Methamphetamine Substance Use Disorders (SUD) have been on the rise in the United States. Patients who present with this particular SUD present with challenges for the anesthesia provider. Managing these patients with appropriate medications and actions will help to reduce the risk of patients developing untoward effects. This review article details medications and actions most appropriately suited for methamphetamine SUD patients who require anesthetic care.

Substance Use Disorders (SUD) are a topic of increasing concern in the United States and continue to impact families and communities. Of the reported 329.9 million population of the United States in 2014, 21.5 million people were diagnosed with SUD.¹ Methamphetamine accounts for approximately 1.6 million of the 21.5 million individuals who misuse substances in this country. According to the National Institute on Drug Abuse, 0.6 percent of the population reported using methamphetamines.² That number is likely drastically under-reported due to the criminal nature and stigma related to diseases associated with drug use. A survey of 5,000 participants found that approximately 81% of patients provide false information to their providers regarding substance abuse.³ The most common reason given in the study was that patients did not want to be “judged.”³ Therefore, it would be prudent for an anesthesia professional to be aware that patients presenting for elective cases to the operating room may conceal the truth with regard to their illicit substance use.
The COVID-19 pandemic also has the potential to increase the likelihood of encountering a patient with a SUD. Many patients who had previously maintained sobriety are now experiencing relapse due to increased stress, social isolation, and economic strain.⁴ It is important to remember that SUD still exist as an epidemic even during the pandemic. The use of substances, like methamphetamine, has not gone away or decreased, but rather increased in frequency.⁴ It is important for each anesthesia professional to be aware of the potential lethal effects of methamphetamine use in the preoperative setting, the consequences of which may include hypertensive crisis, cardiovascular collapse from hypotension, and death.⁵ Adhering to practice from the most up to date literature may abate the potential morbidity and mortality and ensure the most appropriate care of patients with this particular SUD.
Pharmacology of Methamphetamines
The International Union of Pure and Applied Chemistry (IUPAC) name for methamphetamine is (2S)-N-methyl-1-phenylpropan-2-amine.⁶ Though the mechanism of action is not fully understood, methamphetamine causes a release of the endogenous monoamines dopamine, norepinephrine, and serotonin (figure 1).
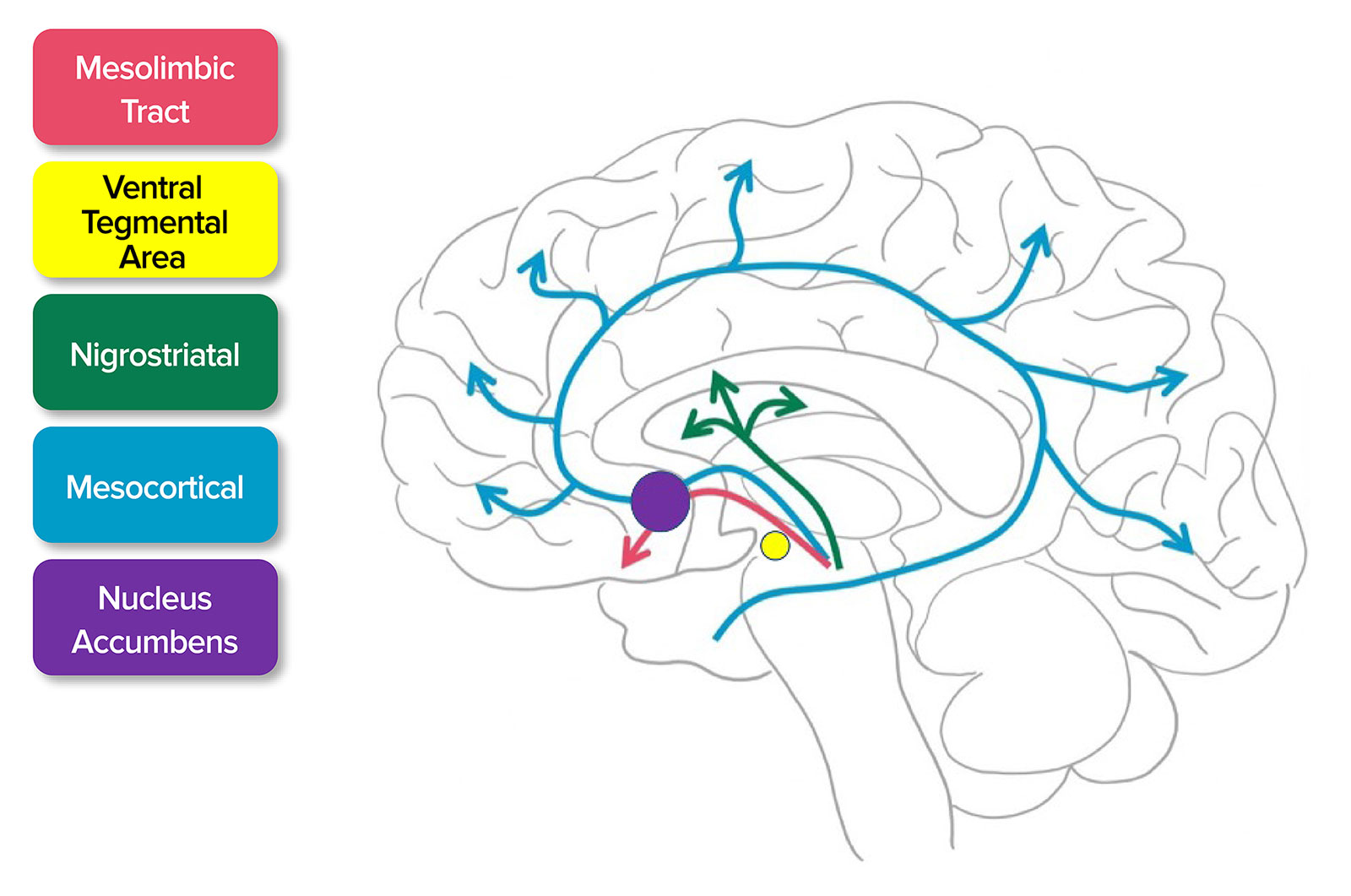
Figure 1. Release of Dopamine. Dopamine activates the mesolimbic, mesocortical tract, and nigrostriatal pathways. This pathway extends from ventral tegmental areas to the nucleus accumbens which is responsible for the euphoric feeling after using methamphetamine.7
Source: Adapted from SITNBoston. Haynes et al, 2018.7
https://sitn.hms.harvard.edu/flash/2018/dopamine-smartphones-battle-time/
Accessed April 16, 2021.
Once released, the monoamines bind to their appropriate postsynaptic receptors to affect a response. The release of dopamine into the nucleus accumbens follows the same pathway for natural rewards like social interaction, sex, eating, and exercise, but the stimulation from methamphetamine causes 2 to 10 times more dopamine to be released from endogenous stores than the natural rewards resulting in a dopamine release above 1000% basal levels.7-10 Methamphetamine also interacts with the endogenous opioid system further increasing endorphins in the nucleus accumbens which mediates reward centers.11
Lastly, the scarcity of dopamine caused by the body’s inability to recover from the massive release of monoamines from storage vesicles causes feelings of depression and withdrawal which can further induce drug-seeking behaviors.12 These physiologic changes combined create an almost manic-depressive state in patients which can create a vicious cycle of misuse.
The peripheral action of monoamines culminates in a diffuse and complex chain of systemic events.11 Those intoxicated with methamphetamines experience a variety of signs and symptoms (table 1).
Table 1. Signs and Symptoms of Methamphetamine Intoxication.11,13,14
| Signs of Methamphetamine Intoxication According to Category |
| Central Nervous System |
| Agitation |
| Restlessness |
| Mydriasis |
| Seizures |
| Hyperthermia |
| Anxiety |
| Increased alertness |
| Hallucinations |
| Psychosis |
| Cardiothoracic |
| Hypertension |
| Tachycardia |
| Dysrhythmia |
| Malignant arrhythmia |
| Myocardial infarction |
| Coronary vasospasm |
| Aortic dissection |
| Bronchodilation |
| Acute Respiratory Distress Syndrome |
| Pulmonary arterial hypertension |
| Right heart failure |
| Sudden cardiac arrest |
| Death |
| Diaphoresis |
| Musculoskeletal |
| Rhabdomyolysis |
| Severe muscle spasms |
| Other |
| Ischemic colitis |
| Metabolic acidosis |
| Placental abruption -> fetal death |
Hyperthermia is a common symptom experienced in these patients, which seems to be related to muscular activity, and therefore antipyretics will have no impact in decreasing body temperature.13 An alarming medical concern with methamphetamines is abrupt cardiac arrest following a physical altercation. Isovolumetric muscle contractions can lead to severe acidosis, rhabdomyolysis, hyperkalemia, and sudden asystolic cardiac arrest.13,15
Pharmacokinetics of Methamphetamines
Pharmacokinetics and metabolism of methamphetamine are highly dependent on the route of administration and the dose, or repeated doses. Methamphetamine elimination occurs via cytochrome CYP2D6 in the hepatic pathway and several renal pathways. Excretion occurs in the first 20 hours but is highly dependent on urine pH. For alkaline urine, excretion can be as low as 2% whereas with acidic urine this can be as high as 76%.16,17 The duration of action of methamphetamine is usually around 24 hours. However, elimination and clinical effect vary highly from person to person with some withdrawal symptoms persisting for up to 10 days.13,16,18
Detection of methamphetamine in the clinical setting is via serum or urinalysis. If a patient is using methamphetamine, they may test positive for either methamphetamine or the metabolized drug of amphetamine.16,17 At this time, there are no quantitative toxicology screenings that could equate to clinical intoxication or severity of physiologic responses under anesthesia. Consequently, it is difficult to determine the associated risks under anesthesia for any patient who tests positive for methamphetamine use.
Guidelines and Precautions
Anesthesia care of the patient under the influence of methamphetamine is centered around a few core concepts. If the patient is acutely intoxicated and requiring emergent surgery, providers should avoid physically restraining these patients because any intervention that leads to intense muscle contractions could cause cardiovascular collapse.13,15 Instead, chemical restraint via sedation with benzodiazepines is the primary therapy. The literature recommends administering midazolam 2mg intravenously every 8 to 10 minutes until the patient is no longer aggressive. Some patients may require up to 20mg.13 If benzodiazepines are not effective in treating psychosis, secondary agents such as haloperidol may be given. Benzodiazepines and haloperidol mitigate the reciprocal effect of methamphetamine by antagonizing the activity of dopamine in the central nervous system.19
Hypertensive patients will most likely see a return to baseline after administration of sedating agents; however, anesthesia professionals may note refractory hypertension in some patients. In these cases, a variety of medications may be used to treat hypertension (table 2).
Table 2. Medications and Considerations for Treatment of Methamphetamine-associated Hypertension.13,14,19,20-22
| MEDICATION |
CONSIDERATIONS |
| 1. MIDAZOLAM | Repeated dosing required for sedation, high doses of midazolam may cause respiratory compromise |
| 2. HALOPERIDOL | Risk of QT prolongation, risk of Neuroleptic Malignant Syndrome, may trigger extrapyramidal symptoms |
| 3. DEXMEDETOMIDINE | Few studies for safety in obstetric patients |
| 4. NITROGLYCERINE | Decreases blood pressure, may cause slight reflex tachycardia |
| 5. NITROPRUSSIDE | Decreases blood pressure with reflex tachycardia, may cause cyanide toxicity |
| 6. PHENTOLAMINE | Anesthesia professional may not have phentolamine available for use |
| 7. NICARDIPINE (DIHYDROPYRIDINE CCB) | Decreases blood pressure with reflex tachycardia |
| 8. VERAPAMIL (NON-DIHYDROPYRIDINE CCB) | Less vasodilatory effect with slight reflex tachycardia or may cause severe bradycardia. |
| 9. LABETALOL | May cause coronary spasm. Can cause hypertension related to unopposed alpha stimulation. |
CCB = Calcium Channel Blocker
The concept of “unopposed alpha stimulation” with the use of beta-blocking agents is becoming increasingly controversial. Some authors have published systemic reviews with scant adverse outcomes and have observed no untoward outcomes when using nonselective beta-blocking agents such as labetalol.22 Furthermore, beta-blockers have been used to treat other hyperadrenergic conditions such as thyrotoxicosis.22 However, the American College of Cardiology Foundation with the American Heart Association have stated in their most recent executive summary from 2014 that patients demonstrating acute signs of intoxication should not be given beta-blockers due to the possibility of potentiating coronary spasm.23 Therefore, suppressing the catecholamine surge with benzodiazepines is still the primary treatment for methamphetamine hypertension.13
Methamphetamine SUD patients who require immediate surgical intervention should be monitored closely for hypotension related to catecholamine depletion. Insertion of an arterial line may be prudent. If hypotension is encountered, treatment with direct-acting vasopressors such as norepinephrine, epinephrine, dopamine, or phenylephrine may be considered.13,24 Although spinal or epidural anesthesia is not contraindicated, many anesthesia professionals choose to avoid neuraxial anesthesia during the anesthetic due to persistent hypotension caused by the sympathectomy despite treatment with vasopressors.
Methamphetamine SUD patients have an increased risk of developing rhabdomyolysis. This multifactorial problem is likely due to a decrease in fluid intake while intoxicated, vasoconstriction from decreased perfusion, and a direct toxic effect on skeletal muscle.25 Succinylcholine may potentiate rhabdomyolysis and is considered a relative contraindication for airway management. Therefore, rocuronium or vecuronium is the paralytic of choice and even more favorable if sugammadex is available to the clinical provider.13 If the patient does develop rhabdomyolysis, administering fluid boluses as indicated is appropriate.13 In addition, clinicians should adjust the ventilator settings to avoid metabolic acidosis.13 Failure to treat any patient aggressively could lead to an irreversible progression of symptoms and may lead to patient death.13
Beyond acute intoxication, some patients may be taking chronic amphetamines as treatment modalities for diagnosis such as attention deficit hyperactivity disorder. Researchers indicate that there is no increased risk of labile blood pressure under anesthesia for this patient subsect. Therefore, patients who are taking amphetamines as part of their treatment regimen may continue their medication perioperatively without pause.26,27
Considerations for the Parturient
Pregnant women who use methamphetamine may present with hypertension, premature rupture of membranes, hemorrhage, or placental abruption.28 If the patient is acutely agitated, benzodiazepines are the best treatment option, especially compared to physical restraint prior to induction. Previous case reports from the 1960s listed benzodiazepines as a significant contributing factor of congenital malformations related explicitly to cleft palate and heart defects. Despite flaws in previous research suggesting a link between benzodiazepines and congenital malformations, a deep aversion to expose pregnant women resulted in a lack of further research.29,30 Recently, more robust data has emerged and several studies have indicated there are no correlations between most benzodiazepines and congenital malformations taken either immediately before surgery or to control anxiety symptoms during the pregnancy.29,31-33 It is unwise for clinicians to withhold benzodiazepines for agitated methamphetamine parturient since the mother is still at risk of cardiovascular collapse with struggle, which could be fatal to both patients. However, the anesthesia professional may prefer to give haloperidol to patients in their first trimester.34 Ketamine is not generally used due to possible catecholamine surge and subsequent hypertension.22
Anesthesia professionals concerned about drug trapping in the newborn may also be hesitant to administer benzodiazepines. Researchers have shown that the increased bio-availability may cause newborns to have three to four times the levels of benzodiazepines in their system when compared to their mothers.35 However, at low doses (0.02–0.025mg/kg) of midazolam, there are no differences in Apgar scores in the newborn following pre-cesarean administration.28,30 The parturient is also at risk of cardiovascular collapse from intense muscle contraction from physical restraint. Since this could be fatal to both mother and newborn, it may still be prudent to sedate agitated pregnant patients via chemical restraint and tend to the respiratory status of the newborn after delivery.
Serotonin Toxicity
Serotonin toxicity, also referred to as serotonin syndrome, is an increase in serotonergic activity in the central nervous system that has the potential to be fatal.36 Serotonin toxicity is a predictable consequence of excess serotonergic activity in the central nervous system and peripheral receptors leading to a variety of symptoms caused by the release of excess serotonin such as agitation, hypertension, tachycardia, and diaphoresis. There have been cases of serotonin toxicity from a single ingestion of methamphetamine.37 Serotonin toxicity may also be precipitated by tramadol, meperidine, opioids (e.g., fentanyl), and methylene blue.36,38,39 Fentanyl is of particular importance to the anesthesia professional since it is one of the more common opioid medications used in the operating room.
If anesthesia professionals encounter a methamphetamine SUD patient who is experiencing serotonin toxicity, benzodiazepines are recommended as the first line of treatment for both. However, unlike methamphetamine intoxication, serotonin toxicity may also be treated with non-selective serotonin antagonists such as cyproheptadine and risperidone. Serotonin toxicity may also be treated with a postsynaptic dopamine blocking agent such as chlorpromazine.40
Summary
Methamphetamine SUD is on the rise, even more so with the COVID-19 pandemic increasing stress, social isolation, and economic strain. Patients who present with this particular SUD present with challenges for the anesthesia provider. As a reminder, chemical restraint should be used as opposed to physical restraints to limit muscle contractions, which can lead to cardiovascular collapse. Direct-acting vasopressors are often needed as profound hypotension is likely, but, if the patient is hypertensive, beta-blockers are to be used with caution. Finally, methamphetamine SUD patients may present with rhabdomyolysis or serotonin toxicity; providers should avoid administering associated triggering medications.
Jennifer Krogh, MSN, CRNA, is a DNP student at Yale School of Nursing, Orange, CT.
Jennifer Lanzillotta-Rangeley, PhD, CRNA, is an assistant professor at the University of Cincinnati College of Nursing in Cincinnati, Ohio, USA and is the Chief of Anesthesiology at Highland District Hospital, Hillsboro, Ohio.
Elizabeth Paratz, MD, is a cardiologist at St. Vincent’s Hospital Melbourne, Victoria, Australia.
Lynn Reede, DNP, CRNA, is an associate clinical professor in School of Nursing Nurse Anesthesia Program at Northeastern University, Boston, MA.
Linda Stone, DNP, CRNA, is the assistant program administrator and an assistant clinical professor for the University of North Carolina Greensboro DNP nurse anesthesia concentration, Greensboro, NC.
Joseph Szokol, MD, is the chief health policy officer of the American Society of Anesthesiologists, clinical professor of Anesthesiology and executive director of mentorship and physician development at Keck Medicine of USC, Los Angeles, CA.
Laura Andrews, PhD, is an associate professor and specialty director of Adult/Gerontology Acute Care Nursing at Yale School of Nursing, Orange, CT.
Joan Kearney, PhD, APRN, FAAN, is an associate professor at Yale University, West Haven, CT.
The authors have no conflicts of interest.
References
- Lipari RN, Van Horn SL. Trends in substance use disorders among adults aged 18 or older. The CBHSQ Report. 2017.
- National Institute on Drug Abuse. What is the scope of methamphetamine misuse in the United States? https://www.drugabuse.gov/publications/research-reports/methamphetamine/what-scope-methamphetamine-misuse-in-united-states. Accessed November 6, 2019.
- Levy AG, Scherer AM, Zikmund-Fisher BJ, Larkin K, Barnes GD, Fagerlin A. Prevalence of and factors associated with patient nondisclosure of medically relevant information to clinicians. JAMA Netw Open. 2018;1:1–8
- Wan W, Long H. ‘Cries for help’: drug overdoses are soaring during the coronavirus pandemic. Washington Post. July 1, 2020.
- Gao W, Elkassabany N. Drugs of Abuse. Gupta A, Singh-Radcliff, N. Pharmacology in anesthesia practice. New York, NY: Oxford University Press. 2013;391–411.
- National Center for Biotechnology Information. PubChem compound summary: Methamphetamine. https://pubchem.ncbi.nlm.nih.gov/compound/methamphetamine. Accessed April 29, 2019.
- Haynes T. Dopamine, smartphones, and you: a battle for your time. Science in the News. http://sitn.hms.harvard.edu/flash/2018/dopamine-smartphones-battle-time/. Accessed August 12, 2020.
- Allerton M, Blake W. The “Party Drug” crystal methamphetamine: Risk factor for the acquisition of HIV. Perm J. 2008;12:56–58.
- Beaulieu P. Anesthetic implications of recreational drug use. Can J Anaesth. 2017;64:1236–1264.
- National Institute on Drug Abuse. Methamphetamine. https://www.drugabuse.gov/publications/drugfacts/methamphetamine. Accessed November 6, 2019.
- Courtney KE, Ray LA. Methamphetamine: an update on epidemiology, pharmacology, clinical phenomenology, and treatment literature. Drug Alcohol Depend. 2014;143:11–21.
- Kish SJ. Pharmacologic mechanisms of crystal meth. CMAJ. 2008;178:1679–1682.
- Boyer EW, Seifert SA, Hernon C. Methamphetamine: acute intoxication. UpToDate. Ed. Traub SJ, Burns MM: UpToDate; 2019. https://www.uptodate.com/contents/methamphetamine-acute-intoxication. Accessed October 24, 2019.
- Paratz ED, Cunningham NJ, MacIsaac AI. The cardiac complications of methamphetamines. Heart Lung Cir. 2016;25:325–332.
- National Criminal Justice Reference Service. White paper report on excited delirium syndrome. Updated September 2009. https://www.ncjrs.gov/App/Publications/abstract.aspx?ID-260278. Accessed September 28, 2019.
- Volkow ND, Fowler JS, Wang G, et al. Distribution and pharmacokinetics of methamphetamine in the human body: clinical implications. PLoS One. 2010;5:1–6
- Oyler JM, Cone EJ, Joseph RE, Moolchan ET, Huestis MA. Duration of detectable methamphetamine and amphetamine excretion in urine after controlled oral administration of methamphetamine in humans. Clin Chem. 2002;48:1703–1714
- Huestis MA, Cone EJ. Methamphetamine disposition in oral fluid, plasma, and urine. Ann NY Acad Sci. 2007;1098:104–121.
- Richards JR, Derlet RW, Albertson TE. Methamphetamine toxicity treatment and management. Medscape. https://emedicine.medscape.com/article/820918-treatment#d10. Accessed December 7, 2018.
- Johnson BA, Wells LT, Roache JD, et al. Isradipine decreases the hemodynamic response of cocaine and methamphetamine. Am J Hypertens. 2005;18:813–822.
- Lam v, Shaffer RW. Management of sympathomimetic overdose including designer drugs. Hyzy RC, McSparron J. Evidence-based critical care: a case study approach. 2nd Edition. Switzerland. Springer Nature Switzerland. 2020.
- Richards JR, Albertson TE, Derlet RW, et al. Treatment of toxicity from amphetamines, related derivatives, and analogues: a systematic clinical review. Drug Alcohol Depend. 2015;150:1–13
- Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with Non-ST-elevation acute coronary syndromes. J Am Coll Cardiol. 2014;64:e139–e288.
- Selvaggi G, Spagnolol AG, Elander A. A review of illicit psychoactive drug use in elective surgery patients: Detection, effects, and policy. Int J Surg. 2017;48:160–165.
- Eilert RJ, Kliewer ML. Methamphetamine-induced Rhabdomyolysis. Int Anesthesiol Clin. 2011;49:52–56.
- Cartabuke RS, Tobias JD, Rice J, Turmin D. Hemodynamic profile and behavioral characteristics during induction of anesthesia in pediatric patients with attention deficit hyperactivity disorder. Pediatr Anesth. 2017;27:417–424.
- Fischer SP, Schmiesing CA, Guta CG, Brock-Utne JG. General anesthesia and chronic amphetamine use: Should the drug be stopped preoperatively? Anesth Analg. 2006; 103:203-206.
- Pham T, Tinajero Y, Mo L, et al. Obstetrical and perinatal outcomes of patients with methamphetamine positive drug screen on labor and delivery. Am J Obstet MFM. 2020;2:1–7.
- Senel AC, Mergan F. Premedication with midazolam prior to caesarean section has no neonatal adverse effects. Braz J Anesthesiol. 2014;64:16–21.
- Shergill AK. Guidelines for endoscopy in pregnant and lactating women. Gastrointest Endosc. 2012;76:18–24.
- Flölich MA, Burchfield DJ, Euliano T, Canton D. A single dose of fentanyl and midazolam prior to Cesarean section have no adverse neonatal effects. Can J Anesth. 2006;53:79–85.
- Bellantuono C, Tofani S, Sciascio GD, Santone G. Benzodiazepine exposure in pregnancy and risk of major malformations: A critical overview. Gen Hosp Psychiatry. 2013;35:3–8.
- Upadya M, Saneesh P. Anaesthesia for non-obstetric surgery during pregnancy. Indian J Anaesth. 2016;60:234–241.
- Betcher HK, Montiel C, Clark CT. Use of antipsychotic drugs during pregnancy. Clin Schizophr Relat Psychoses. 2019;6:17–31.
- Radojcic MR, Marroun HE, Miljkovic B, et al. Prenatal exposure to anxiolytic and hypnotic medication in relation to behavioral problems in childhood: a population-based cohort study. Neurotoxicol Teratol. 2017;61:58–65.
- Greenier E, Lukyanova V, Reede L. Serotonin syndrome: Fentanyl and selective serotonin reuptake inhibitor interaction. AANA J. 2014;82:340–345.
- Rahmani SH, Hassanian-Moghaddam H, Ahmadi S. Serotonin syndrome following single ingestion of high dose methamphetamine. J Clin Toxicol. 2011;1:1–3.
- Smischney NJ, Pollard EM, Nookala AU, Olatoye OO. Serotonin syndrome in the perioperative setting. ACF Case Rep J. 2018;19:833–835.
- Gillman PK. CNS toxicity involving methylene blue: The exemplar for understanding and predicting drug interactions that precipitate serotonin toxicity. J Psychopharmacol. 2010;23:429–436.
- Moss MJ. Serotonin toxicity: Associated agents and clinical characteristics. J Clin Psychopharmacol. 2019;39:628–633.
