To address rising maternal mortality, anesthesia professionals must recognize and overcome "wellness bias"—the dangerous assumption that obstetric patients are inherently healthy and resilient. Shifting maternal demographics and underlying chronic conditions necessitate proactive, vigilant clinical monitoring to detect and prevent the rapid decompensation often masked by normal physiological changes of pregnancy.
INTRODUCTION
The United States continues to face rising maternal mortality and severe maternal morbidity (SMM). Sepsis alone now accounts for nearly 13% of maternal deaths, which is on par with hemorrhage and hypertensive disorders.1 What is striking across reviews of maternal deaths is how often these cases are deemed preventable by multidisciplinary review committees. The themes are consistent: delayed recognition, delayed escalation, and interventions initiated only after a patient is already critically ill.
Moving toward forecasting decompensation and earlier intervention requires acknowledgement of two hidden contributors to maternal morbidity and mortality: wellness bias and physiologic masking in pregnancy. These cognitive traps are particularly relevant to anesthesia professionals, who are frequently involved in patient care only once decompensation has already occurred, and who face the daunting task of resuscitating patients who have already lost the reserve that pregnancy physiology once provided.
“WELLNESS BIAS” AND THE “NORMALIZATION OF DEVIANCE” IN PREGNANCY CARE
“Wellness bias” is the subconscious tendency among clinicians to assume that young, healthy-appearing pregnant patients are well, even when symptoms suggest otherwise.2 This can extend to medically complex pregnant patients with pre-existing conditions, for whom wellness bias can result in minimization of the real medical conditions that actually make the pregnancy extremely high risk. This is particularly worrisome in a progressively older and obese obstetric population, where the risks of SMM and mortality compound and potentially magnify complications outside of what would be recognized as a normal healthy pregnant person.
Wellness bias inherently lowers clinical suspicion for serious conditions. For example, in obstetric patients with infection or sepsis, wellness bias can lead to minimization of concerns voiced by the patients, or dismissal of abnormal vital signs and laboratory values. It is this pregnancy-related optimism that explains why tachycardia is often dismissed as “normal pregnancy,” why shortness of breath may simply be attributed to the gravid uterus, or why postpartum fatigue is accepted at face value rather than evaluated as possible sepsis or cardiomyopathy.
“Normalization of deviance” is a related phenomenon through which safety standards gradually erode over time after repeated encounters without negative outcomes.3 Both wellness bias and normalization of deviance are commonly observed in obstetric and pediatric medicine, where abnormal outcomes are relatively infrequent and most patients appear healthy. Normalization of deviance can include disregarding alarms, bypassing protocols, or skipping checklists; over time, unintentional denial, dismissal, and ultimately delays can lead to morbidity and even mortality. Furthermore, systemwide and individualized wellness biases can be compounded by unconscious biases toward marginalized populations, further widening disparities in diagnosis and treatment. Left unaddressed, these cognitive traps delay recognition and escalation of care, placing both maternal and fetal outcomes at risk. For anesthesia professionals, delayed recognition of serious medical conditions may mean that involvement of the anesthesia team only occurs once the patient is in extremis, when intubation, hemodynamic support, or transfusion carry higher risks and lower margins for safety.

MATERNAL PHYSIOLOGY THAT MASKS DETERIORATION
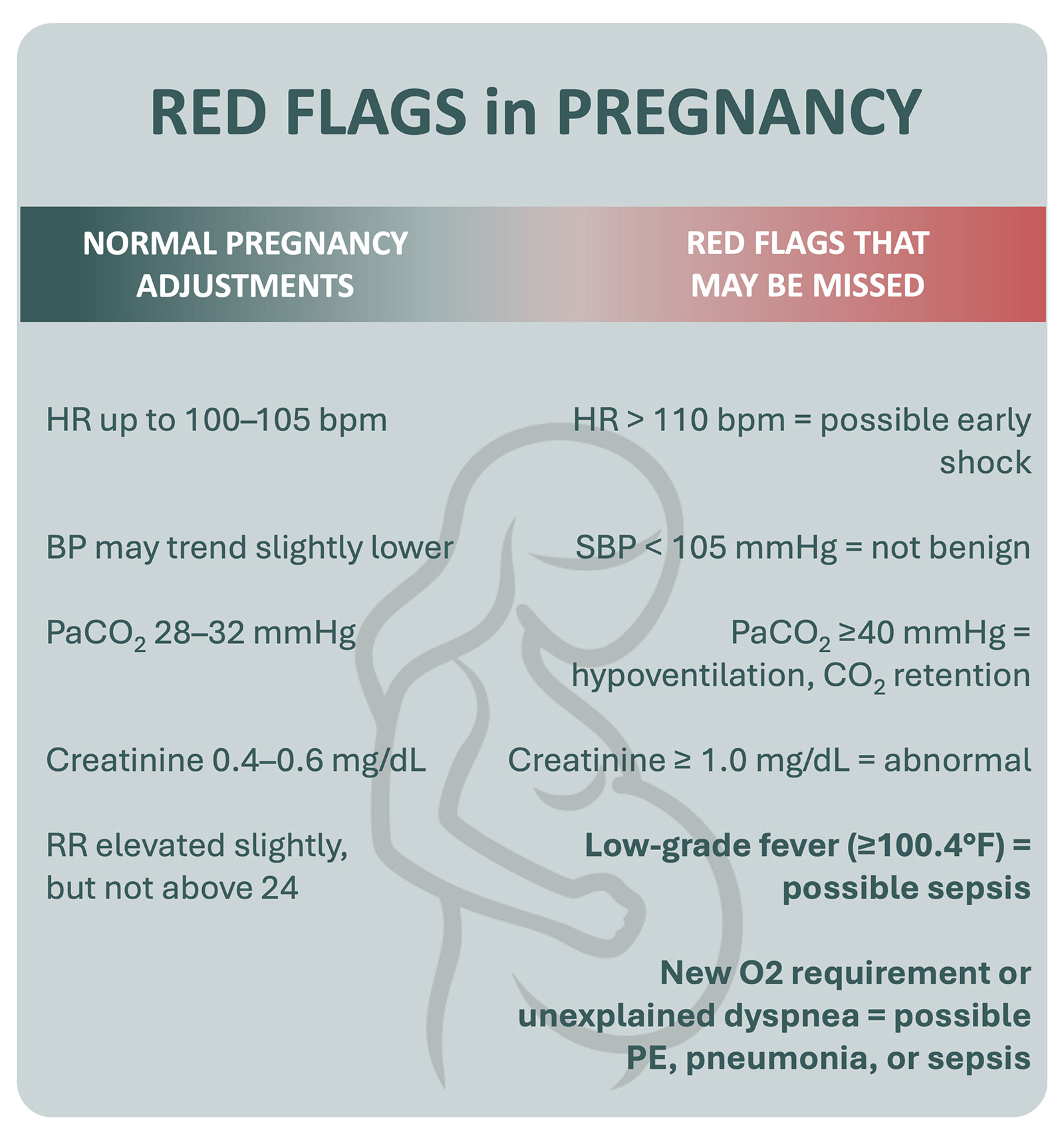
The physiology of pregnancy can create a dangerous situation where patients may appear stable until they suddenly are not, particularly when systems rely on nonpregnant thresholds for alerts and when the health care team is not trained and actively aware of early signs of decompensation in a pregnant patient. Clinical understanding of maternal vital signs and physiology is critical to early recognition. For example, while expanded plasma volume and reduced systemic vascular resistance in pregnancy may result in a mildly increased maternal heart rate and lower blood pressure, frank tachycardia and hypotension may be erroneously interpreted as “normal.” Similarly, a blunted febrile response in pregnancy means infection may present without fever, with 20% of maternal sepsis cases presenting without a fever.2
Equally concerning is the lack of awareness of, and system safety alerts regarding, laboratory value differences in pregnancy. There are scoring processes created specifically for obstetric patients, like “MEWS” or “MEWT” that predict deterioration and alert teams of vital sign abnormalities in pregnancy.4-5 These scores adopt vital sign parameters that are more specific to pregnancy than adult scoring tools. Misinterpretations of maternal physiology can also lead to delays. One example is a common presumption that tachypnea is physiologic to pregnancy. This is incorrect, and while there is a compensatory rise in respiratory rate, it should not be over 24. In addition to the differences in vital sign parameters, there are differences in laboratory values that need to be adjusted for pregnancy. For instance, a baseline creatinine in pregnant patients of 0.4–0.8 mg/dL means that a “normal” value of 1.0 mg/dL reflects developing acute kidney injury. During pregnancy, a normal PaCO₂ is ~32–35 mmHg, so a “normal” PaCO2 of 40 mmHg is in fact abnormal during pregnancy, signaling hypoventilation, CO2 retention, and possible impending respiratory collapse. Expanded intravascular volume and the resultant dilutional anemia of pregnancy can obscure bleeding. The hypercoagulable state of pregnancy makes disseminated intravascular coagulopathy (DIC) harder to recognize until well-advanced. In the third trimester, a normal maternal fibrinogen should be greater than 400 mg/dl, even though a normal nonpregnant adult value is 200 mg/dl.6-9 Unfortunately, most lab values are not adjusted for pregnancy, nor are critical alerts built into health care systems to alert to these pregnancy-specific lab value aberrations. There also remains a paucity of maternal safety infrastructure and alerts like those that exist for nonpregnant adults, forcing obstetric care teams to rely on individuals to remember these differences. Investing in electronic health record (EHR) systems with maternal-specific alerts for both vitals and lab results is essential for any health system providing care to obstetric patients, and should be extended to emergency departments, operating rooms, and intensive care units (ICUs) where these patients may receive care.10
BIAS IN WITHHOLDING MATERNAL DIAGNOSTICS AND THERAPY
Wellness bias can also extend to overemphasizing theoretical fetal risk at the expense of maternal safety. Too often, diagnostic tools and therapeutic interventions are delayed or withheld in pregnancy because of perceived teratogenicity, radiation risk, or concerns regarding drug transfer to breastmilk, despite evidence that timely maternal intervention is the best protection for both mother and baby. Examples include not obtaining a chest x-ray, pulmonary angiography CT, or other indicated imaging; delaying indicated surgery or cardiovascular treatments; and hesitating to give antibiotics, vasopressors, or other indicated medications. These delays in treatment only compound the delay in recognition of serious medical conditions and contribute to increased morbidity and mortality. In fact, the failure to treat maternal disease aggressively is arguably itself a form of bias. In every major mortality review, maternal stabilization is cited as the most important determinant of fetal survival and barring a few exceptions to known fetal risk (such as the administration of medications known to be teratogenic, when suitable alternatives exist), pregnant individuals should receive the standard-of-care evaluation and treatment.11-15
SYSTEM-LEVEL CONTRIBUTORS AND EQUITY CONSIDERATIONS
In addition to wellness bias and physiologic masking, demographic and social determinants compound risk as maternal mortality is not distributed evenly throughout the population. Pregnant patients 40 and older have nearly a sevenfold increase in mortality compared to those under 25, as age-related comorbidities and reduced physiologic reserve amplify risk during pregnancy.16-18 Pregnancy-related mortality also increases with higher body mass index (BMI), with women with a BMI ≥ 40 kg/m2 facing a 5–6 fold higher risk compared with those with a lower BMI. For anesthesia professionals, this translates into greater potential for a difficult/failed airway, altered pharmacokinetics, and increased hemodynamic instability under stress. Race and ethnicity also influence maternal risk: Black women have a pregnancy-related mortality rate three to four times higher than White women, with the highest risk observed in Black women over age 40.16-18 American Indian and Alaska Native women also face a more than twofold increase. These inequities persist even when controlling for socioeconomic status and comorbidities, reflecting systemic bias and barriers to care. Patients who are uninsured, underinsured, or rely on state-funded health programs face a two- to four-fold higher risk of pregnancy-related mortality compared with those with private insurance. Limited access to preventive care, delayed escalation of care, and systemic barriers compound the danger.16-18
IMPLICATIONS FOR ANESTHESIA TEAMS
For anesthesia teams, these biases and physiologic challenges converge at the worst possible moment: the crashing patient with minimal reserve. Intubation is more dangerous, resuscitation more difficult, and transfusion more urgent when recognition is delayed.
ANESTHESIA PROFESSIONALS SHOULD KEEP THE FOLLOWING RECOMMENDATIONS IN MIND
- Do not accept “normal” at face value. Remember maternal-adjusted vitals and lab values.
- Advocate for early escalation. Push for sepsis bundle activation, massive transfusion protocol initiation, and/or timely ICU transfer as appropriate.
- Encourage early neuraxial anesthesia when appropriate. Timely epidural placement may be preferable to automatically waiting until active labor, when worsening patient status (e.g., HELLP syndrome or sepsis) may increase the risk of neuraxial anesthesia or even preclude its placement.
- Support postpartum vigilance. The postpartum period is where patients can decompensate under decreased monitoring and higher nurse staffing ratios. Discharge education regarding warning signs of serious postpartum complications is essential.
- Promote timely diagnostics and interventions. Speak up if maternal diagnostics or therapies are being deferred inappropriately out of fetal concern—the safest fetus is one with a stable mother.
SYSTEM-LEVEL SOLUTIONS
System-level changes are required to fully counteract bias and physiologic masking:
- Embed pregnancy-adjusted thresholds into EHR early warning systems. Reliance on nonpregnant normal lab value and vital sign cutoffs is unsafe in obstetrics.
- Use simulation to expose wellness bias. Train teams with scenarios where a “well-appearing” patient deteriorates rapidly.
- Normalize anesthesia involvement in early huddles. Bring anesthesia in early, not just when the patient is coding.
- Adopt bundles with explicit anesthesia triggers. Hemorrhage, hypertension, and sepsis pathways should have delineated roles for anesthesia professionals from the start.
- Institutionalize maternal-first counseling. Establish standards that reinforce maternal stabilization as the priority in decision-making regarding diagnostics and treatment.
CONCLUSION
Maternal mortality and SMM will not be reduced without addressing embedded wellness bias and the unique physiology of pregnancy. These silent drivers of delay are within our power to fix—by recalibrating our thresholds, building better systems, and challenging our assumptions.
For anesthesia professionals, the message is urgent: your vigilance, your voice, and your leadership in early recognition can change the trajectory of care. By speaking up when “normal” isn’t normal, by advocating for appropriate diagnostics and therapies, and by partnering with obstetrics to counteract bias, we can better forecast and prevent decompensation, prioritize early intervention, preserve maternal safety, and close the gap on preventable harm.
Courtney Martin, DO, MHA, FACOG, is a board certified, MIGS-certified OB/GYN hospitalist.
The author reports no conflicts of interest.
REFERENCES
- Bauer ME, Albright C, Prabhu M, Heine RP, et al. Alliance for Innovation on Maternal Health: Consensus bundle on sepsis in obstetric care. Obstet Gynecol. 2023;142(3):481-492. PMID: 37590980
- California Maternal Quality Care Collaborative. Improving diagnosis and treatment of obstetric sepsis, Version 2.0 Toolkit. Palo Alto, CA: CMQCC; 2025.
- Banja J. The normalization of deviance in health care delivery. Bus Horiz. 2010;53:139–148. PMID: 20161685
- Arnolds DE, Carey KA, Braginsky L, et al. Comparison of early warning scores for predicting clinical deterioration and infection in obstetric patients. BMC Pregnancy Childbirth. 2022;22:295. PMID: 35387624
- Chimwaza Y, Hunt A, Oliveira-Ciabati L, et al. Early warning systems for identifying severe maternal outcomes: using data from the 2017 WHO Global Maternal Sepsis Study. BMJ Glob Health. 2024;9:001114. PMID: 39720608
- Abbassi-Ghanavati M, Greer LG, Cunningham FG. Pregnancy and laboratory studies: a reference table for clinicians. Obstet Gynecol. 2009;114:1326–1331. PMID: 19935037
- Cunningham FG, Leveno KJ, Bloom SL, et al. Williams Obstetrics. 26th ed. New York, NY: McGraw-Hill; 2022.
- Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A. Physiological changes in pregnancy. Cardiovasc J Afr. 2016;27(2):89-94. PMID: 27213856
- Chestnut DH, Wong CA, Tsen LC, et al., eds. Chestnut’s Obstetric Anesthesia: Principles and Practice. 6th ed. Philadelphia, PA: Elsevier; 2020.
- Martin C, Pappas J, Johns K, et al. Semiautonomous treatment algorithm for the management of severe hypertension in pregnancy. Obstet Gynecol. 2021;137:211–217. PMID: 33416295
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 211: Critical care in pregnancy. Obstet Gynecol. 2019;133(5):e303-e319. PMID: 31022122
- Society for Maternal-Fetal Medicine (SMFM), Plante LA, Pacheco LD, Louis JM. SMFM Consult Series #47: Sepsis during pregnancy and the puerperium. Am J Obstet Gynecol. 2019;220(4):B2-B10. PMID: 30684460
- California Pregnancy-Associated Mortality Review. Pregnancy-Related Deaths in California, 2011–2019. Sacramento, CA: California Department of Public Health; 2022
- California Department of Public Health. Pregnancy-Related Mortality (California dashboard; 2009–2022). Sacramento, CA: California Department of Public Health; updated June 10, 2025.
- Wolfson CL, Angelson JT, Forrest AD, et al. Comorbidities and pregnancy-related risk factors in patients with severe maternal morbidity: application of a validated obstetrical comorbidity scoring system to a surveillance-identified population. Healthcare (Basel). 2025;13:2351. PMID: 41008483
- Nam JY. Validation of the obstetric comorbidity index for predicting severe maternal morbidity and mortality in South Korea. Sci Rep. 2025;15:98310. PMID: 40325179
- Henderson I, Lynch R, Gerry S, et al. Severe maternal morbidity in the high-income setting: a systematic review of composite definitions. eClinicalMedicine. 2025;81:103105. PMID: 40034571
