INTRODUCTION
Nonsurgical cosmetic enhancements such as neurotoxins, eyelash extensions, gel manicures, or permanent jewelry, have grown exponentially in popularity over the last several years. Whether individuals seek to alter their appearance to achieve a more youthful image, enhance self-esteem, or experience the latest social media trend, these procedures have become increasingly safer, more accessible, socially acceptable, and affordable.
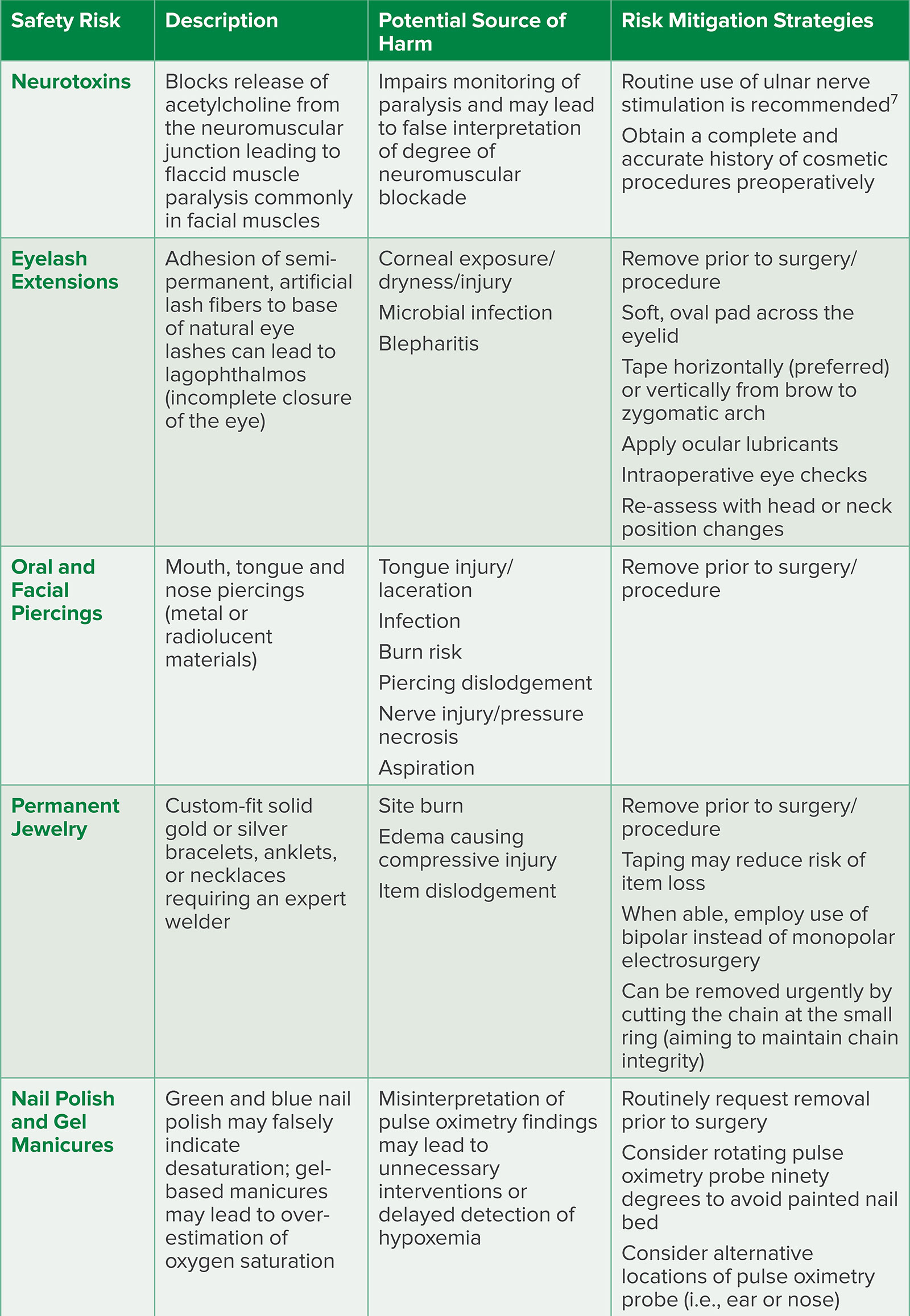
Regrettably, many of these cosmetic enhancements can significantly impact anesthetic technique and delivery. This article highlights popular cosmetic enhancements that may have under-recognized anesthetic implications whilst providing suggestions to improve patient safety by (1) promoting conversations with patients about the associated risks and (2) outlining steps that can minimize patient harm (Table 1).
Table 1. Potential Cosmetic Safety Risks and Authors’ Proposed Risk Mitigation Strategies
NEUROTOXINS AND PERIPHERAL NERVE STIMULATOR MONITORING
Overall trends in the use of minimally invasive cosmetic procedures have significantly gained in popularity since the pre-pandemic era with the return to mask-free environments. According to the American Society of Plastic Surgeons, neuromodulator injections are the most popular minimally invasive procedure with over 8.7 million procedures performed in 2022—an increase of over 70% from 2019.1 Botulinum toxin, a neurotoxin produced by the bacterium Clostridium botulinum, produces flaccid muscle paralysis by blocking the release of acetylcholine at the neuromuscular junction; it is used for the treatment of hyperfunctional facial lines resulting from repeated contractions most commonly in facial muscles such as orbicularis oculi, procerus, corrugator supercilii, and frontalis. Commonly known by their brand names (BOTOX Cosmetic®/AbbVie Inc, North Chicago, IL; Dysport®/Galderma Laboratories, L.P. Dallas, TX; Xeomin®/Bocouture, Merz North America, Inc., Raleigh, NC; Jeuveau®/Evolus, Inc., Newport Beach, CA; and Daxxify®/Revance Therapeutics, Inc., Nashville, TN), these neurotoxins have been of increased interest, driven by the desire for personalized beauty, economic feasibility, and accessibility.
There are few case reports documenting monitoring-related complications secondary to neurotoxin use. In 2006, a case report was published describing a 35-year-old woman presenting for elective laparoscopic surgery given rocuronium with no train-of-four, double-burst, or tetanic stimulation patterns noted on her forehead one hour after induction though forceful and fade-free muscle contractions were provoked at the ulnar nerve.2 A year later, a case report of a 72-year-old man scheduled for an urgent exploratory laparotomy described that upon surgical closure of the fascia, the surgeon stated the patient’s muscles were not relaxed despite 0/4 twitches noted using a peripheral nerve stimulator at the orbicularis oculi muscles bilaterally.3 Placement of the nerve stimulator over the ulnar nerve noted recovery of the train-of-four. In both case reports, postoperative patient interviews confirmed a history of botulinum toxin injections to the upper facial muscles in the weeks prior to surgery.
Similar case reports have continued to be published in isolation. One report described an urgent intra-abdominal procedure with surgical concerns voiced about degree of paralysis, and the patient was noted to be breathing while on the ventilator.4 Another described a 46-year-old woman presenting for Cesarean delivery under general anesthesia for HELLP syndrome who was given succinylcholine to facilitate intubation; absence of train-of-four pattern was noted 25 minutes later at the orbicularis oculi, but full recovery then confirmed with ulnar nerve stimulation, highlighting the risk of encountering cosmetic neurotoxin use in the aging pregnant population.5 Another report detailed a 61-year-old woman whose postoperative course was complicated by multi-organ system failure requiring mechanical ventilatory support.6 Adequate neuromuscular blockade with cisatracurium was assumed via facial nerve stimulation; however, patient-ventilator dyssynchrony prompted moving the peripheral nerve stimulator to the ulnar nerve, whereby muscle twitches indicated inadequate paralysis.
Notably, each report proffers sensible advice given the increasingly common use of cosmetic neurotoxins. First, all authors suggested the routine use of the ulnar nerve stimulation for neuromuscular monitoring—a recommendation now strongly supported in the 2023 American Society of Anesthesiologist Practice Guidelines for Monitoring and Antagonism of Neuromuscular Blockade.7 Second, most authors recommended obtaining a complete and accurate history including the use of cosmetic procedures prior to the administration of paralytic agents. As the prevalence of cosmetic procedures continues to rise, all patients, regardless of age, gender, or youthful appearance, should be queried preoperatively.
EYELASH EXTENSIONS AND CORNEAL INJURY
Safety Concerns for Cosmetic Enhancements
Eyelash extensions, which involve the adhesion of semipermanent, artificial lash fibers to the base of each individual natural lash via glue with the hopes of obtaining fuller, longer lashes, are also increasing in popularity. Adverse effects following eyelash extensions include dry eyes, burning sensations, lid swelling, and pain following their application. Of particular interest to the anesthesia professional, these extensions can cause lagophthalmos, or incomplete closure of the eye during sleep, which can lead to increased corneal exposure and dryness, collection of bacteria under the lash bed causing microbial infection, and constraints to physical hygiene and cleansing of the lid which can lead to infection and blepharitis.8 Corneal injury is cited to be the most common ophthalmic complication during the perioperative period, specifically for patients undergoing general anesthesia.9 Corneal abrasions and exposure keratopathies are secondary to inadequate closure of the eyelids during anesthesia, and the lagophthalmos caused by eyelash extensions can exacerbate these complications. Furthermore, misdirection of lashes falling into the eye can also increase the risk of corneal injury.
Ideally, eyelashes should be removed prior to surgery. When eyelashes cannot be removed, an increased risk of corneal abrasions, infection, and inadvertent removal of lashes should be disclosed. Intraoperatively, a soft, oval eye pad can be placed across the eyelid with tape placed in a horizontal (preferred) or vertical manner from brow to zygomatic arch, which may avoid direct adhesive contact to the eyelashes, causing unintentional removal. Ocular lubricants can also be used to help prevent dehydration. Vigilance during intraoperative eye checks is paramount, particularly if head or neck positioning changes occur.
ORAL AND FACIAL PIERCINGS AND AIRWAY COMPROMISE
Preoperative Assessment of Cosmetic Enhancements May Improve Patient Safety
There are numerous potential and actual hazards of mouth, tongue, and nose piercings including unintentional dislodgement, airway obstruction, or reactivity including a published case report of a missing nose stud that was eventually found near the patient’s head but had the potential to have been displaced into the airway.10 More concerning, another case report described a case of laryngospasm caused by oropharyngeal bleeding secondary to a tear adjacent to a tongue stud.11
A thorough preoperative assessment of the presence and type of foreign bodies should include piercings. Theoretical and documented risks of these piercings include tongue injury and laceration, infection, bleeding, dental injury, piercing dislodgement, nerve injury, aspiration, pressure necrosis injury, and death. Recognize that while patients may agree to remove metal studs after these risks are detailed, there has been a trend to replace a metal stud with a radiolucent bar to maintain the hole patency—potentially posing a challenge to see or locate should it become displaced.12 Additionally, while the notion of utilizing neuraxial or regional techniques (such as in the case of laboring parturients or orthopedic procedures) to avoid general anesthesia may seem to pose less of a risk, the need to emergently convert to a general anesthetic is always possible and may potentiate the risks associated with in situ jewelry.13-15
PERMANENT JEWELRY AND BURN RISKS
Electrocautery use in the operating room requires a return plate for the electrosurgical unit, serving as a low-resistance pathway for the energy to return safely to the apparatus. In the rare case that the pad is not adhered appropriately, dislodged, or has dried electrolyte gel, patient jewelry or piercings could act as a return pathway and cause a burn.16 While many perioperative protocols require the removal of metal jewelry prior to surgeries using electrocautery, little is known about the risk of burns to patients, though the risk is thought to be relatively small.17,18 The Association of Perioperative Registered Nurses recommends removing metal piercings if they are between the active electrode (i.e., Bovie tip) and the grounding pad.19 Removal of jewelry is a reliable method to eliminate the risk, but may not always be possible. Taping jewelry, believed to insulate metal jewelry from contacting other electroconductive material, has not been proven to affect the risk of site burns though may reduce the risk of losing the personal item.16
Permanent jewelry is a recent trend gaining popularity due in part to social media platforms. Though a relatively niche service, permanent jewelry entails a custom-fit solid gold or silver bracelet, anklet, or necklace and requires an expert welder to “zap” (refers to the flash you see when a jewelry piece is welded) the two ends together. These delicate chains can be accessorized with mini charms such as natural gemstones, diamonds, or gold drops and often have sentimental value to the wearer.
Permanent jewelry can be removed by carefully cutting the chain with scissors at the small ring that connects the two ends of the chain to maintain the integrity of the chain, such that it can be re-welded should the user so desire. Ideally, permanent jewelry should be removed prior to scheduled surgery and included in preoperative instructions. If jewelry cannot be removed, potential adverse events (including burn, edema causing compressive injury, or item dislodgement) should be disclosed to the patient and documented. When possible, alternative technologies (i.e., bipolar instead of monopolar electrosurgery) should be employed, and care should be taken to prevent contact between the patient and metal objects. Postoperatively, all jewelry sites should be assessed for evidence of injury.
NAIL POLISH, GEL MANICURES, AND PULSE OXIMETRY
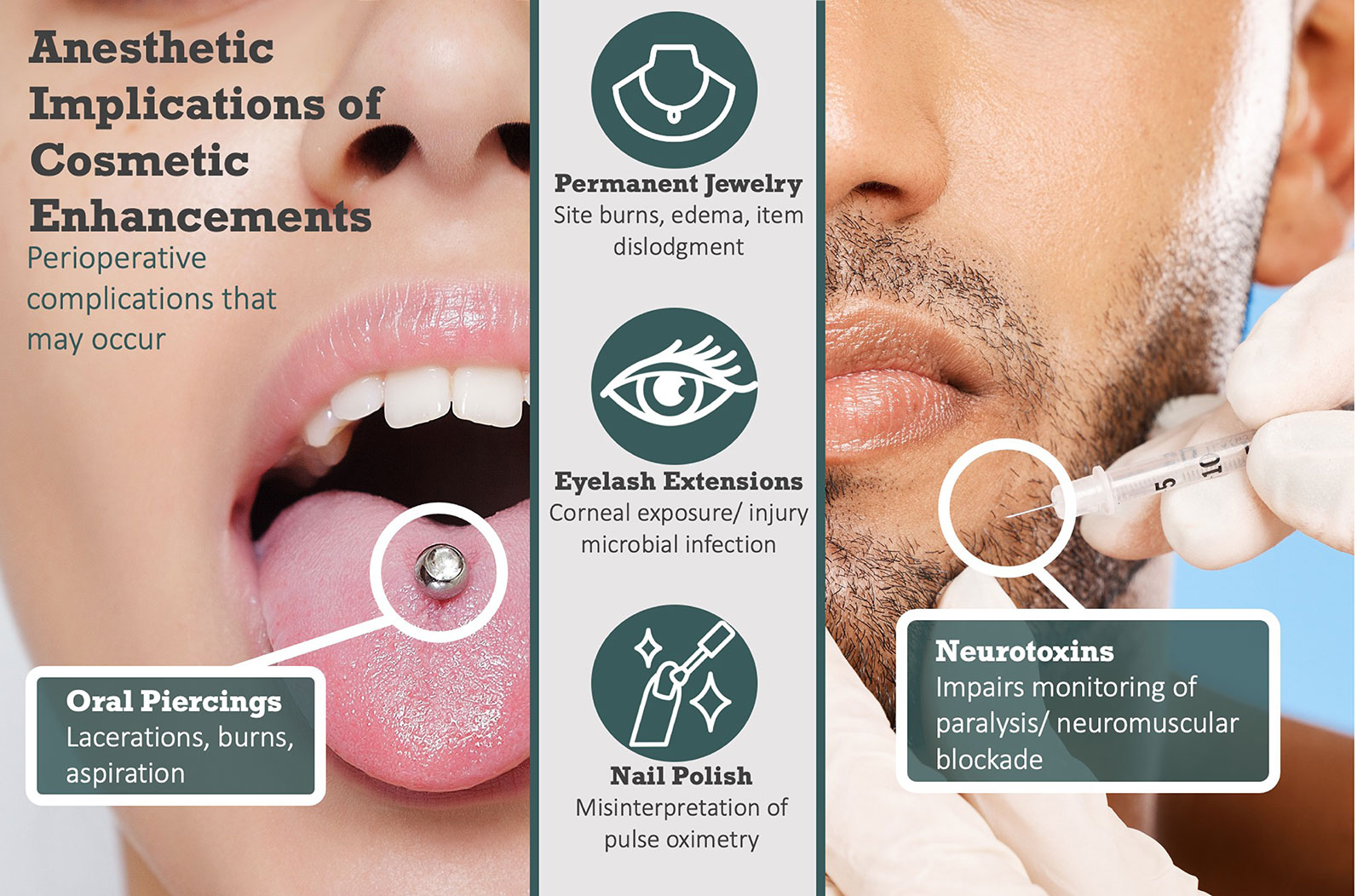
Pulse oximetry helps to measure functional oxygen saturation in arterial blood by examining the difference in absorbance at two wavelengths, 660 and 940 nm. Any factors that increase the difference in absorbance between the two wavelengths will cause the pulse oximeter to falsely indicate desaturation. Spectrophotometric evidence yields that both green and blue nail polish increase absorbance at 660 nm as compared to 940 nm and can “trick” the sensor into indicating desaturation, which could lead to unnecessary interventions in the operating room.20 More recently, gel-based manicures have gained favor by extending the life of a manicure, utilizing polymerized acrylate monomers that decrease chipping and scratching. These types of manicures can result in a statistically significant increase from baseline SpO2 readings, most notably with orange and light blue colors, suggesting that nail polish could result in an anesthesia professional’s overestimation of the actual oxygen saturation subsequently delaying or even failing to detect hypoxemia altogether.21 As such, it may be prudent to routinely request polish removal prior to surgery. In the event patients are unable to comply with this request, alternative pulse oximetry probe locations or even simply turning the probe 90 degrees so as to avoid the painted nail bed may be warranted (Figure 1).
Figure 1. Alternative placement of a pulse oximetry probe on the finger with 90-degree rotation to avoid green nail polish interference.
FACILITATING DISCLOSURE
Cosmetic enhancements can affect the planning and execution of anesthetic delivery both inside and outside of the operating room. The risks these procedures pose to patients should be formally discussed in the informed consent process.
Anesthesia professionals may not be comfortable broaching these topics or feel inadequately suited to ask questions regarding cosmetic enhancements in the preoperative setting, but there are resources to help clinicians discuss sensitive topics with patients. The goal is to improve communication by decreasing patient and physician anxiety, thereby increasing the accuracy and specificity of patient self-reporting.22 Three essential factors affect the reliability and validity of self-report:
The clinician’s own anxiety may result in avoidance of inquiry about these topics. Recognizing the anesthetic implications of these cosmetic procedures is vital to understanding and identifying any potential safety concerns.
The patient’s anxiety about disclosing, particularly in the perioperative setting without established patient-physician relationships or due to family member presence, may prohibit disclosure. While patients have become more transparent and comfortable with disclosing personal information, it may be beneficial to include the potential liabilities associated with these cosmetic enhancements on informed consent, which the patient can read privately. The perioperative setting can be particularly challenging to navigate these discussions with time-pressure demands, elevated noise levels, and little-to-no privacy.
The “how” of asking questions, including reconsidering the wording, order, and form of questions, can affect the accuracy of obtained information. Where many health care professionals have been trained to ask open-ended questions in medical history-taking, it is ideal to ask more closed-ended questions, such as “Have you had any recent cosmetic procedures?” or “Do you have any nail polish, jewelry, or metal studs?” Be sure to ask for specific facts about neurotoxins, the location of piercings, etc.
CONCLUSION
Anesthesia professionals should be knowledgeable of the implications of non-surgical cosmetic procedures. Performing a thorough yet sensitive preoperative assessment, offering informed disclosure of potential adverse events, and promoting vigilance throughout the perioperative environment mitigates the risks from cosmetic procedures and thereby reinforces the anesthesia professional’s role as the advocate for patient safety.
Melissa Byrne, DO, MPH, FASA, is a clinical assistant professor of anesthesiology at Michigan Medicine, Ann Arbor, Michigan, USA.
Danielle Saab, MD, is a clinical assistant professor of anesthesiology at Michigan Medicine, Ann Arbor, Michigan, USA.
The authors have no conflicts of interest.
REFERENCES
- Plastic surgery statistics. American Society of Plastic Surgeons. https://www.plasticsurgery.org/news/plastic-surgery-statistics. Accessed October 30, 2023.
- Ward SJ, Harrop-Griffiths W. Botox injections and monitoring neuromuscular blockade. Anaesthesia. 2006;61:726. PMID: 16792640.
- Miller L, Neustein S. Neuromuscular blockade monitoring complicated by the unknown preoperative cosmetic use of botulinum toxin. Anesthesiology. 2006;105:862. doi: 10.1097/00000542-200610000-00049
- Cross C. Botox injections and monitoring neuromuscular blockade—a reminder. Anaesthesia. 2016;71:732. PMID: 27159003.
- Kuczkowski, K. Botox and obstetric anesthesia: is there cause for concern? 11AP1-1. Eur J Anaesth. 2007;24:139. https://journals.lww.com/ejanaesthesiology/citation/2007/06001/botox_and_obstetric_anesthesia__is_there_cause_for.518.aspx. Accessed December 15, 2023.
- Le NK, Liauw D, Siddiqui SZ, Donohue KM. Assessment of neuromuscular function in patients with prior cosmetic procedures: a case report. Eplasty. 2019;19:e20. eCollection 2019. PMID: 31885763.
- Thilen SR, Weigel WA, Todd MM, et al. 2023 American Society of Anesthesiologists practice guidelines for monitoring and antagonism of neuromuscular blockade: a report by the American Society of Anesthesiologists Task Force on neuromuscular blockade. Anesthesiology. 2023;138:13–41. PMID: 36520073.
- 8. Masud M, Moshirfar M, Shah TJ, et al. Eyelid cosmetic enhancements and their associated ocular adverse effects. Med Hypothesis Discov Innov Ophthalmol. 2019;8:96–103. PMID: 31263720.
- A case report from the anesthesia incident reporting system. ASA Newsletter. 2014;78:44–45. https://pubs.asahq.org/monitor/article/80/7/44/3270/Case-Report-From-the-Anesthesia-Incident-Reporting. Accessed October 15, 2023.
- Girgis Y. Hypoxia caused by body piercing. Anaesthesia. 2000;55:413. PMID: 10781175.
- Wise H. Hypoxia caused by body piercing. Anaesthesia. 1999;54:1129. PMID: 10540120.
- Pandit JJ. Potential hazards of radiolucent body art in the tongue. Anesth Analg. 2000;91:1564–1565. PMID: 11094027.
- Mandabach MG, McCann DA, Thompson GE. Tongue rings: just say no. Anesthesiology. 1998;89:1279–1280 PMID: 9822025.
- Rapid response: anaesthetic concerns in patients with pierced tongues. BMJ. 1999;319:1627. doi: 10.1136/bmj.319.7225.1627.
- Kuczkowski KM, Benumof JL. Tongue piercing and obstetric anesthesia: is there cause for concern? J Clin Anesth. 2002;14:447–448. PMID: 12393114.
- Body piercing and electrocautery risks. Anesthesia Patient Safety Foundation. https://www.apsf.org/article/body-piercing-and-electrocautery-risks/. Accessed October 30, 2023.
- Blumenstein N, Wickemeyer J, Rubenfeld A. Bringing to light the risk of burns from retained metal jewelry piercings during electrosurgery—torching the myth. JAMA Surg. 2022;157:455–456. PMID: 35234844.
- Deml MC, Goost H, Schyma C, et al. Thermic effect on metal body piercing by electrosurgery: an ex vivo study on pig skin and bovine liver. Technol Health Care. 2018;26:239–247. PMID: 29286941.
- Guideline quick view: electrosurgical safety. AORN J. 2020;112:430–434. doi: 10.1002/aorn.13421
- Coté CJ, Goldstein EA, Fuchsman WH, Hoaglin DC. The effect of nail polish on pulse oximetry. Anesth Analg. 1988;67:683–686. PMID: 3382042.
- Yek JLJ, Abdullah HR, Goh JPS, Chan YW. The effects of gel-based manicure on pulse oximetry. Singapore Med J. 2019;60:432–435. PMID: 30854571.
- McBride R. Talking to patients about sensitive topics: communication and screening techniques for increasing the reliability of patient self-report. MedEdPORTAL. 2012;8:9089. doi: 10.15766/mep_2374-8265.9089
