Patient safety relies on robust relationships and teamwork in the perioperative space. The concept of “leading infinitely” is explored – reaching across disciplines and complex environments to build relationships and incorporate multiple perspectives into decision-making. Such connections can ensure safety, excellence, and improved outcomes in the perioperative environment.
INTRODUCTION

Sparrow is Amazon’s new intelligent robotic system.
Originally founded in 1994 under the name Cadabra, the company we now know as Amazon completely revolutionized the way we shop. With a staggering market capitalization of $2.4 trillion,1 Amazon’s relentless commitment to innovation is perhaps best embodied in its newest fulfillment facility in Shreveport, LA. Here, a trio of robotic arms with names like Robin, Cardinal, and Sparrow retrieve and package items from Amazon’s Sequoia multistory inventory platform, which are then transported to loading docks and loaded onto Rivian electric delivery vehicles by Proteus, Amazon’s first fully autonomous mobile robot.2
While this relentless pursuit of technological innovation recalls images from our favorite science fiction movies, Amazon was originally a small online bookseller in the garage of founder Jeff Bezos’ rental home in Bellevue, WA. Before its explosive expansion, Amazon was intensely and passionately focused on gaining the trust of a single subset of customers: online book enthusiasts.3 Before crossing the chasm from that of a small online bookseller to a global marketplace serving millions of customers, Amazon was unwaveringly and singularly focused on serving its niche market of book enthusiast customers. Anesthesia leaders need to do the same: focus intensely on the relationships we cultivate across the health care system to move beyond our role solely as perioperative patient safety experts and onto the application of our skills, wisdom, and experience to the health care team as a whole. We previously wrote about “Infinite Anesthesia,” but now we need to think infinitely bigger.4
CROSSING THE CHASM
In his 1991 book, Crossing the Chasm: Marketing and Selling High Tech Products to Mainstream Customers,5 marketing strategist Geoffrey Moore laid out a strategic framework for businesses aiming to achieve broad-scale adoption of their products. According to Moore, there are distinct and pivotal stages in the technology adoption lifecycle, with each requiring a different playbook to navigate unique challenges and opportunities. At its core, the crossing the chasm framework demands an understanding of and distinction between those customers who want the newest things and those who want complete solutions and convenience. These customers can be represented by a bell-shaped curve (Figure 1), where only the smallest percentage are true tech enthusiasts and innovators, and slightly more are visionaries and early adopters. To gain market penetration, Moore contends that crossing the chasm from early adopters to mainstream customers—the much larger subset of the more pragmatic but swayable early majority—represents a hurdle that many companies fail to cross. However, companies that cross this chasm by winning over early adopters will attain widespread adoption by the more pragmatic crowd of early and late adopters and laggards. Moore calls this cascading wave of rapid and widespread adoption the “tornado,” but it is only achieved after focusing on the “lead bowling pin” represented by specific niche markets (deemed “pragmatists in pain”) that value and very much need the company’s unique offering. Widespread adoption occurs when companies focus intently and unwaveringly on finding and serving these customers first, ignoring skeptics.5
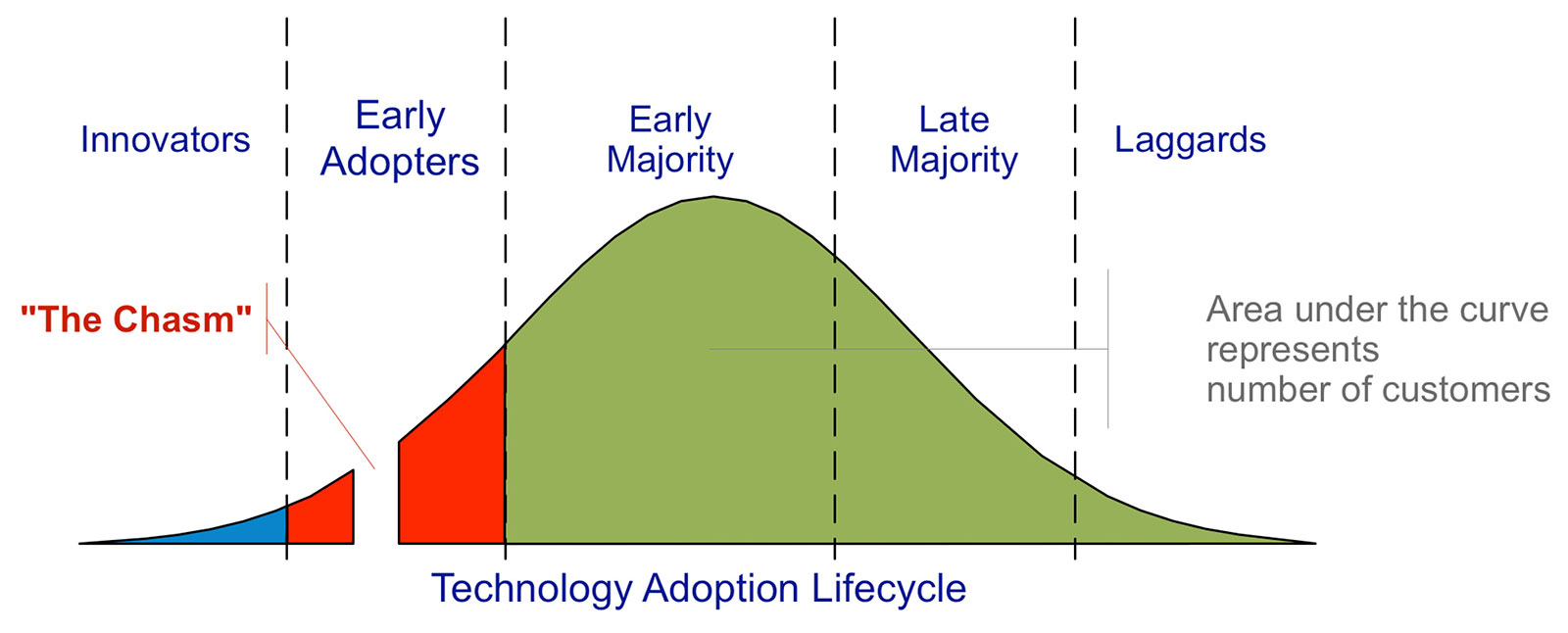
Figure 1: Depiction of the Technology Adoption Lifecycle, adapted from Gregory Moore’s Crossing the Chasm. Source: https://commons.wikimedia.org/wiki/File:Technology-Adoption-Lifecycle.png.
The Infinite Game6 author Simon Sinek references the work of Everett Rogers7 and Frank Bass8 in discussing “The Law of Diffusion of Innovation,” using a similar bell-shaped curve to emphasize that for new ideas or new ways of thinking to stick, innovators should aim for 15–18% market penetration. Crossing this chasm requires an intense initial focus on the 12.5% subset of early adopters. It is only when this subset adopts the idea that the larger segment of the curve represented by the early majority will buy in. Once this tipping point is achieved and the chasm is crossed, new ideas will spread to pragmatists in the late majority and even to the laggards who loudly oppose culture change.9 Both Moore and Sinek emphasize the need to serve these pivotal early adopters with an emphasis on gaining trust and building relationships.
TRUSTING RELATIONSHIPS
The topic of trust in the perioperative space has received significant attention. It would be convenient if trust in health care teams had an agreed-upon definition and validated metrics, but this is sadly not the case; a universal definition is hard to find. Further, the Joint Commission attributes up to 70% of serious medical errors to poor communication.10 Fortunately, the pursuit of a collaborative conflict culture, where team members engage in active listening, open discussion, and demonstrations of mutual respect, has recently been shown to promote civility in health care teams, potentially mitigating the threat of incivility-related patient harm. This focus on multidisciplinary professional relationships encourages productive conflict built upon empathy, humility, and openness to differing opinions.11 By resisting the urge to focus on in-group preservation and instead emphasizing health care professionals’ common bonds in delivering outstanding patient care and our shared fate in the health care system, teams under the overarching umbrella of a collaborative conflict culture achieve high performance and safety by prioritizing civil communication and cultivating trust.12
Interestingly, there has been increasing emphasis on the role of relational leadership in health care. Existing issues of constrained resources, decreasing reimbursement, workforce shortages, etc., were only made worse by the COVID-19 pandemic, forcing leaders to work across silos in new and innovative ways. Relational leadership encourages leaders in complex environments to build and sustain collaborative relationships with individuals and groups across health care systems to incorporate multiple perspectives into decision-making. This focus on long-term organizational health vs. the short-term bottom line is key to sustaining and building resilient organizations.13 Authors have previously argued that anesthesia leaders make outstanding health system leaders because our jobs intrinsically demand clear communication, consensus-building, and collaboration, and our clinical work encompasses every kind of patient and procedure.14 Further, when it comes to patient safety, no other specialty can approach the near six sigma level of safety that “team anesthesia” has created.4 Stated differently, no one in health care does “team” like “team anesthesia.” While most health care workers know their specific niche, no other group of specialists spans the gamut of specialty touchpoints like anesthesia professionals. Breadth of knowledge and diverse experiences are often key to successful leadership, especially in complex and unpredictable environments,15 allowing anesthesia leaders to cultivate trusting relationships across health care systems in a way that few other leaders can. We would argue that it is these trusting relationships that allow anesthesia leaders to identify other “pragmatists in pain”—or early adopters—across our health systems. Furthermore, the cultivation of these trusting relationships allows us to lead effectively in areas we have previously never considered. By re-envisioning anesthesiology’s role from volume-based perioperative professional to orchestrator of value across the care continuum, we can better serve our colleagues and health systems, delivering measurable improvements in patient experience, safety, and efficiency.
THE PATH FORWARD: LEAD INFINITELY
We recently suggested that anesthesia care teams should embrace an infinite mindset to navigate the complexities and challenges of the perioperative space.4 A pillar of Sinek’s infinite game mindset is building trusting teams in pursuit of a just cause. We suggested a new approach to perioperative care entitled “Infinite Anesthesia” with a stated just cause of creating “a mutually supportive workspace that maximizes patient care with every encounter—in a way that appreciates every team member.”4 The Infinite Anesthesia culture of “trust and teamwork” encourages all anesthesia professionals to see one another as respected fellow players in the infinite game of perioperative patient care, rather than rivals, highlighted by intentional and respectful interprofessional dialogue, learning, and team building.4
Our experience over the past year and a half shows us that, while the proposed just cause is indeed inclusive and idealistic, it is not inclusive or idealistic enough. Since the concept of “Infinite Anesthesia” was proposed, hospitals across the country have reached out for information and consultation. The model has even been applied to current anesthesia practices internationally, specifically in the United Kingdom, where an infinite game approach of a tiered system with levels of care based on surgical risk and clinical training has been suggested to decrease surgical wait lists.16 In our own institution, we put our theories into practice with a workshop series entitled “LEAD INFINITELY.”17 Beginning with anesthetists, anesthesiologists, and perioperative nursing and now extending to proceduralists and surgeons, our workshop series based on the infinite mindset approach has reach over 300 perioperative clinicians this year alone. With sessions on collective intelligence and teaming, humility, civility, discovery driven planning, and the infinite game mindset (Table 1), this workshop series has grown steadily at our institution and is now gaining traction in other hospitals across the country. Given that workplace engagement has been shown to promote employee retention,18 the goal of this series is to bring front-line care teams together to educate on leadership and teamwork principles while also strengthening bonds and building respectful and trusting professional relationships. Teams attend this workshop series together, as group discussion and planning are incorporated into every session. Teams graduate from this series equipped with a strategic plan to optimize the patient care their teams deliver by forging trusting and respectful professional relationships to enhance team communication and performance.17
Table 1: Lead Infinitely Workshop Series.
| Leading Collectively | Teaming, collective intelligence, and the mutual learning mindset |
| Leading with Humility | Finding balance between professional will and personal humility |
| Leading with Civility | The price of incivility and benefits of civility in health care teams |
| Leading with Discovery | Managing change through the concepts of discovery driven planning, and “idea flow” |
| Leading Infinitely | Pursuing a just cause, building trusting teams, studying worthy rivals, preparing for existential flexibility, and demonstrating the courage to lead |
Further education related to this approach is now being requested by surgical subspecialties, medical proceduralists such as cardiologists and gastroenterologists, obstetricians and neonatologists, as well as hospital medicine physicians. To meet this demand, single-day workshops incorporating any and/or all of the original five topics are now offered to departments across the institution and customized to the needs of local leadership. Further, school of medicine faculty affairs leaders are now promoting this series to all faculty in both the clinical and research domains and incorporating it into the onboarding process for new hires. Finally, research is now underway to elucidate participants’ perceptions of the course and its impact on daily practice and culture. Initial feedback has included comments that the material is “engaging, relevant, and helpful” and that the message is one that “many need to hear.”17
While the original “Infinite Anesthesia”4 call was to include all anesthesia care team members, we now suggest this concept should include ALL health care teams. Infinite leadership has the potential to catalyze transformation far beyond the confines of the perioperative space. While the original call was idealistic, we now argue that it was not big and bold enough. Anesthesia leaders see the inner workings of the health care system like few others can. We do teams as well as anyone in health care. We should therefore, LEAD in health care like no other group can. Our respectful, trusting, and inclusive care team approach is relevant across all health care settings, and our relationships give us the access and credibility to spread our message FAR beyond the perioperative space. We know where the pain points to operational efficiency lie, and we know the key early adopters we need to target to cross the chasm and broadly spread our patient safety efforts.
“Infinite Anesthesia”4 is too small a concept. We need to think bigger and more boldly. We invite our surgical and medical colleagues and health system partners to join the “Lead Infinitely”17 movement, not as passive stakeholders but as active co-leaders. By embracing infinite leadership, anesthesia leaders can help unlock operational, financial, and clinical gains across the health system. The “Lead Infinitely”17 movement is not ours to own, but ours to share. This movement is not about protecting turf but about building up new leaders across the health care system, regardless of specialty, to deliver and diffuse the just cause of mutually supportive workspaces that maximize patient care while appreciating every team member. The opportunity is big—and the need is urgent. We encourage our anesthesia colleagues in hospital systems across the country and the globe to LEAD INFINITELY,17 both in anesthesia and beyond.
Matthew Sherrer, MD, MBA, FASA, FAACD, is an associate professor at the University of Alabama at Birmingham, Department of Anesthesiology and Perioperative Medicine, Birmingham, AL.
Juhan Paiste, MD, MBA, CPE, is a professor at the University of Alabama at Birmingham, Department of Anesthesiology and Perioperative Medicine, Birmingham, AL.
Dan E. Berkowitz, MB, BCh, is a professor at the University of Alabama at Birmingham, Department of Anesthesiology and Perioperative Medicine, Birmingham, AL.
Richard P. Dutton, MD, MBA, is the chief quality officer for US Anesthesia Partners in Columbia, MD.
Matthew Sherrer, Juhan Paiste, and Dan E. Berkowitz report no conflicts of interest. Richard P. Dutton is a shareholder in US Anesthesia Partners.
REFERENCES
- Companies Market Cap. Market capitalization of Amazon. Available at: https://companiesmarketcap.com/amazon/marketcap/. Accessed August 1, 2025.
- Amazon. Amazon unveils the next generation of fulfillment centers powered by AI and ten times more robotics. Available at: https://www.aboutamazon.com/news/operations/amazon-fulfillment-center-robotics-ai. Accessed August 1, 2025.
- Michigan Journal of Economics. The history of Amazon and its rise to success. Available at: https://sites.lsa.umich.edu/mje/2023/05/01/the-history-of-amazon-and-its-rise-to-success/. Accessed August 1, 2025.
- Sherrer DM, Dutton RP, Kamdar N, et al. The infinite game: one possible future of anesthesia in the United States. Anesth Analg. 2023;137(6):1179–1185. PMID: 37703209.
- Moore, GA. Crossing the chasm: marketing and selling high-tech products to mainstream customers. HarperBusiness; 1991.
- Sinek, S. The infinite game. Portfolio Penguin; 2020.
- Rogers, EM. Diffusion of innovations. Free Press of Glencoe; 1962.
- Bass, FM. A new product growth for model consumer durables. Management Science. 2004;50:1825–1832. https://doi.org/10.1287/mnsc.15.5.215. Accessed September 1, 2025.
- Simon Sinek. How to make a cultural transformation. Available at: https://www.youtube.com/watch?v=N9d0NqSztWA. January 10, 2020. Accessed August 1, 2025.
- Agency for Healthcare Research and Quality. Improving patient safety through provider communication strategy enhancements. Available at: https://www.ahrq.gov/downloads/pub/advances2/vol3/advances-dingley_14.pdf. Accessed September 30, 2025.
- Li R, Choi VK, Gelfand MJ. Ripple effects of hospital team faultlines on patient outcomes. Proc Natl Acad Sci U.S.A. 2023;120(47):e2302341120. https://doi.org/10.1073/pnas.2302341120 (2023).
- Sherrer DM, Peters CB, Mertz BA, et al. Building trusting health care teams. Anesth Analg. 2025;141:1024–1029. PMID: 40408288.
- Hawley R, Wall T. Leading across health care silos: why relational leadership matters? BMJ Leader. 2025;9:1–3. PMID: 38350717
- Conroy JM, Lubarsky D, Newman MF. Anesthesiologists as health system leaders: why it works. Anesth Analg. 2022;134(2):235–240. PMID: 35030118.
- Epstein DJ. Range: why generalists triumph in a specialized world. Riverhead Books; 2019.
- Sherrer DM, Tremper KK, Pandit JJ. The infinite game: opportunities and lessons about possible futures of anesthesia service delivery from the United Kingdom. Anesth Analg. 2025;140:901–905. PMID: 39446660.
- University of Alabama at Birmingham Department of Anesthesiology and Perioperative Medicine. Lead Infinitely. Available at: https://www.uab.edu/medicine/anesthesiology/about/lead-infinitely. Accessed September 30, 2025.
- Xu K, Lei L, Guo Z, et al. Turnover intention among health care workers in Shenzhen, China: the mediating effect of job satisfaction and work engagement. BMC Health Serv Res. 2024;24:1413. PMID: 39548526.
