The Institute for Safe Medication Practices (ISMP.org) receives thousands of medication error reports through their voluntary practitioner online reporting system. By this mechanism, ISMP compiled a list of important medication errors and hazards during 2020, most of which are of interest to perioperative, intensive care, or pain management practices. They include
Prescribing, Dispensing, and Administering Extended-Release (ER) Opioids to Opioid-Naïve Patients.
Inappropriate prescribing of ER opioids to opioid-naïve patients has resulted in serious harm and death. ISMP, as well as the US Food and Drug Administration (FDA), have warned practitioners about this well-known problem for decades. However, inappropriate opioid prescribing continues to occur, often due to a knowledge deficit about the dangers associated with prescribing ER opioids to opioid-naïve patients and/or not understanding the difference between opioid-naïve and opioid-tolerant. For example, in 2020, ISMP published several new reports related to prescribing fentaNYL patches to opioid-naïve, elderly patients, sometimes to treat acute pain or due to a codeine “allergy” that was a minor drug intolerance.1 FentaNYL patches should only be prescribed to opioid-tolerant patients for the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment. This is so critical to safety that, in 2018, ISMP called for the elimination of prescribing fentaNYL patches to opioid-naïve patients and/or patients with acute pain in our Targeted Medication Safety Best Practices for Hospitals. In 2020, this Best Practice was incorporated into a new Best Practice to verify and document the patient’s opioid status (naïve vs. tolerant) and type of pain (acute vs. chronic) before prescribing and dispensing ER opioids.²
To do this, ISMP first recommends establishing definitions for opioid-naïve and opioid-tolerant patients (for example, following the fentaNYL package insert definitions), and then developing and implementing a standard process for gathering and documenting each patient’s opioid status and type of pain (if pain is present). Order entry systems should default to the lowest initial starting dose and frequency when initiating orders for ER opioids, and interactive alerts should be built to confirm opioid tolerance when prescribing and dispensing ER opioids. Distinguish between true allergies and drug intolerances when collecting allergy information. Eliminate the storage of fentaNYL patches in automated dispensing cabinets (ADCs) or as unit stock in clinical locations where primarily acute pain is treated (e.g., in the emergency department [ED], operating room, post-anesthesia care unit, procedural areas). Our 2020 survey showed low compliance with many of these recommendations.³
Not Using Smart Infusion Pumps with Dose Error-Reduction Systems (DERS) in Perioperative Settings
Our updated (2020) Guidelines for Optimizing Safe Implementation and Use of Smart Infusion Pumps recommend the use of smart pumps with DERS throughout the organization, including in perioperative settings, for all infusions (including hydrating solutions) and bolus/loading doses. However, use of smart pumps with DERS by anesthesia providers in perioperative settings is limited due to barriers and unique challenges. One common barrier to optimal use of smart pumps with DERS in perioperative settings is that there may not be a clear expectation from leadership for anesthesia professionals to use smart pumps with DERS. Many anesthesia professionals do not understand the capabilities of smart pumps, including loading/bolus dose capabilities. Anesthesia professionals may also feel that the soft and hard dose/infusion limits set in the pump are unacceptable, often because they have not been included when building the anesthesia/perioperative drug library. In many organizations, smart pumps are used in the operating room with an “anesthesia mode” setting. However, the organization may fail to understand that, in some pumps, “anesthesia mode” settings reduce all hard stops to soft stops, (soft stops can be overridden, while hard stops cannot), thereby allowing easy overrides of dosing/concentration limits that should never be bypassed.
Leadership should clearly establish that the use of smart pumps with an engaged DERS is expected in perioperative settings for all infusions and loading/bolus doses (except when the hydrating solution rate is greater than the pump allows). Anesthesia professionals involvement with building the smart pump library is paramount. When possible, implement upper and lower hard limits for medication doses, concentrations, infusion rates, and loading/bolus doses, and restrict the use of pumps in “anesthesia mode” if it affects individualization of infusion limits. Anesthesia professionals should use the bolus feature (if available) with hard limits for catastrophic doses, and not allow the delivery of bolus doses by increasing the rate of the infusion. Hands-on education about how to use smart pumps with DERS, including the bolus dose feature, along with competency assessments should be implemented for all anesthesia professionals. Organizations are encouraged to analyze pump data to understand any barriers to the effective use of smart pumps with DERS in the perioperative setting.
Errors with Oxytocin
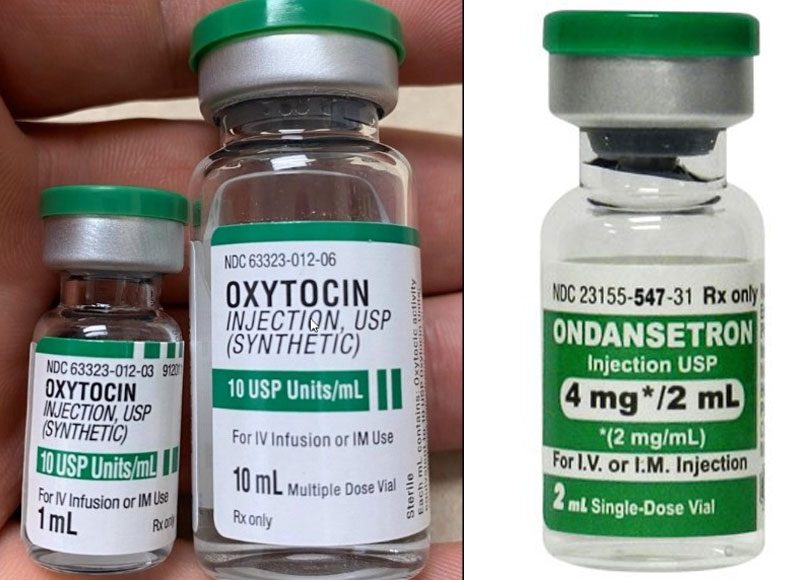
Figure 1: (Left) Depicts oxytocin vials with green caps that look similar to the ondansetron vials.
Figure 2: (Right) Depicts an ondansetron vial with a green cap that looks similar to some oxytocin vials.
In 2020, ISMP conducted an analysis of oxytocin errors, many of which caused hyperstimulation of the uterus, which can result in fetal distress, uterine rupture, or an emergency cesarean section. Sadly, a few maternal, fetal, and neonatal deaths have been reported. More than one-third of the reported errors were associated with look-alike vials and label confusion.4 For example, generic oxytocin and brand PITOCIN vials look similar to ondansetron vials from various manufacturers, which all have green caps (see figures 1 and 2). Several recent 10-fold dosing errors were caused by label confusion with 1, 10, and 30 mL oxytocin vials (Fresenius Kabi, Homburg, Germany). The labels prominently display “10 USP units/mL,” with the total volume in the vial at the bottom of the label, causing staff to think there were only 10 units total in each vial. A few prescribing errors were caused by selection of the wrong drug on order entry screens when searching using only the first few letters of a drug name (e.g., “OXY10” for oxytocin vs. oxyCODONE; “PIT” for Pitocin vs. PITRESSIN [discontinued brand of vasopressin]). Occasionally, verbal orders for “Pitressin” were misheard as Pitocin and dispensed, or vice versa. Administration errors were often related to incomplete or omitted labels on nurse-prepared oxytocin solutions, which often led to infusion bag swaps. Numerous errors were reported in which an oxytocin bag was mixed up with either a hydrating fluid or magnesium infusion.
To help prevent oxytocin errors, hospital systems may require prescribers to use at least five letters of a drug name when searching electronic systems. Avoid nurse-prepared oxytocin infusions and instead have pharmacy dispense oxytocin in ready-to-administer, labeled bags in standardized concentrations. Ensure oxytocin vial (and premixed infusion) labels are clear regarding the amount of drug per total volume. Employ barcode scanning technology when stocking automatic dispensing cabinets and when preparing and administering infusions. Infuse oxytocin solutions through a smart infusion pump with an engaged DERS. Immediately discard discontinued oxytocin infusion bags.⁴
Hazards Associated with Positioning Infusion Pumps Outside COVID-19 Patients’ Rooms
During the COVID-19 pandemic, some hospitals have positioned infusion pumps outside COVID-19 patients’ rooms to conserve personal protective equipment (PPE), reduce staff exposure, and enhance the ability to hear and respond to pump alarms in a timely manner. This has been accomplished, in part, through the use of extension sets. The length and inner diameter of the long extension tubing can impact the volume of fluid needed for priming, flow rates, and the time medications and solutions take to reach a patient. Inadvertent bolus doses of medication remaining in the extension set might be administered to a patient when flushing the long tubing. Occlusion alarms may be delayed at low flow rates or become excessive at high flow rates. The long extension tubing (and electrical cords) may pose a tripping hazard and become tangled and disconnected. Barcode scanning of the patient and drug may be more challenging, and certain components of an independent double check may become difficult or impossible in some situations.
While recognizing that this is not ideal, hospitals must weigh the risk vs. benefit of positioning infusion pumps outside COVID-19 patients’ rooms. If a decision has been made to locate pumps outside of rooms, health care professionals should periodically assess the process. A special report from ECRI can help guide the selection and use of long extension sets for this purpose and includes other factors (e.g., fluid viscosity) that should be considered.⁵ ECRI recommends the following:
- The nurse should conduct periodic infusion pump rounds in the hallway to verify the accuracy of the fluids and medications infusing as well as the pump settings;
- Check that the tubing is not disconnected or a tripping hazard;
- Develop a temporary process that allows some components of barcode scanning and/or independent double checks to occur prior to medication administration. For example, because nurses cannot scan the barcode on the patient’s identification band, some hospitals affix the patient’s name, birthdate, and a barcode to the pump or intravenous (IV) pole located outside the room.
- At the end of the pandemic or when pumps are no longer located in hallways, discontinue temporary identification measures and have staff return to the verification processes in place prior to the pandemic.
Combining or Manipulating Commercially Available Sterile Products Outside the Pharmacy
Our recent 2020 survey on admixture outside the pharmacy showed that this error-prone practice happens often during emergency situations, mostly without formal training, and that there are significant procedural deviations and challenges associated with the practice that contribute to risk.6 Survey respondents told us that IV push medications, IV intermittent infusions, IM injections, and IV continuous infusions were the most frequent sterile injectables prepared outside the pharmacy, primarily by nurses, anesthesia professionals, and physicians. Nearly half of the respondents told us they have not been formally trained for this complex task. The biggest concerns expressed by respondents were lack of space, rushing through the preparation process, labeling issues, mixing by memory instead of following written instructions, interruptions and distractions, and concerns about sterility and accuracy. Nearly one-third of the respondents were aware of associated errors in the past year, particularly preparation errors.⁶
The results of this survey can be used to prompt internal discussions about the need to limit the preparation of admixtures outside the pharmacy as much as possible and how to increase the use of pharmacy- and manufacturer-prepared, ready-to-use products. If your organization did not participate in this survey, you can download it by clicking here, conduct it internally, and review the results to pinpoint your vulnerabilities and establish a plan for improvement. The goal for 2021 should be to significantly reduce the need and frequency of admixture outside the pharmacy.
Wrong Route (Intraspinal Injection) Errors with Tranexamic Acid
ISMP continues to receive reports involving the accidental intraspinal injection of tranexamic acid instead of a local anesthetic intended for epidural or spinal anesthesia. Bupivacaine, ropivacaine, and tranexamic acid are sometimes packaged in vials with the same blue color cap (see figure 3). When the vials are standing upright in storage, practitioners have picked up a vial based on cap color and not noticed it was the wrong vial. Wrong route errors with tranexamic acid are the only error type repeated from our 2019 list of Top 10 Medication Errors and Hazards, and they are the only danger that rose to the level of activating the National Alert Network during 2020. Last month, the FDA announced that it will be revising the tranexamic acid labeling to highlight the IV route of administration and strengthen the warnings to include the risk of wrong route errors. Accidental intraspinal injection of tranexamic acid can result in severe patient harm, with a mortality rate of 50%.⁷
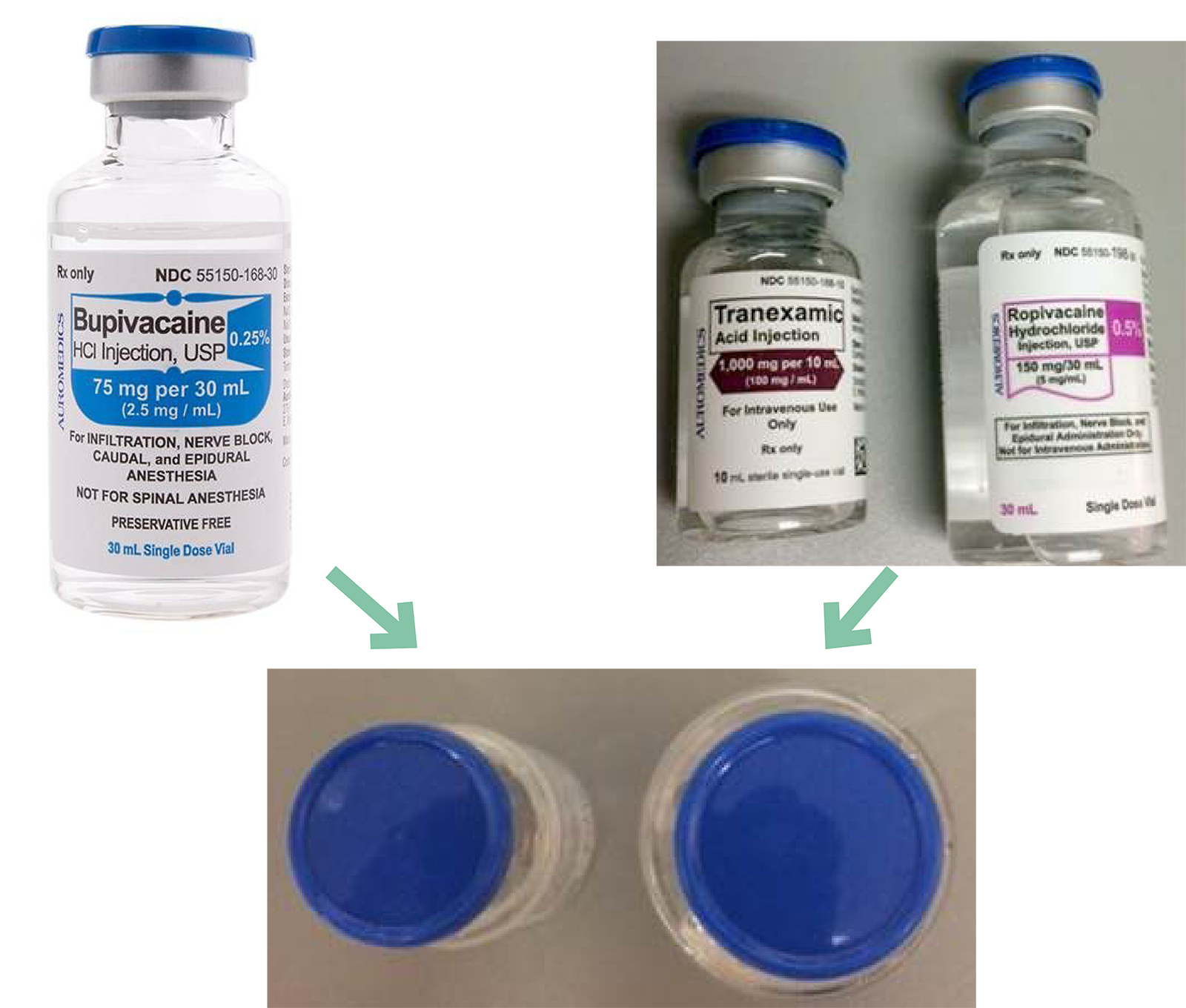
Figure 3: Depicts tranexamic acid, ropivacaine and bupivacaine vials with the same blue color cap.
We urge practitioners to purchase these products from different manufacturers to help differentiate their appearance and/or consider alternate preparations (e.g., premixed bag, pharmacy-prepared syringes or infusions). Providers should avoid upright storage of the vials so the labels are always visible. Pharmacies should store tranexamic acid vials away from other look-alike vials and add an auxiliary label to vials to highlight the IV route of administration. When possible, employ barcode scanning prior to dispensing and administration. Some manufacturers provide a premixed bag of 1 g/100 mL of tranexamic acid, which should be used when appropriate, or have the pharmacy prepare minibags to reduce the risk of mix-ups. Providers should also consider transitioning to NRFit syringes and connectors for local anesthetics to prevent misconnections with drugs intended for IV use.
In summary, ISMP has compiled some of the most common medication errors reported from perioperative care areas in 2020, and they are reported here.
This article was adapted from the ISMP Top Ten List of Medication Errors and Hazards,8 with permission.
Ronald S. Litman, DO, ML, is professor of Anesthesiology and Pediatrics at the Children’s Hospital of Philadelphia and the Perelman School of Medicine at the University of Pennsylvania, and the medical director of the Insitutute for Safe Medication Practices.
The author has no further conflicts of interest.
References
- Institute for Safe Medication Practices. Inappropriate fentaNYL patch prescriptions at discharge for opioid-naïve, elderly patients. ISMP Acute Care Newsletter. July 2, 2020.
- Institute for Safe Medication Practices. Targeted medication safety best practices for hospitals. ISMP Acute Care Newsletter. February 21, 2020.
- Institute for Safe Medication Practices. survey shows room for improvement with two new ISMP targeted medication safety best practices. ISMP Acute Care Newsletter. July 30, 2020.
- Institute for Safe Medication Practices. Errors associated with oxytocin use: a multi-organization analysis by ISMP and ISMP Canada. ISMP Acute Care Newsletter. February 13, 2020.
- ECRI. Large-volume infusion pumps—considerations when used with long extension sets outside patient rooms to help reduce staff PPE use. ECRI Exclusive Hazard Report. April 1, 2020.
- Institute for Safe Medication Practices. ISMP survey provides insights into preparation and admixture practices OUTSIDE the pharmacy. ISMP Nurse AdviseERR Newsletter. November 4, 2020.
- Palanisamy A, Kinsella SM. Spinal tranexamic acid—a new killer in town. Anaesthesia. 2019;74:831–833.
- Institute for Safe Medication Practices. ISMP publishes top 10 list of medication errors and hazards covered in newsletter. ISMP medication safety alert! Acute Care Newsletter. January 16, 2020.
