Reports emerged of moisture and mold accumulation within certain GE HealthCare anesthesia workstations, primarily associated with prolonged use and high-humidity clinical settings. A system-wide investigation identified vulnerabilities within the ventilator breathing system, and informed mitigation strategies to protect patient safety and equipment integrity.
| Table of Contents |
DEAR RAPID RESPONSE:
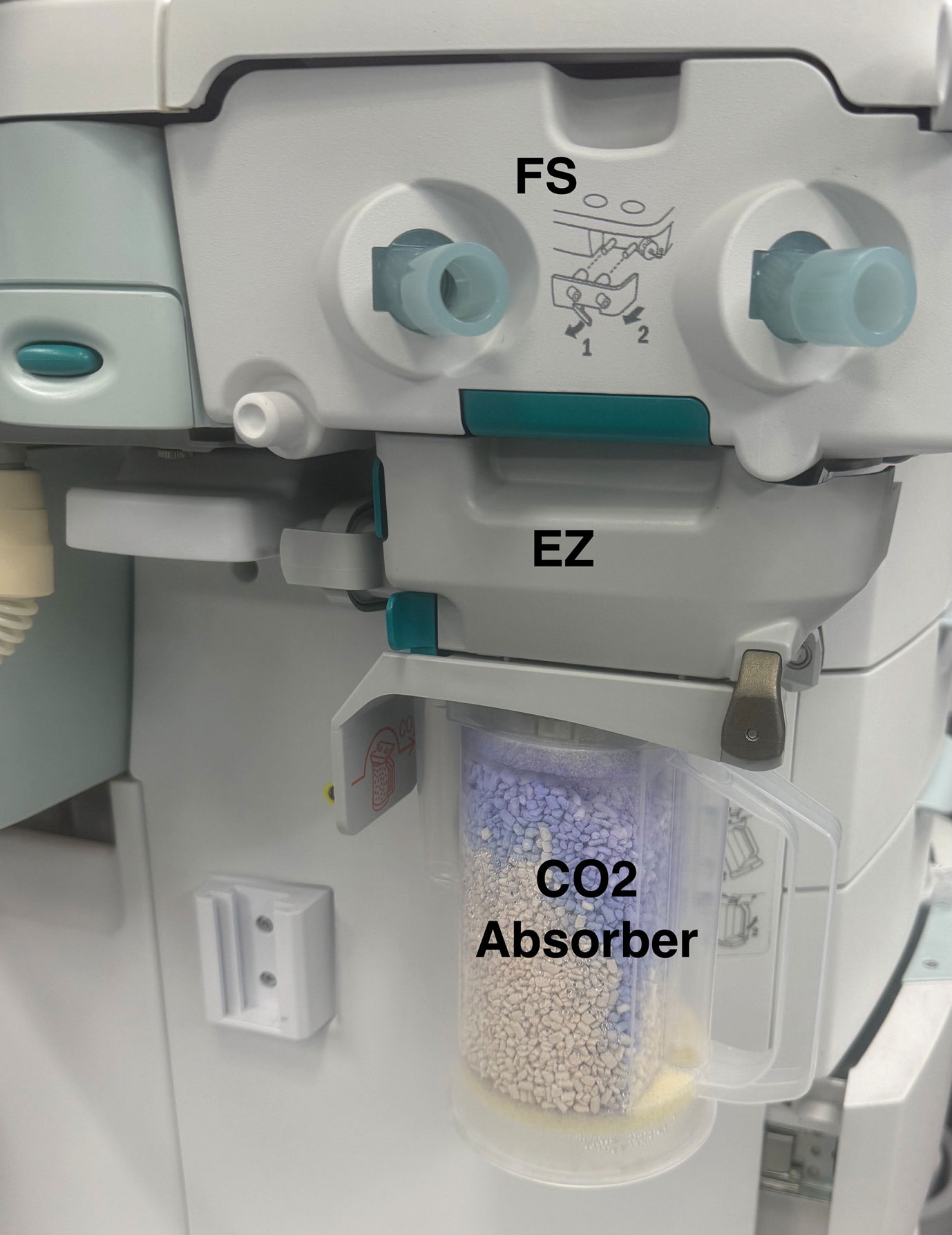
Figure 1: Depiction of the flow sensor unit (FS), EZChange module (EZ) and CO2 absorber in GE Ventilators. The circuit has been removed in this picture.
In the same week, two GE HealthCare Aisys CS2 anesthesia workstations (GE HealthCare, Madison WI) in a single facility within Advocate Health, a 69-hospital health care system across 6 states, were found to have black particles on the EZChange module (Figure 1) of the Advanced Breathing System (ABS), raising concern for mold growth (Figure 2). The EZChange module supports continued ventilation of the patient while the CO2 absorbent canister is exchanged.1 The mold-like particles were initially identified during investigations into a failed daily checkout and a flow sensor failure alarm event. A multidisciplinary team including anesthesia professionals, infection prevention, technicians, administration, and clinical engineering was convened to investigate further across the health care system.
Inspection of 300 GE HealthCare Operating Room (OR) anesthesia workstations found 21 units (7%), including Aisys CS2 and Avance CS2 models, with potential mold. Multiple additional workstations showed significant moisture accumulation within the internal components of the ventilators. Cultures were taken of the mold-like substance from 3 ventilators, two of which grew Cladosporium spp. and the other Alterneria. One hundred eighty-eight additional GE HealthCare anesthesia workstations in non-OR areas were evaluated and did not demonstrate evidence for moisture or mold. Outreach to peers in other health care systems revealed similar reports of mold growth in GE HealthCare anesthesia workstations, and one health system reported mold reappearance as soon as 18 days after sterilization. We decided to implement moisture and mold checks every 1–2 weeks in our system to identify any mold regrowth. Another health system which had implemented all moisture mitigation solutions reported no mold growth in GE HealthCare anesthesia workstations. This information guided our discussions with GE HealthCare.

Figure 2: Black particles concerning for mold around the valve in the EZChange module where moisture-containing gas leaves the absorbent canister.
A literature review and assessment of patient risk was immediately performed when the findings were reported. Prior research on ventilator contamination and patient risk is limited. APSF has previously reported that infectious risk from contaminated anesthesia ventilators is low. This is due in part to the caustic nature of the CO2 absorbent, which is hostile to pathogens, and also to the effectiveness of filters in the breathing circuit.2 Fungal and bacterial growth in anesthesia breathing circuits has been documented; however, these findings were largely attributed to ineffective reprocessing methods and introduction of organisms during air drying.3 No correlation between organisms in the circuits and patients who developed postoperative pneumonia have been found, and there was no difference in contamination between high and low fresh gas flow rates.4
Evaluation of anesthesia practices revealed that all Advocate Health sites routinely use a new heat and moisture exchange filter (HMEF) with each case and replace it intraoperatively if it becomes saturated or visibly contaminated. HMEF, a high efficiency viral filter with 99.99% efficiency, effectively filters fungal organisms, which are significantly larger than viral particles.2 We reviewed six months of patient respiratory cultures from 19 facilities within our system, focusing on non-Aspergillus mold growth. Some of these sites used GE HealthCare anesthesia workstations, while others used workstations from other vendors. Regardless of the type of workstation used at the site, non-Aspergillus mold species were rarely identified in patient’s respiratory cultures. Additionally, no association was found between patients with mold in respiratory cultures and the presence of a recent operative procedure. Based on our internal practice review and review of the literature, risk to patients was deemed minimal. Nevertheless, all anesthesia workstations with concern for mold growth were taken out of service immediately for sterilization per the manufacturer’s instructions for use.5
GE HealthCare was notified of the findings and provided support through virtual and in-person site visits and emails to help determine root causes and mitigation strategies to prevent future occurrences. Since moisture accumulation in the EZChange module was deemed to be a root cause for mold growth, guidance was provided on sterilization and moisture mitigation solutions. GE HealthCare provided a contact person for each region within our system to address ongoing concerns for mold growth in anesthesia workstations. We initially encountered variable communication on ideal moisture mitigation strategies. Specifically, there were different messages about the priorities for proposed solutions and the impact of filters in the breathing circuit. Other health systems reported lack of clarity from GE on remediation of moisture and mold.
Moisture can accumulate in the anesthesia breathing circuit from two sources—the patient and the reaction of absorbent with exhaled CO2. Exhaled gas contains 100% humidity, and the absorbent reaction generates heat and water. When an HMEF is placed at the y-piece, a significant amount of exhaled moisture is absorbed and prevented from entering the breathing circuit. The amount of moisture created by the absorbent reaction is highly dependent upon fresh gas flow. When fresh gas flow exceeds minute ventilation, exhaled gas is not rebreathed and there is little to no CO2 reacting with the absorbent. As fresh gas flow is reduced below minute ventilation, the amount of exhaled gas returning to the patient increases and therefore more CO2 reacts with the absorbent creating moisture in the circuit. Our investigation found that even at a fresh gas flow of 2 L/min, there is enough rebreathing to allow moisture to accumulate in the circuit. Ambient temperature also plays a role in moisture accumulation with colder temperatures causing moisture to condense in the circuit. Moisture mitigation was therefore a key focus of prevention especially given our desire to practice low-flow anesthesia.
INVESTIGATION FINDINGS
- Most end-users lacked awareness that moisture accumulation could be an issue in anesthesia workstations.
- While a few sites within our system had implemented some moisture mitigation practices, most were unaware of optional moisture mitigation steps that can be employed such as:
- Add-on condenser for drainage of excess moisture
- Removal of the breathing circuit overnight
- Removal of the flow sensor overnight
- Although lower fresh gas flow rates are associated with increased rebreathing, and, therefore, moisture accumulation,6-8 mold and moisture were found in ventilators regardless of whether sites routinely practiced low-flow ventilation as part of sustainability efforts.
- Excess moisture accumulation was more common in workstations exposed to higher case volumes and longer surgical durations.
- There are no specific guidelines from manufacturers on sterilization frequency, and facilities lacked a standardized process or adequate training for sterilizing the ABS.
PRACTICE CHANGES IMPLEMENTED IN THE SYSTEM
- Extensive anesthesia professional and technician education was provided through grand rounds, emails, and virtual and in-person meetings. Anesthesia professionals were specifically educated on weekly mold and moisture checks and daily moisture mitigation steps, which included removing the breathing circuit and flow sensors overnight (Figures 3 and 4).
- Flow sensor and ABS inventory were performed at all practice locations and, where needed, additional components to support moisture mitigation and sterilization were purchased to minimize the risk of interrupting patient care due to moisture and mold.
- Sites with GE HealthCare anesthesia workstations were instructed on how to inspect the ABS for moisture or mold every 1–2 weeks to monitor for regrowth and confirm mitigation effectiveness (Figure 4).
- Non-OR areas with shorter case durations, less ventilator utilization, and no initial moisture or mold issues were not required to perform ongoing assessments.
- Assessments were discontinued once the individual site had no units with moisture or mold for two audit cycles.
- Despite routine removal of flow sensors and breathing circuits overnight, higher surgical volume sites continued to identify moisture within the ABS, albeit at a lower frequency.
- Add-on condenser elements for all OR anesthesia workstations are being purchased from GE HealthCare. This additional step was deemed necessary due to continued moisture accumulation despite a change in practice and the likely increase in complex and longer surgical cases.
- A multidisciplinary team established an internal procedure and assigned responsibility for monitoring moisture accumulation, assembly/disassembly of ventilators, and sterilization.
- Annual sterilization of all OR ventilators was also implemented as part of our annual preventative maintenance.
- GE HealthCare hosted live webinars and developed video-based training for sterile processing and clinical engineering teams on assembly, disassembly, and sterilization of the ventilators.
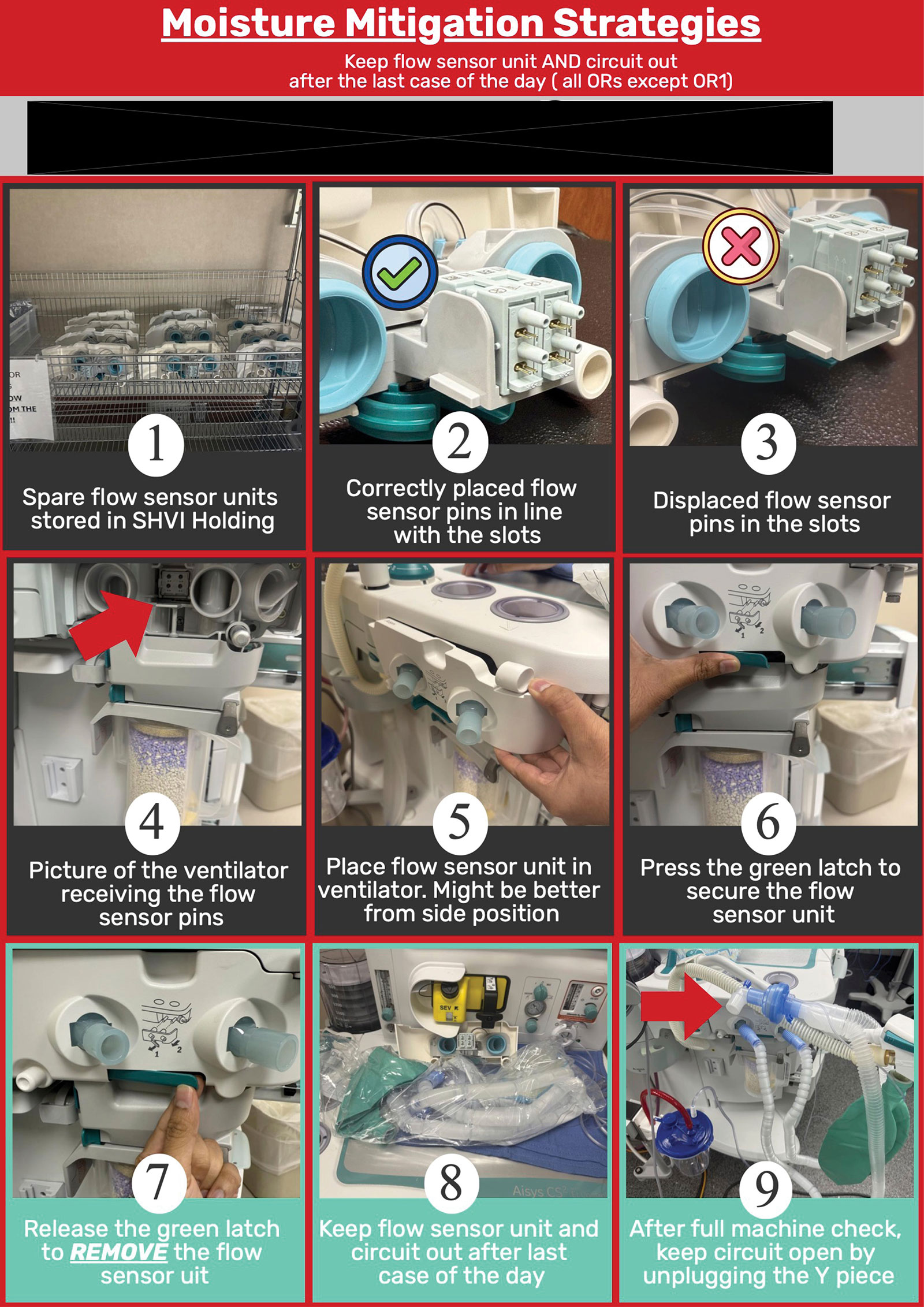
Figure 3: Educational flyer on moisture mitigation for anesthesia professionals and technicians.
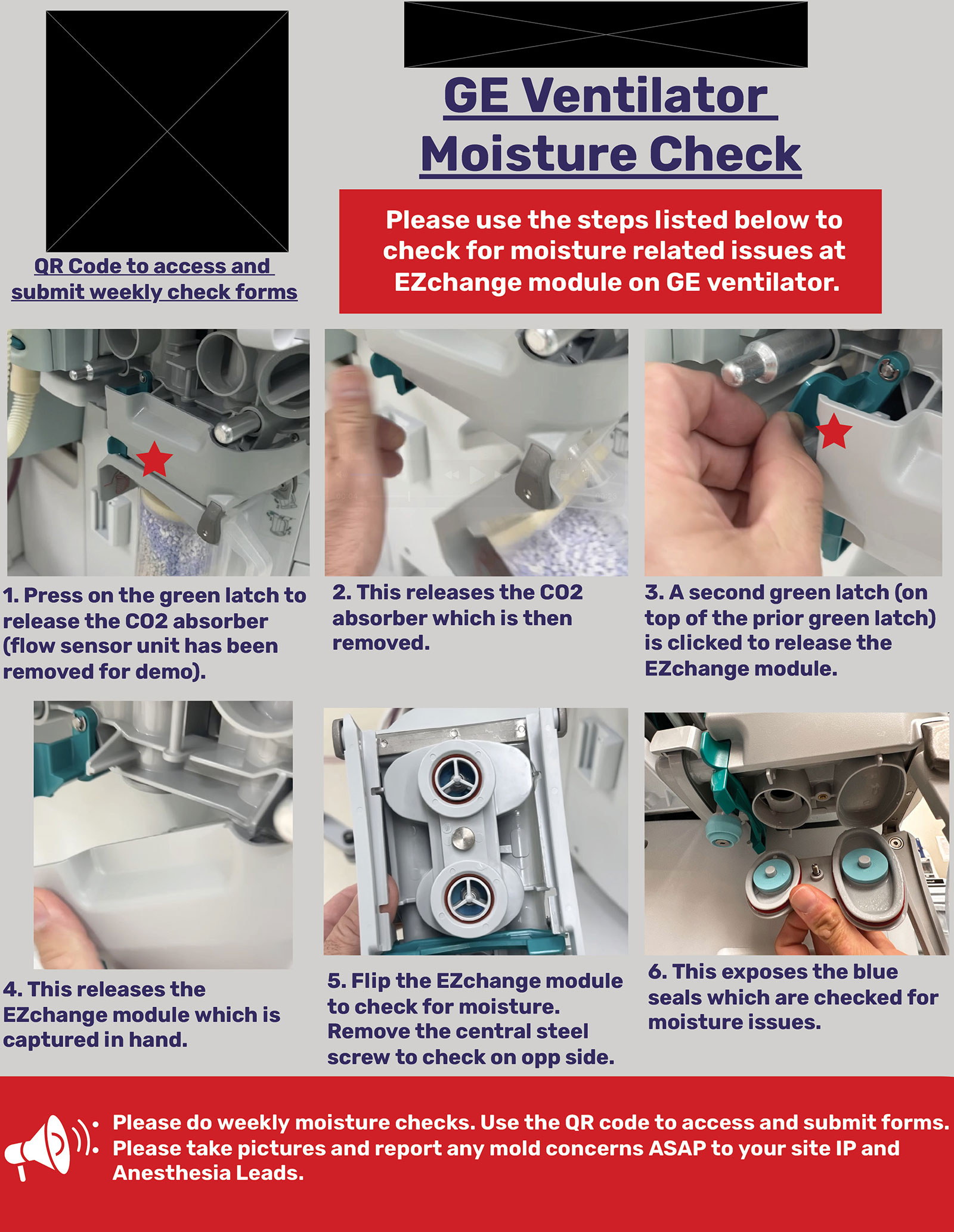
Figure 4: 1–2 weekly Moisture and Mold check flyer.
CONCLUSION
In our multistate health care system, we found GE HealthCare anesthesia workstations to accumulate moisture leading to mold growth, especially in sites that have not implemented moisture mitigation practices deemed optional by the manufacturer. Unless excessive moisture results in alarms potentially triggering manual evaluation, there is no externally visible way to see mold has grown, nor any internal trigger to alert biologic growth within our workstations. While our assessment revealed minimal infectious risk to patients given the routine use of HMEF filters between the patient and ventilator components, sites should assess their risk based on local practices. It is important to note that this moisture accumulation could impact flow sensors, reducing the accuracy of tidal volume measurements.
Education of anesthesia professionals using GE anesthesia workstations on the potential for and impact of moisture accumulation, in addition to the need to implement moisture mitigation solutions, is needed. While lower fresh gas flow rates increase rebreathing and the potential for moisture retention, increasing fresh gas flow to eliminate rebreathing and moisture production is not a useful strategy. Fresh gas flows required to eliminate rebreathing must exceed minute ventilation creating substantial anesthetic gas waste, increased expense, and a negative impact on the environment.7 A practice of low-flow anesthesia can be done safely and effectively once strategies for moisture mitigation are employed.
Sterilization of OR anesthesia workstations is a complex and coordinated effort that needs education and involvement of multiple teams. It is essential to balance and weigh the need for sterilization against the workload and impact on the internal components from sterilization and disassembly and reassembly of the ABS units.
QUESTIONS TO GE HEALTHCARE
- While newer models of GE anesthesia workstations are designed with a built-in condenser, GE HealthCare designates the condenser as an optional product for older models. We have continued to see mold growth despite implementing two moisture mitigation solutions that included removing the flow sensor and circuits overnight. Based on our experience that moisture accumulated despite daily moisture mitigation practices, we believe the condenser is a necessary moisture mitigation solution for all compatible older models and not an optional product.
- During discussions with other health systems using GE workstations, some sites reported implementing all moisture mitigation solutions while others were not aware of moisture mitigation solutions and their importance. Could GE HealthCare share what initiatives have been undertaken or are being planned to ensure a comprehensive and consistent moisture mitigation education for all clinical sites in the country?
QUESTIONS TO APSF
- Please educate on the need for multiple filter use for each patient. Is it necessary to have both HMEF and expiratory filters for all patients? If a site decides to use just one filter, which filter is the preferred filter for adult and pediatric populations?
- Please educate on the need for moisture mitigation when using non-GE HealthCare ventilator brands.
- Is there any evidence or guidance on moisture levels that are safe within ventilators and breathing circuits?
- Please provide guidance on OR ventilator sterilization frequency. Should this be a part of yearly preventative maintenance?
Sandeep Narayan, MD, is an anesthesiologist with Scope Anesthesia of North Carolia, PLLC and is an adjunct assistant professor at Wake Forest University School of Medicine.
Katie Passaretti, MD, is the chief infection prevention officer for Advocate Health and is a professor of internal medicine in the Section of Infectious Disease at Wake Forest University School of Medicine.
The authors report no conflicts of interest.
REFERENCES
- GE HealthCare. Aisys CS2 Technical reference manual. December 4, 2024. Available at https://www.gehealthcare.com/support/manuals?search=eyJzZWFyY2hUZXJtIjoiMjA2OTEzNy0wMDEiLCJsYW5ndWFnZU5hbWUiOiJFbmdsaXNoIChFTikifQ%3D%3D Accessed November 24, 2025.
- Feldman J, Loeb R, Philip J. FAQ on anesthesia machine use, protection, and decontamination during the COVID-19 pandemic. Anesthesia Patient Safety Foundation. Published July 27, 2023. https://www.apsf.org/faq-on-anesthesia-machine-use-protection-and-decontamination-during-the-covid-19-pandemic/ Accessed November 23, 2025.
- Arai LA de C, Azevedo RB. Contamination of anesthesia circuits by pathogens. Bra J Anesthesiol. 2011;61(1):50-59. PMID: 21334507
- Bengston JP, Brandberg A, Brinkhoff B, Sonander H, Stenqvist O. Low-flow anaesthesia does not increase the risk of microbial contamination through the circle absorber system. Acta Anaesthesiol Scand. 1989;33:89–92. PMID: 2916393
- GE HealthCare. ABS cleaning and sterilization. Published April 23, 2024. https://www.gehealthcare.com/support/manuals?srsltid=AfmBOooMYu_ABXNoK2UVbs43cVy5ObAIu-Ld1P2Jnltz6Yv4isUXEez0&search=eyJzZWFyY2hUZXJtIjoiMjA5NDg4My0wMDEiLCJsYW5ndWFnZU5hbWUiOiJFbmdsaXNoIChFTikifQ%3D%3D Accessed November 23, 2025.
- Feldman J, Lampotang S, Hendrickx J. Is rebreathing prevented when FGF equals MV? Anesthesia Patient Safety Foundation. Published October 20, 2022. https://www.apsf.org/article/is-rebreathing-prevented-when-fgf-equals-mv/ Accessed November 23, 2025.
- Feldman JM. Managing fresh gas flow to reduce environmental contamination. Anesth Analg. 2012;114:1093–1101. PMID: 22415533
- Feldman J, Lampotang S. Patient safety and low-flow anesthesia. APSF Newsletter. 2022;37:54–56. https://www.apsf.org/article/patient-safety-and-low-flow-anesthesia/ Accessed December 4, 2025.
MOISTURE AND MOLD: APSF RESPONSE
by Jeffrey Feldman, MD, MSE
| Editor’s Note: We are pleased to be able to publish the Rapid Response report from Drs. Narayan and Passaretti on their investigation and management of moisture and mold in the anesthesia workstation, along with the accompanying guidance from the manufacturer, GE HealthCare. The report raised several questions for APSF. Here are the responses to those questions: Moisture and Mold: APSF Response |
QUESTION 1:
Please educate on the need for multiple filter use for each patient—is it necessary to have both HME filters and expiratory filters for all patients? If a site decides to use just one filter, which filter is the preferred filter for adult and pediatric populations?
Answer: The short answer is that APSF recommends a pleated filter be located between the expiratory limb and the breathing circuit. A high-quality filter in that location should prevent respiratory pathogens (bacteria, viruses, and molds) from entering the anesthesia machine. It is not uncommon to place another pleated filter between the machine and the inspiratory limb as a safety against pathogens from the machine getting to the patient, but there is little evidence to suggest this is a significant patient safety concern. Heat and moisture exchange devices placed at the airway often include filters effective for bacteria and viral pathogens although they are not as effective as the pleated filters. The sampling tube for sidestream gas analysis can also bring pathogens into the machine, which can be prevented by using an HME filter at the airway. Many sidestream devices also have internal filters—check with the manufacturer to confirm. APSF has two resources that were published during the COVID-19 pandemic that provide additional details which are germane to this discussion.
FAQ on Anesthesia Machine Use, Protection, and Decontamination During the COVID-19 Pandemic
HEPA Filters. Do We Really Know Enough?—Breathing System Filters in the Era of COVID-19
QUESTION 2:
Please educate on the need for moisture mitigation when using non-GE HealthCare ventilator brands.
Answer: The authors are correct to observe that anesthesia machines from different manufacturers vary in the approach to moisture mitigation. Water traps and heating elements in the breathing circuit are commonly used. There are too many anesthesia machines in use to provide a detailed explanation for every machine. Manufacturers are a reliable source of information on how to approach moisture mitigation in a specific machine. The clinical impact of moisture in the circuit depends upon both anesthesia machine design and clinical practices. Reducing fresh gas flow consistent with a low-flow anesthesia practice can be done safely with attention to moisture mitigation but will increase the amount of moisture in the circuit. Clinicians are advised to understand the best practices for moisture mitigation based upon clinical practice and the specific devices they use.
QUESTION 3:
Is there any evidence or guidance on moisture levels that are safe within ventilators and breathing circuits?
Answer: I am not aware of specific moisture levels that are considered safe. Moisture is desirable in the breathing circuit if it prevents drying of secretions and the respiratory mucosa, but it becomes unsafe when moisture interferes with sensor measurements or results in growth of pathogens. Heat and moisture exchange filters are a useful barrier for keeping the lungs moist and reducing the amount of moisture entering the machine. They will not, however, reduce the moisture created by carbon dioxide absorption.
QUESTION 4:
Please provide guidance on OR ventilator sterilization frequency. Should this be a part of yearly preventative maintenance?
Answer: After discussing this question with the Emergency Care Research Institute (ECRI)and anesthesia machine manufacturers, we could not identify a rationale for recommending a specific interval for OR ventilator sterilization. While the manufacturers provide specific guidance to sterilize the breathing circuits, it is a time-consuming process, which introduces cost and complexity to practice. In reality, the anesthesia breathing circuit is never a sterile component and is always exposed to organisms and contaminants in the environment. Reasonable indications for sterilization would include visible internal contamination of the circuit or perhaps after caring for a patient with a pathogen known to be transmitted through the respiratory system, e.g., tuberculosis.
Jeffrey Feldman, MD, MSE, FASA, is professor of clinical anesthesiology (retired) at Perelman School of Medicine and Children’s Hospital of Philadelphia. He is also the chair of the APSF Committee on Technology.
Dr Feldman has compensated consulting relationships with Micropore Inc., Blink Device Company, Draeger Medical, and GE HealthCare.
GE HealthCare Response to APSF Submission on Moisture and Mold in GE HealthCare Anesthesia Workstations
by Robert Myers and John Beard, MD
DEAR RAPID RESPONSE:
GE HealthCare appreciates the opportunity to respond to the submission titled “OR Ventilators—Moisture, Mold, and More in GE Operating Room Ventilators: System Response and Mitigation” authored by Drs. Sandeep Narayan, MD, and Katie Passaretti, MD. We commend Advocate Health for this thorough investigation and commitment to patient safety.
We have reviewed the Advocate Health report on moisture accumulation and mold growth in GE HealthCare anesthesia workstations, specifically the Aisys CS2 and Avance CS2 models. Moisture accumulation is an inherent characteristic of all modern anesthesia rebreathing systems. Moisture originates from two primary sources: patient exhalation, which is saturated with water vapor, and the chemical reaction of CO₂ absorption, which produces heat and water. These factors are not unique to GE HealthCare systems. If not proactively addressed through moisture management and reprocessing, moisture can lead to microbial growth, particularly in warm environments.
GE HealthCare anesthesia machines include features and recommended equipment maintenance instructions to effectively manage foreseeable moisture accumulation.
DESIGN AND MOISTURE MANAGEMENT FEATURES
GE HealthCare anesthesia machines are designed with breathing systems to support low-flow anesthesia and are verified to operate in environments with 100% humidity. To manage moisture accumulation, several optional components are available, including:
- Condensers to collect and drain excess moisture.
- Heat and Moisture Exchange (HME) filters to reduce moisture entering the breathing circuit.
These components are described as optional in our User’s Reference Manuals1,2 (URMs), as their use is dependent on clinical practice and institutional protocols. The newest models of GE HealthCare anesthesia machines include a condenser within the CO2 absorbent canister, which eliminates the need for an additional condenser component.
MAINTENANCE, REPROCESSING, AND STERILIZATION PRACTICES
GE HealthCare URMs state that anesthesia breathing systems are not sterile and require routine maintenance and reprocessing. Disconnection of the breathing circuit and air drying of the breathing system are two commonly employed maintenance strategies. While we do not mandate a fixed reprocessing frequency, we recommend that institutions follow local infection prevention policies and clinical usage patterns. We recommend the use of inspiratory and expiratory bacterial/viral filters to reduce contamination risk and provide guidance on cleaning and sterilization in our URMs,3 as well as on our website.4 Additionally, we offer training resources, including on-site training, webinars, and instructional videos, to support proper maintenance and sterilization procedures.
MOISTURE ACCUMULATION AND MICROBIAL GROWTH
We appreciate the authors’ investigation, which identified mold in anesthesia workstations and noted regrowth in some cases after reprocessing. We also admire the epidemiologic investigation, which did not identify these mold species in patient specimens in the health system. The identification of Cladosporium spp. and Alternaria is consistent with environmental fungi, which may be found in the hospital environment. We agree with the authors’ conclusion that patient risk is minimal, especially with the use of bacterial/viral filters. GE HealthCare is aware of no adverse events reported with this issue and supports continued vigilance and routine inspection of workstations, particularly in OR settings where low-flows and long-duration anesthetics are common, creating the conditions for moisture accumulation.
COMMUNICATION AND EDUCATION
GE HealthCare thanks the authors for feedback on our communication and education deployment across their sites. GE HealthCare is working to optimize the effectiveness of our customer support to ensure the most effective utilization of our equipment. We are expanding our educational outreach to emphasize the moisture mitigation strategies referenced above as technology supporting low-flow practice, such as End-tidal Control*, becomes more widely implemented.
IMPACT ON VENTILATOR PERFORMANCE
Moisture accumulation is not expected to impact ventilator performance. In rare cases, moisture in sensing lines could affect flow sensor performance and tidal volume measurement. To mitigate this impact, our systems are equipped with cross-checks and alarms (e.g., “Calibrate, dry, or replace flow sensors”) to alert users to potential issues. Importantly, PAW (airway pressure) measurements remain unaffected due to the location of the measurement port. Furthermore, machine design places flow sensors in an elevated position to be free from moisture in the gas pathway.
RESPONSE TO SPECIFIC QUESTIONS
Optional condenser: GE HealthCare offers condensers as optional accessories for Aisys CS2 and Avance CS2 models. As moisture accumulation is dependent on clinical practice, the condenser is not required by all customers—it is offered as an optional accessory if additional moisture management is needed.
Education Initiatives: GE HealthCare is continually enhancing its training programs and documentation to ensure consistent understanding of moisture mitigation strategies across all customer sites.
Inspiratory/Expiratory Filters and Moisture: These filters are primarily designed to prevent microbial contamination, not to manage moisture. HME filters are more effective for moisture control.
CONCLUSION
GE HealthCare is grateful to participate in this discussion of moisture accumulation in anesthetic breathing systems. We value the collaboration with Advocate Health and APSF to identify and address issues proactively while expanding knowledge to the medical community. We encourage all users to consult our URMs and reach out to our support teams for guidance on best practices for moisture management and workstation maintenance.
Sincerely,
Robert Meyers, principal mechanical engineer of GE Healthcare.
John Beard, MD, chief medical officer, patient care solutions of GE Healthcare.
REFERENCES
- GE HealthCare. Aisys CS2 user’s reference manual (Part no. 5824841). Datex-Ohmeda, Inc.; 2023.
- GE HealthCare. Avance CS² user’s reference manual (Part no. 5835098). Datex-Ohmeda, Inc.; 2022.
- GE HealthCare. Advanced breathing system cleaning, disinfection and sterilization user’s reference manual (Part no. 2094883-001). Datex-Ohmeda, Inc.; 2024.
- GE HealthCare. Cleaner compatibility. Available from: https://cleaning.gehealthcare.com/
*End-tidal Control in the United States is indicated for patients 18 years of age and older.
The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or group responses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intention of APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
