Prosocial behavior—voluntary actions intended to benefit others, such as kindness, cooperation, and gratitude—serves as a powerful tool to mitigate clinician burnout and enhance organizational resilience. By fostering a culture of civility and mutual support, perioperative teams can reduce cognitive load, improve communication, and directly enhance patient safety and operational efficiency.
| PROSOCIALITY: ANY BEHAVIOR ORIENTED TOWARD THE WELFARE OF OTHERS OR ONE’S GROUP AS A WHOLE |
More than ever, perioperative services must use time and human resources efficiently. Demand for health care services continues to grow while staffing shortages are stressing an already vulnerable system. Burnout rates are high and increasing, putting more pressure on those who remain, leading to more burnout. These challenges can limit the ability to provide services and make it difficult to achieve and sustain efficiency and patient safety targets. New approaches are needed to foster a stable engaged workforce and mitigate ongoing quality and safety problems.1 There is evidence from sectors other than health care that “prosocial” behaviors among people who work together lead to effective teamwork and greater satisfaction for everyone.2 We describe the essence of prosocial behaviors and how these behaviors can be fostered to enhance team collaboration in procedural care. Our goal is to raise awareness of the need for cultural change to address ongoing workforce and efficiency challenges. To begin, here is an example of behaviors you may recognize in a typical operating room and will likely agree are counterproductive to not only providing safe, effective, and efficient care but also to simply having a nice day.
A surgeon has scheduled three procedures during an 8-hour block of surgical time. Two are robotic prostatectomies and one just a “short” cystoscopy case. The nursing team consists of an experienced circulating nurse and a relatively new scrub technician. The anesthesiologist is responsible for managing two operating rooms along with a CRNA in each room. The CRNA assigned to the robotic cases is an experienced traveling CRNA working for four weeks in the facility. The first patient was identified to have a difficult airway in the preoperative review the day before the procedure.
The surgeon arrives in the morning 20 minutes before the scheduled start time and tells the circulating nurse that they have to start and finish the day “on time” so she can get to a meeting with the chair of surgery. The nurse responds he has been asked to stay late all week for long cases and cannot stay late today. In addition, the same nurse is instructing the scrub tech on preparing and managing the robot and asks the anesthesia team not to bring the patient to the room until they are ready. The anesthesiologist tells the team he will be starting his other room first to reduce the time pressure when caring for the patient with the difficult airway. The patient is brought to the room almost 10 minutes after the scheduled start time and the surgeon asks why the case is starting “late.” The surgeon also questions if the fiberoptic-guided intubation will take extra time. The anesthesiologist and CRNA have not worked together previously, and it takes about 30 minutes for the patient to be anesthetized and intubated. The surgeon comments that the day will never be able to finish on time if the remaining cases take this long to get started.
This vignette illustrates the “production pressure” that is common in procedural areas. Some degree of production pressure can be helpful to keeping the care team focused on working productively together. Counterproductive behaviors fostered by production pressure set the stage for reduced efficiency, staff burnout, decreased staff retention, and avoidable patient harm.3 The unique needs of each patient require the team of caregivers at the bedside to be empowered to make decisions that support safe and efficient care.
Caring for a patient requiring a procedure is a team sport. In addition to the primary proceduralist/surgeon, the team also includes nurses, technicians, and anesthesia professionals during the procedure and numerous other personnel readying the patient, ordering and preparing instruments and supplies and cleaning the environment. There are examples of procedural areas where the proceduralist/surgeon, nurses, technicians, and anesthesia professionals and other personnel involved in providing care work well as a team. Well-functioning teams are more likely to be present in environments where a group of people work together regularly and develop shared expertise and camaraderie. More typically, especially as health systems have expanded, the team consists of people who may or may not know each other well, nor work together on a regular basis. While these people may have a shared knowledge of the requirements to complete the procedure safely and effectively, it can be challenging for them to coordinate their efforts and collaborate.
ENHANCING PROCEDURAL TEAM PERFORMANCE IS NOT A NEW CONCEPT
There is extensive literature investigating the performance of procedural care teams and interventions for improvement, e.g., briefings, checklists, team training and debriefing, but rigorous studies are lacking.4,5 One study of patients undergoing spinal fusion for idiopathic scoliosis found a positive correlation between team consistency and heightened efficiency.6 Other studies have provided evidence that familiarity between the team members enables safer care and team collaboration.7-9
Despite the lack of strong evidence, there is general recognition that some interventions can be effective for improving procedural team performance. The Association of Operating Room Nurses (AORN) has published a comprehensive guide of strategies intended to enhance team communication in the operating room.10 The improvement strategy does not have to be complex; simple interventions may have a positive impact on both teams and patients. For example, the use of a compassionate pause as a moment of reflection for surgical teams at a time-out can be a useful method for enhancing bonds between team members.11 While it may be advantageous to schedule people to work together frequently, it can be difficult in a larger organization to match the individual needs for work scheduling with procedural block times. The use of temporary or traveling staff further impedes organizational efforts to foster team familiarity.
PROSOCIAL CONCEPTS AND PROCEDURAL PATIENT CARE
We offer for consideration a model not yet applied in perioperative care that could foster more collaborative working relationships and the benefits that would ensue. The model arises from the work of Elinor Ostrom, who was awarded the 2009 Nobel Prize in Economics for her research on group collaboration. Ostrom described a set of Core Design Principles (CDPs) that are common to groups of people who successfully share a common limited resource.12 David Sloan-Wilson generalized the CDPs and applied them to understanding any group where there is a shared common goal (Table 1).2 These CDPs can be used to analyze how well the team in our vignette is likely to function as a group, and also to identify opportunities for improvement. In this example, both positive and negative behaviors that influence the CDPs are described (Table 2). While there are examples where the group complies with a specific CDP, there are numerous opportunities for improvement.
Table 1: Core Design Principles for Successful Group Collaboration.
| Ostrom Principles | Generalized Prosocial Principles | Adaptive Impact |
| Clearly defined boundaries | Shared identity and purpose | A group that works for all: Defines the group and its culture as purposeful, equitable with a power arrangement appropriate for the mission. |
| Proportional equivalence of benefits and costs | Equitable distribution of costs and benefits | |
| Collective choice arrangements | Fair and inclusive decision-making | |
| Monitoring | Monitoring agreed behaviors (transparency) | All working for the group: Ensures effectiveness within groups by utilizing reciprocity, reputation, and trust to balance individual and collective interests. |
| Graduated sanctions | Graduated response to helpful and unhelpful behaviors | |
| Conflict resolution and mechanisms | Fast and fair conflict resolution | |
| Minimal recognition of rights to organize | Authority to self-govern | Working with other groups: Ensures effectiveness between groups by balancing interests and supporting shared power. |
| Polycentric governance | Collaborative relations with other groups |
Ostrom’s eight core design principles and generalized versions oriented towards prosocial behavior. (Adapted with permission from Paul Atkins)
Table 2: Core Design Principles Applied to the Problem of OR efficiency.
| CDP | Positive Contributor to CDP | Negative Contributor to CDP |
| Is there shared identity and purpose? | Commitment to the patient’s safety and outcome | Shared team identity is questionable Efficiency and safety goals are in conflict |
| Is there equitable distribution of contributions and benefits? | Shared benefit of employment | Inequalities in the team especially hierarchy and autonomy Surgeon’s work extends beyond the procedure |
| Is there fair and inclusive decision-making? | Morning huddle used for team to review the needs of the day | Procedures planned without input from the rest of the team |
| Monitoring of agreed behaviors | Efficiency metrics typically tracked | Unacceptable behaviors are not well defined nor consistently monitored |
| Gradual responding to helpful and unhelpful behavior | Emphasis on psychological safety to empower all personnel. | No accepted standard for responding to behaviors that impede patient care goals |
| Is there fast and fair conflict resolution? | No formal process for addressing staff conflicts that impede team performance | |
| Authority to self-govern | OR teams typically control the activities of the day without close management of tasks and patient flow | OR team has limited ability to impact system problems that impede performance |
| Collaborative relations with other groups | Communication between the intra- procedure team and the pre- and post-procedure teams typically not well integrated |
Analysis of common procedural team dynamics for compliance with Ostrom’s core design principles. Examples of positive and negative contributors to each of the core design principles are provided.
From the behavioral science perspective, well-being can be analyzed by measuring the coercive control in one’s environment specifically, the opportunities for individuals to influence their environment, and access to positive consequences. For example, if we consider the original vignette, we can see the coercive forces on the team members from production pressure and the hierarchical relationships. The individual opportunities to influence the environment are limited for the nurse by the training needs, for the anesthesiologist by the need to care for another patient, for the nurse anesthetist due to a temporary status, and for the surgeon by the need to use block time completely in order to provide timely care to patients. While the group likely seeks access to the same positive consequences of safe and effective care completed in timely fashion, there are many factors that conspire against achieving that goal. When successful, the prosocial approach enhances the well-being of workers and consumers as well as organizational financial goals.13,14
Returning to our vignette, we can imagine that beginning the day with verbal recognition by each of the team members of the pressures they feel collectively can foster individual engagement in the team effort. Similarly, pre-planning between and among the team members can reduce the impact of production pressure and allow for each individual to exert some influence on how the work will be accomplished.
Defining the CDPs for effective group collaboration provides a validated scientific foundation for prosocial change. Acceptance and Commitment Training (ACT) is useful for realizing such positive change at individual, group, and organizational levels.15 ACT is a validated methodology for managing burnout and negative behaviors in the service of maintaining healthy, cooperative working environments.16-18 A useful tool for applying ACT training to both individual and group behaviors is the ACT Matrix.15 As an analytical tool, the ACT Matrix becomes a procedure for analyzing the environment and understanding behaviors that move away from or towards desired goals. Essential to that process is training individuals to notice when their behavior is counterproductive and develop the psychological flexibility to adopt productive behaviors.
We can apply the ACT matrix to the group highlighted in our vignette to describe the current state and define a more desirable future state (Figure 1).
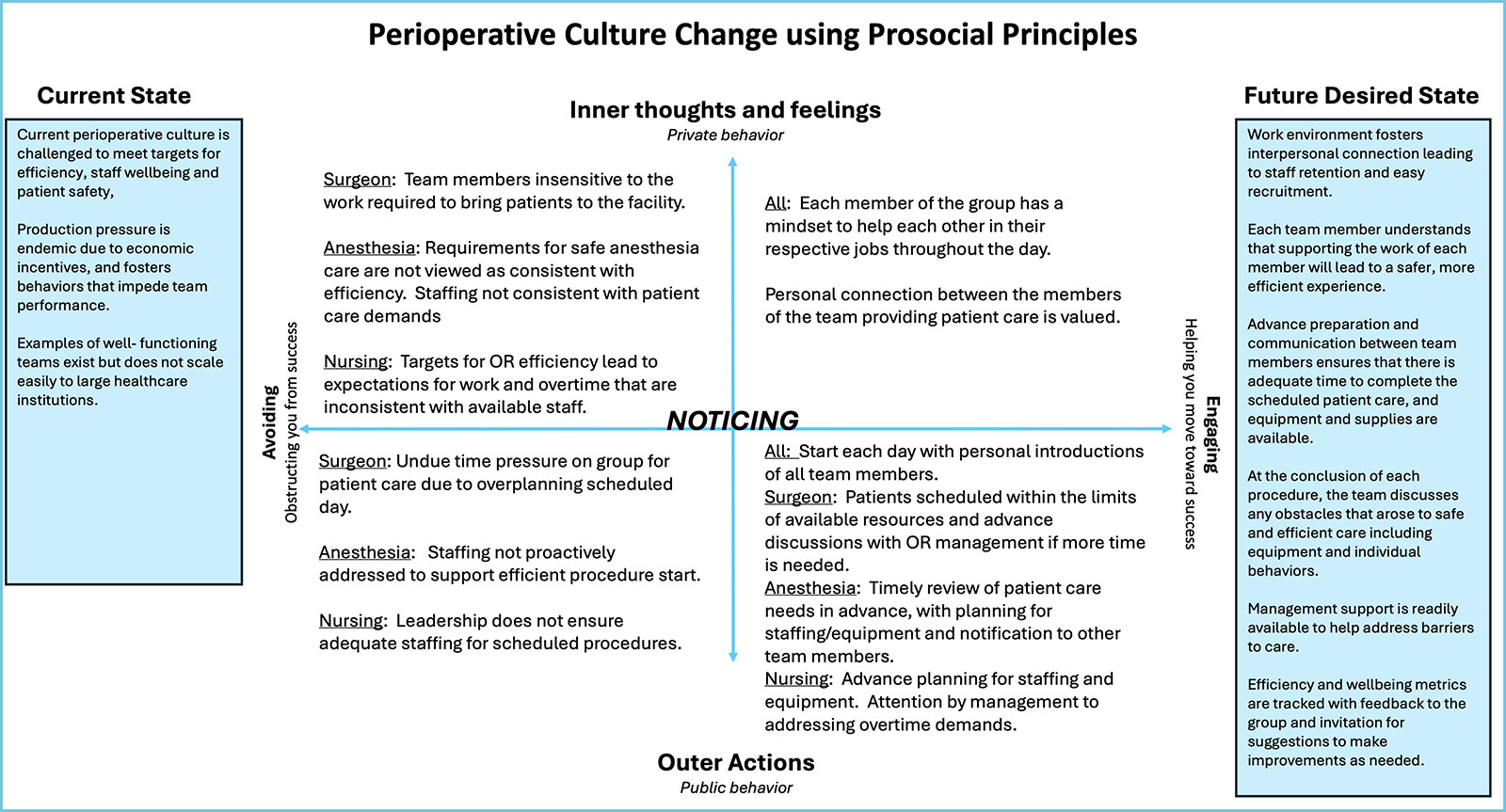
Figure 1: ACT Matrix applied to a procedural team helps to understand the behaviors required to move from the current state to a more desired future state. Specific behaviors move the individual or group towards the desired future state (engaging) or away from the current state (avoiding) as indicated by the horizontal axis. The vertical axis indicates differences between “Outer” or observable behaviors and “Inner” behaviors or what we experience. Avoiding-behaviors are typically self-interested; engaging behaviors are prosocial, intended to foster the group mission. The individual action of NOTICING these behaviors and developing the psychological flexibility to replace avoiding behaviors with engaging behaviors is central to ACT training. Special thanks to Dr. Kevin Polk and colleagues for their original formulation. (Adapted with permission from Paul Atkins.)
POTENTIAL FOR PROSOCIAL CHANGE IN THE OPERATING ROOM
Changing established cultures requires engaging the people involved to recognize the limitations of existing culture and the potential value of making a change. The current shortage of staff leading to the burnout syndrome in health care can be a motivating change. In addition, efficiency goals continue to increase as more people require care and organizations struggle to remain profitable. Teaming has been promoted as an active process, essential to the success of every organization where groups of people need to work together to meet targets for success.19
The potential value of prosocial change is to create a culture that fosters highly functional teams that maximize efficiency AND derive job satisfaction from collegial relationships and collectively achieving shared goals. While this type of culture is clearly desirable and has been applied successfully in many venues, the process required to achieve such change in procedural areas in health care is unclear. It’s worth our time and effort to try new methods for reducing burnout, increasing job satisfaction, and providing safe, efficient care.
THE FUTURE STATE
Changing the established periprocedural culture will be challenging, but we can imagine how embedded prosocial behaviors might alter the perioperative vignette. As before, the scenario is an 8-hour block where three cases have been scheduled- two robotic prostatectomies and a cystoscopy.
The day prior to the OR day, all professionals to be involved with the cases are scheduled and notified. The surgeon sends a group text acknowledging that the schedule is ambitious and indicates that she will be available at the start of the day to help the team manage the day. Nursing leadership ensures that the circulator and scrub tech have an opportunity to discuss the setup for the next day in advance. The anesthesia team reviews the patient together and plans to manage a fiberoptic-guided intubation. The anesthesiologist communicates with the team in his other room with the goal of minimizing any delay to the start of the robotic cases.
On the morning of the procedure, the team huddles 20 minutes prior to the anticipated start of the case. At that point, the patient has been evaluated in the preop area by both the surgeon and anesthesiologist. The circulator is instructing the new scrub tech on preparing a robotic procedure, reinforcing the discussion from the prior day. The nurse anesthetist brings the patient into the room on time, is well-prepared for induction and intubation after the prior discussion with the anesthesiologist, and can begin monitoring and sedating the patient. The anesthesiologist joins 10 minutes later after starting the other room. During the process of induction and fiberoptic intubation, the surgeon (who has remained in the room) offers to assist the anesthesia team so the circulator and scrub tech can continue to prepare equipment for the procedure.
As the timeout checklist begins, the surgeon states, “Let’s take a moment to ensure we are all set for the day. If anyone has any concerns or needs support, now is the time to speak up.” The circulating nurse introduces the scrub tech who is in training by name, and the anesthesiologist introduces the visiting nurse anesthetist. These new team members are welcomed and encouraged to ask any questions. The anesthesiologist indicates he is covering two rooms and identifies the need for communication to coordinate the work in both rooms throughout the day.
Towards the end of the second case, the procedure time is running longer than expected, and the surgeon invites the team to discuss any challenges to starting the last case and completing the day on time. The circulator states that he can stay for a short time after the scheduled day to take care of the patient, but the surgeon encourages them to speak to nursing leadership before starting the case to ensure there is relief if needed. The team works quickly to turn over the operating room and begin the last case. Despite their efforts, the last case runs 30 minutes late, but everyone wants to finish the day together. As the anesthesia team exits the room with the patient, everyone expresses appreciation for the communication and teamwork during the day.
It is easy to pen a “Hollywood” ending to this story since it is not a sequence of actual events. Nevertheless, the behaviors described in the second vignette, where people proactively plan how to work together, are not part of the routine culture in many or most procedural areas; these behaviors are born of a prosocial approach to the work where all team members act in ways that demonstrate mutual respect and support in the service of safe and effective patient care.
Team efficiency and staff wellness and retention are measurable and can be used to assess impact. It is time to look more critically at our existing culture and to evaluate the potential impact of validated tools like prosocial culture change to foster team engagement and performance.
This article introduces the science and methods of prosocial change. More detailed information can be found at Prosocial World.
Jeffrey Feldman, MD, MSE, FASA, is chair of the APSF Committee on Technology and professor of clinical anesthesiology (retired), University of Pennsylvania, Children’s Hospital of Philadelphia, Philadelphia, PA.
Ramona Houmanfar, PhD, is professor and director, Behavior Analysis Program; director, Performance System Technologies Lab, Department of Psychology, College of Science, at University of Nevada, Reno, NV.
Mary Fearon, RN, MSN, is a nurse consultant at MMFearon, LLC.
John M. Flynn, MD, is chief and Richard M. Armstrong Jr. endowed chair in pediatric orthopedic surgery, Children’s Hospital of Philadelphia; professor of orthopedic surgery, University of Pennsylvania, Philadelphia, PA.
Jeffrey B. Cooper, PhD, is professor emeritus of anesthesiology (retired), Harvard Medical School.
Stuart Libman, MD, is a board certified adult, child, & adolescent psychiatrist; medical director, PLEA Agency, Peer Reviewed ACT Trainer of the Association for Contextual Behavior Science.
Caoimhe Duffy, MD, MSc, CPPS, FCAI, is assistant professor in anesthesia and critical care, Perelman School of Medicine, Hospital of the University of Pennsylvania.
Lisa Spruce, DNP, RN, CNOR, CNS-CP, EBP-C, APRN, FAAN, is senior director of evidence-based perioperative practice, Association of periOperative Registered Nurses.
Della Lin, MS, MD, FASA, is on the APSF Board of Directors.
Jeff Feldman has compensated consulting relationships with Micropore Inc., Blink Device Company, Draeger Medical and GE Healthcare. Della Lin is secretary of the APSF. Ramona Houmanfar, Mary Fearon, John M. Flynn, Jeffrey B. Cooper, Stuart Libman, Caoimhe Duffy, and Lisa Spruce report no conflicts of interest.
REFERENCES
- Wears R, Sutcliffe K. Still not safe: patient safety and the middle-managing of American medicine. New York, NY: Oxford University Press; 2019.
- Wilson DS, Ostrom E, Cox ME. Generalizing the core design principles for the efficacy of groups. J Econ Behav Organ. 2013;90:S21–S32.
- Hashemian SM, Triantis K. Production pressure and its relationship to safety: a systematic review and future directions. Saf Sci. 2023;159:106045.
- Levesque MJ, Etherington C, Lalonde M et al. Interventions to facilitate interprofessional collaboration in the operating theatre: a scoping review. J Perioper Pract. 2024;34:6–19. PMID: 36468241
- Ghanmi N, Bondok M, Etherington C et al. Optimizing teamwork in the operating room: a scoping review of actionable teamwork strategies. Cureus. 2024;16:e60522. PMID: 38883070
- Givens RR, Brown M, Malka M, et al. Do teams of strangers create health care dangers? The effect of OR team consistency on operative times in adolescent idiopathic scoliosis. Spine Deform. 2025;13:123–133. PMID: 39320701
- Hallet J, Sutradhar R, Jerath A, et al. Association between familiarity of the surgeon-anesthesiologist dyad and postoperative patient outcomes for complex gastrointestinal cancer surgery. JAMA Surg. 2023;158:465–473. PMID: 36811886
- Hallet J, Jerath A, d’Empaire PP, et al. Familiarity of the surgeon-anesthesiologist dyad and major morbidity after high-risk elective surgery. JAMA Surg. 2025;160:772–781. PMID: 40434753
- Burden M, Astik G, Auerbach A, et al. Identifying and measuring administrative harms experienced by hospitalists and administrative leaders. JAMA Intern Med. 2024;184:1014–1023. PMID: 38913371
- Association of periOperative Registered Nurses (AORN). Team communication. in: guidelines for perioperative practice. Denver, CO: AORN, Inc; 2025.
- Moldes JM, Llobenes L, Stremmler MM, et al. Surgery with compassion: a potential shift in surgical paradigms. J Pediatr Urol. 2025;21:788–789. PMID: 40016016
- Ostrom, E. Governing the commons: the evolution of institutions for collective action. Cambridge University Press, Cambridge, UK, 1990.
- Houmanfar RA, Alavosius MP, Morford ZH, et al. Functions of organizational leaders in cultural change: financial and social well-being. J Organ Behav Manag. 2015;35:4-27. https://doi.org/10.4324/9780203713198-2
- Houmanfar RA, Szarko A. Utilizing values-based governance to promote well-being in organizations and beyond. In: Houmanfar RA, Fryling M, Alavosius MP, eds. Applied behavior science in organizations: consilience of historical and emerging trends in organizational behavior management. Taylor & Francis; 2022:291–315.
- Polk KL, Schoendorf B, eds. The ACT matrix: a new approach to building psychological flexibility across settings and populations. New Harbinger; 2014.
- Hayes SC, Atkins P, Wilson DS. Prosocial: Using an evolutionary approach to modify cooperation in small groups. In: Houmanfar RA, Fryling M, Alavosius MP, eds. Applied behavior science in organizations: consilience of historical and emerging trends in organizational behavior management. Taylor & Francis; 2022.
- Moran DJ, Batten S, Gamble MA, Atkins P. Acceptance and commitment training: Improving performance in organizations with applied contextual behavioral science. In: Houmanfar RA, Fryling M, Alavosius MP, eds. Applied behavior science in organizations: consilience of historical and emerging trends in organizational behavior management. Taylor & Francis; 2022.
- Szarko AJ, Houmanfar RA, Smith GS, et al. Impact of acceptance and commitment training on resilience and burnout in medical education. J Contextual Behav Sci. 2022;23:190-199. https://doi.org/10.1016/j.jcbs.2022.02.004
- Edmunson AC. Teaming: how organizations learn, innovate, and compete in the knowledge economy. Jossey Bass Pfeiffer, 2012.
