about 0.3–0.6 anesthesia professionals available per 10,000 people, compared to 38.5 anesthesia professionals per 10,000 people in the high-income country of Australia.6
The lack of trained surgeons, obstetricians, and anesthesia professionals poses major patient safety concerns. In a publication that analyzed 11,422 surgical patients from 247 hospitals across Africa, these hospitals averaged 0.7 specialist surgeons, obstetricians, and anesthesia professionals per 100,000 patients. Cesarean deliveries were the most frequent procedure (33%). Overall, postoperative complications occurred in 18.2% of patients, with a 2.1% mortality rate. Despite generally low surgical risk, postoperative mortality in Africa was double the global average. Among cesarean deliveries, complication and mortality rates were 26.9% and 8.4%, respectively.7
Recent efforts to improve training of anesthesia professionals, credentialing, national tracking of anesthesia personnel, and access to safer services are underway. National policy frameworks have emerged as crucial tools to address this gap, particularly through the development of National, Surgical, Obstetric, and Anesthesia Plans (NSOAPs) and increased support from international organizations like the World Health Organization (WHO), the International Federation of Nurse Anesthetists (IFNA), and the World Federation of Societies of Anesthesiologists (WFSA). Several LMICs, such as Tanzania, Ethiopia, Nigeria, Rwanda, Senegal, and Zambia, have developed and implemented NSOAPs to improve access to surgical, obstetric, and anesthesia services, focusing on increasing clinician numbers, surgical volume, and tracking perioperative outcomes as a quality measure. In Tanzania, for example, 19.3% of all deaths are attributable to diseases amenable to surgery in a nation where 85% of cesarean deliveries and 71% of nonobstetric procedures are provided by nonphysician clinicians such as clinical officers and assistant medical officers.8 The Tanzanian NSOAP set a goal to raise the number of specialist surgical, obstetric, and anesthesia (SOA) professionals from 0.46 per 100,000 people in year 2017 to 2.27 per 100,000 by year 2025 (Figure 1). In 2024, SOA professionals had increased to 1.96 per 100,000 population in Tanzania.9
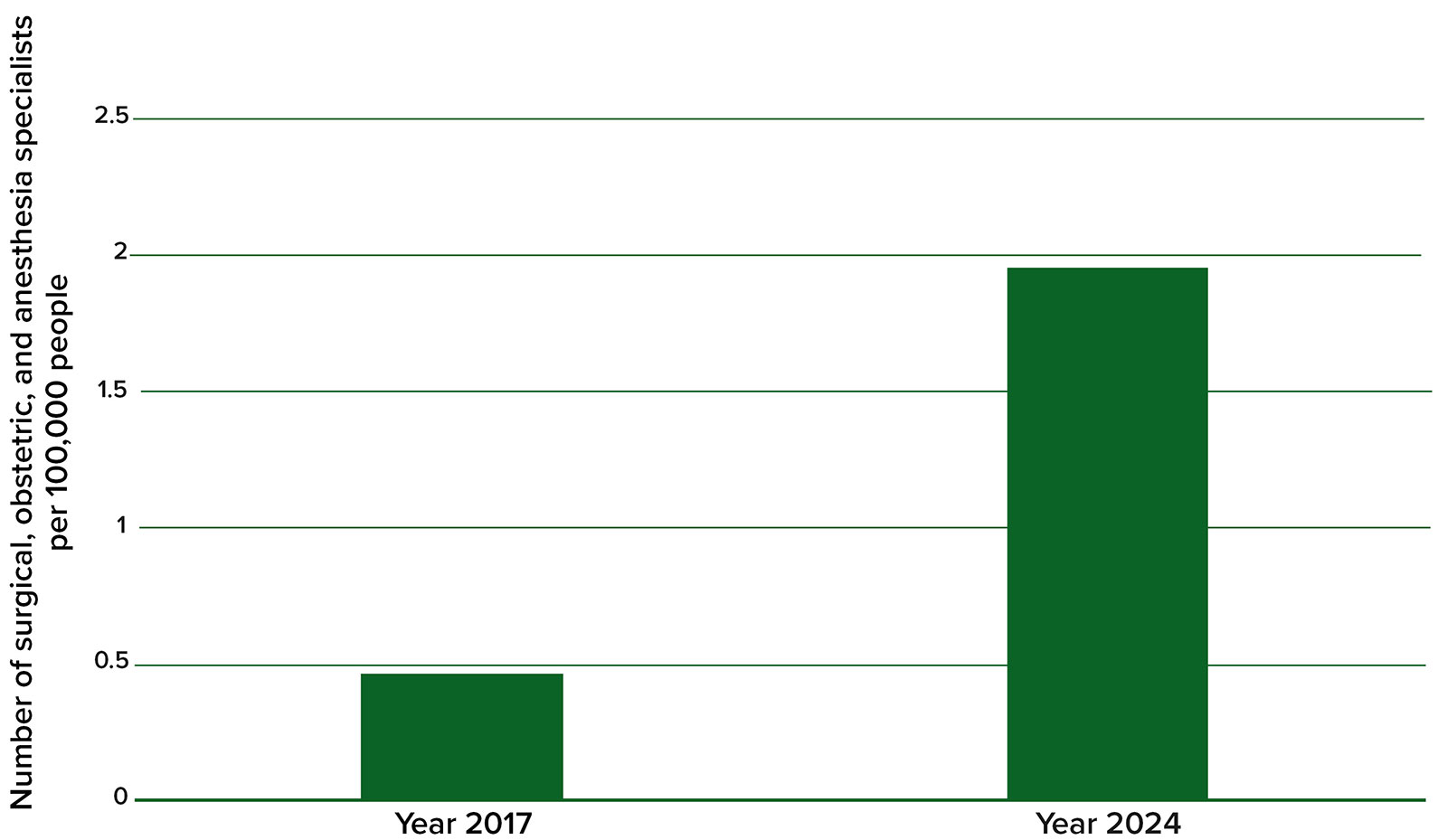
Figure 1: Effect of NSOAP implementation in Tanzania on number of surgical, obstetric, and anesthesia specialists per 100,000 people in 2017 (before implementation of NSOAP) compared to 2024 (after implementation).9
Challenges to implementing NSOAPs include a lack of awareness and a lack of a governance structure at the regional level.9 NSOAPs are important as they address workforce and other anesthesia and patient safety variables; however, tracking workforce has not been successful in all settings. Establishing a workforce baseline of health care professionals was a primary goal of NSOAPs. Additional reports from countries implementing NSOAPs are still needed to elucidate progress and regional challenges.9 As a reference, the LCoGS recommends that countries achieve a specialist surgical workforce (surgeons, anesthesia professionals, obstetricians) ratio of at least 20 specialists per 100,000 people by 2030.10 Ensuring a robust workforce of trained and credentialed anesthesia professionals is essential for improving access to surgery, creating a culture of patient safety, and ensuring best outcomes for patients.
ACCESS TO SAFETY MONITORING AND ESSENTIAL MEDICINES
In many LMICs, the challenge of ensuring patient safety and decreasing perioperative mortality is impacted by limited access to essential equipment such as pulse oximetry, oxygen, and rescue medications. While the WFSA and the WHO recommend pulse oximetry, oxygen, rescue medication, and capnography for each anesthetic, access to these resources has proven challenging with the expansion of basic surgical services into district-level hospitals (outside of major cities) in LMICs.11 These hospitals may not have trained anesthesia professionals, and those providing anesthesia may be working without basic monitors and medications, thereby compromising patient safety.
The WHO and the WFSA have both supported initiatives aimed at addressing these gaps. In particular, the WHO has endorsed organizations like Lifebox, a nonprofit organization established by Atul Gawande in collaboration with the Association of Anaesthetists of Great Britain and Ireland (AAGBI), the WFSA, and the Harvard School of Public Health. Lifebox focuses on providing affordable patient safety equipment—such as pulse oximeters and capnography devices—and promoting patient safety tools, including the WHO Surgical Safety Checklist.12 However, since Ministries of Health have not consistently addressed equipment and medication shortages, challenges persist, especially in communities removed from larger cities. Additionally, the WHO Surgical Safety Checklist has not been universally adopted, even in high-income countries.13,14 The use of the Surgical Safety Checklist has produced significant benefits across hospitals of various socioeconomic levels, such as a 47% reduction in major surgical mortality. The rates of overall complications, surgical-site infections, and unplanned reoperations also declined significantly.15 Access to important safety monitors and essential medicines, along with creating a culture of safety that embraces the use of checklists and other reminders of common pitfalls, are the greatest needs for providing consistent anesthesia care across countries and regions.
GLOBAL ANESTHESIA SAFETY ASSESSMENT TOOLS
To provide guidance in assessing and improving the quality of global anesthesia care, the WFSA and the WHO developed the International Standards for a Safe Practice of Anaesthesia (ISSPA), first published in 1992.16 This set of guidelines aim to assist anesthesiology departments, institutions, health care professionals, and policymakers in establishing and evaluating their compliance with international quality anesthesia care standards. The amended 2018 version of ISSPA covers recommendations for standardized professional training, facilities, equipment, medications, monitoring, and anesthesia management, and has been recommended as an assessment tool that promotes alignment with global anesthesia care standards.16
Recent literature has addressed the successes and challenges of efforts to align with ISSPA. In a 2024 report from the largest health care system in Morocco, a lower-middle income country, the percentages of anesthetic cases that met ISSPA standards were addressed.17 High compliance was noted for pre-anesthetic visits (89.6%), checklist completion (89.6%), and record keeping (79.6%). Lower compliance was found for postanesthesia care units (58.8%), nurse training (10.5%), premedication use (26.2%), and intraoperative neuromuscular monitoring. A 2020 report from a major hospital system in Cambodia, another lower-income country, showed high compliance in one-to-one patient care, preoperative evaluation, and basic monitoring (pulse oximetry, ECG, blood pressure). Low compliance was noted in the availability of CO₂ detectors, temperature and neuromuscular monitoring, defibrillators, fluid equipment, capnography, and continuing education.18 From these recent reports, it is evident that challenges are region-specific, institutionally variable, and highly dependent on leadership resources. Continued publication on these topics will help elucidate future global advances and challenges in incorporating ISSPA into anesthesia infrastructure.
QUALITY IMPROVEMENT BARRIERS AND TRACKING OF SURGICAL AND ANESTHESIA OUTCOMES DATA
In the last few years, perioperative research studies from LMICs such as Brazil, China, and India have been increasing. Despite this growth, large-scale studies from African regions have remained sparse. The bulk of existing research has focused on short-term surgical results and the patterns of diseases managed through surgery, while relatively few investigations have explored the specific challenges encountered in low-resource environments.19 LMICs often lack infrastructure and means to collect risk-adjusted surgical outcomes data.1,20 To improve surgical outcomes tracking in LMICs, a multidisciplinary understanding of the current practices and challenges to collecting data is needed.
In 2024, a multidisciplinary team from high-income and LMIC surgical settings conducted the first large-scale survey of stakeholders in LMICs regarding surgical data collection. A comprehensive survey was sent to perioperative personnel (surgeons, anesthesia professionals, anesthesia/surgical trainees, and administrators) to elucidate facilitating factors and barriers to collecting surgical outcomes data.1 Less than half of respondents reported having mentorship or research training, and 86.7% said their department offered little or no protected research time. Other major barriers to research included heavy clinical workloads, research costs, and poor medical documentation.1
FUTURE DIRECTIONS AND NEXT STEPS
The opportunity for improving perioperative outcomes in LMICs has never been greater. Thanks to the efforts of the Lancet Commission on Global Surgery and the World Bank’s Disease Control Priorities in Developing Countries, there is a universal commitment to scaling up surgical care in LMICs. This overarching commitment to increasing access to surgery, however, must be accompanied by a commitment to the necessary resources—human, functional and available equipment, medications, and system processes committed to best outcomes and patient safety. Additionally, the collection of data and tracking of outcomes is essential for quality improvement and to understand the impact of additional system level improvements over time.
The WHO and WFSA guidelines and recommendations have been impactful in encouraging National Ministries of Health to invest appropriately for patient safety and best perioperative outcomes. Scaling up to recommended equipment, medications, and processes in every location, however, has been unpredictable and slow in most LMICs. This has resulted in persistently poorer than expected outcomes for even healthy patients in LMICs. Recommendations for the future, therefore, include universal compliance with highly recommended resources and processes, increased workforce, and the tracking of indicators such as perioperative mortality rate over time.
Ying Eva Lu-Boettcher, MD, FASA, is an assistant professor at the University of Wisconsin School of Medicine and Public Health, Department of Anesthesiology, Madison WI.
Kathryn Kelly Ann McQueen, MD, MPH, FASA, FISS, is a professor and chair at the University of Wisconsin School of Medicine and Public Health, Department of Anesthesiology, Madison WI.
The authors report no conflicts of interest.
REFERENCES
- Diehl T, Jaraczewski TJ, Ahmed KS, et al. Barriers and facilitators to collecting surgical outcome data in low- and middle-income countries: an international survey. Ann Surg Open. 2024;5:e384. PMID: 38883944
- Sykes AG, Seyi-Olajide J, Ameh EA, et al. Estimates of treatable deaths within the first 20 years of life from scaling up surgical care at first-level hospitals in low- and middle-income countries. World J Surg. 2022;46:2114–2122. PMID: 35771254
- Khan IA, Karim HMR. Anesthesia services in low- and middle-income countries: the fragile point for safe surgery and patient safety. Cureus. 2023;15(8):e43174. PMID: 37692747
- McQueen KA. Anesthesia and the global burden of surgical disease. Int Anesthesiol Clin. 2010;48:91–107. PMID: 20386230
- Meara JG, Leather AJ, Hagander L, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386:569–624. PMID: 25924834
- Hendel S, Coonan T, Thomas S, McQueen K. The rate-limiting step: the provision of safe anesthesia in low-income countries. World J Surg. 2015;39:833–841. PMID: 25201470
- Biccard BM, Madiba TE, Kluyts HL, et al. Perioperative patient outcomes in the African Surgical Outcomes Study: a 7-day prospective observational cohort study. Lancet. 2018;391):1589–1598. PMID: 29306587
- Broekhuizen H, Lansu M, Gajewski J, et al. Using group model building to capture the complex dynamics of scaling up district-level surgery in Arusha Region, Tanzania. Int J Health Policy Manag. 2022;11:981–989. PMID: 33590734
- Hellar, AM, Akoko, L, Jumbam, DT, et al. An assessment of progress and challenges in the implementation of the National Surgical, Obstetric, and Anesthesia Plan (NSOAP) in Tanzania. East Cent Afr J Surg. 2024;29:15–22.
- Meara J, Greenberg S. The Lancet Commission on Global Surgery. Global surgery 2030: evidence and solutions for achieving health, welfare and economic development. Surgery. 2015;157:834–835. PMID: 25934019.
- Walker IA, Newton M, Bosenberg AT. Improving surgical safety globally: pulse oximetry and the WHO Guidelines for Safe Surgery. Paediatr Anaesth. 2011;21:825–828. PMID: 21208335
- Enright A, Merry A, Walker I, Wilson I. Lifebox: a global patient safety initiative. A A Case Rep. 2016;6:366–369. PMID: 27301049
- WHO surgical safety checklist and implementation manual. Available at: https://www.who.int/publications/i/item/9789241598590. Accessed May 20, 2025.
- Cadman V. Use of the WHO surgical safety checklist in low and middle income countries: a review of the literature. J Perioper Pract. 2018;28:334–338. PMID: 29737922
- van Klei WA, Hoff RG, van Aarnhem EEHL, et al. Effects of the introduction of the WHO “Surgical Safety Checklist” on in-hospital mortality: a cohort study. Ann Surg. 2012;255:44–49. PMID: 22123159
- Gelb AW, Morriss WW, Johnson W, et al. World Health Organization-World Federation of Societies of Anaesthesiologists (WHO-WFSA) international standards for a safe practice of anesthesia. Anesth Analg. 2018;126:2047–2055. PMID: 29736769
- Harfaoui W, Ziani H, Slaihi Z, et al. Compliance with World Health Organization (WHO)-World Federation of Societies of Anesthesiologists (WFSA) Standards for general anesthesia at Ibn Sina University Hospital Center, Morocco. Cureus. 2024;16:e51980. PMID: 38344478
- Tao KM, Sokha S, Yuan HB. The challenge of safe anesthesia in developing countries: defining the problems in a medical center in Cambodia. BMC Health Serv Res. 2020;20:204. PMID: 32164745
- Knight SR, Ots R, Maimbo M, et al. Systematic review of the use of big data to improve surgery in low- and middle-income countries. Br J Surg. 2019;106:e62–e72. PMID: 30620075
- McQueen KA. The global anesthesia crisis and continuous quality improvement. Int Anesthesiol Clin. 2014;52:109–119. PMID: 24370724
