INTRODUCTION
Quantitative neuromuscular blockade monitoring (QNMT) is strongly recommended by the ASA1 and APSF2 and can be accomplished with several commercially available devices. The basic principle is that a low voltage stimulus to the ulnar nerve, delivered by paired electrodes, will elicit a motor response in the adductor pollicis to move the thumb. The strength of the response is influenced by the degree of neuromuscular blockade and can be quantified. One QNMT method utilizes an accelerometer attached to the thumb which senses acceleration as a surrogate for the strength of the response. Under normal circumstances, no voltage is being directly delivered to the thumb, but the accelerometer positioned at the thumb requires an electrical supply.
CASE REPORT
Electrical Injury With Use of a Neuromuscular Monitor
A 43-year-old male underwent a 2-hour uncomplicated revision colostomy under endotracheal general anesthesia with neuromuscular monitoring by QNMT (Philips IntelliVue NMT, Andover, MA).3 On postoperative day (POD) 2, the anesthesia service was consulted to evaluate a blister on the patient’s thumb, with concern that it might be related to a monitoring device. The patient reported that he noticed the blister in the PACU, but did not report it until POD 2. On exam he had a 1-cm blister on his ventral thumb, as well as a region of skin breakdown over his ipsilateral ventral ulnar forearm (Figure 1A). After identifying the operating room where the procedure had taken place, the QNMT monitor was inspected and found to have exposed wires from a breakdown in the insulation in a place that matched the position of the blister when the device was applied (Figure 1B). The patient was informed of the complication, a hand service consultation was placed, and the device was taken out of service (along with 3 other similarly damaged devices that were subsequently identified). The injury was minor and resolved with topical silver sulfadiazine (Silvadene®) ointment applications twice daily. The patient was appreciative that the anesthesia team had taken his complaints seriously and was relieved to have an answer to his complaint.
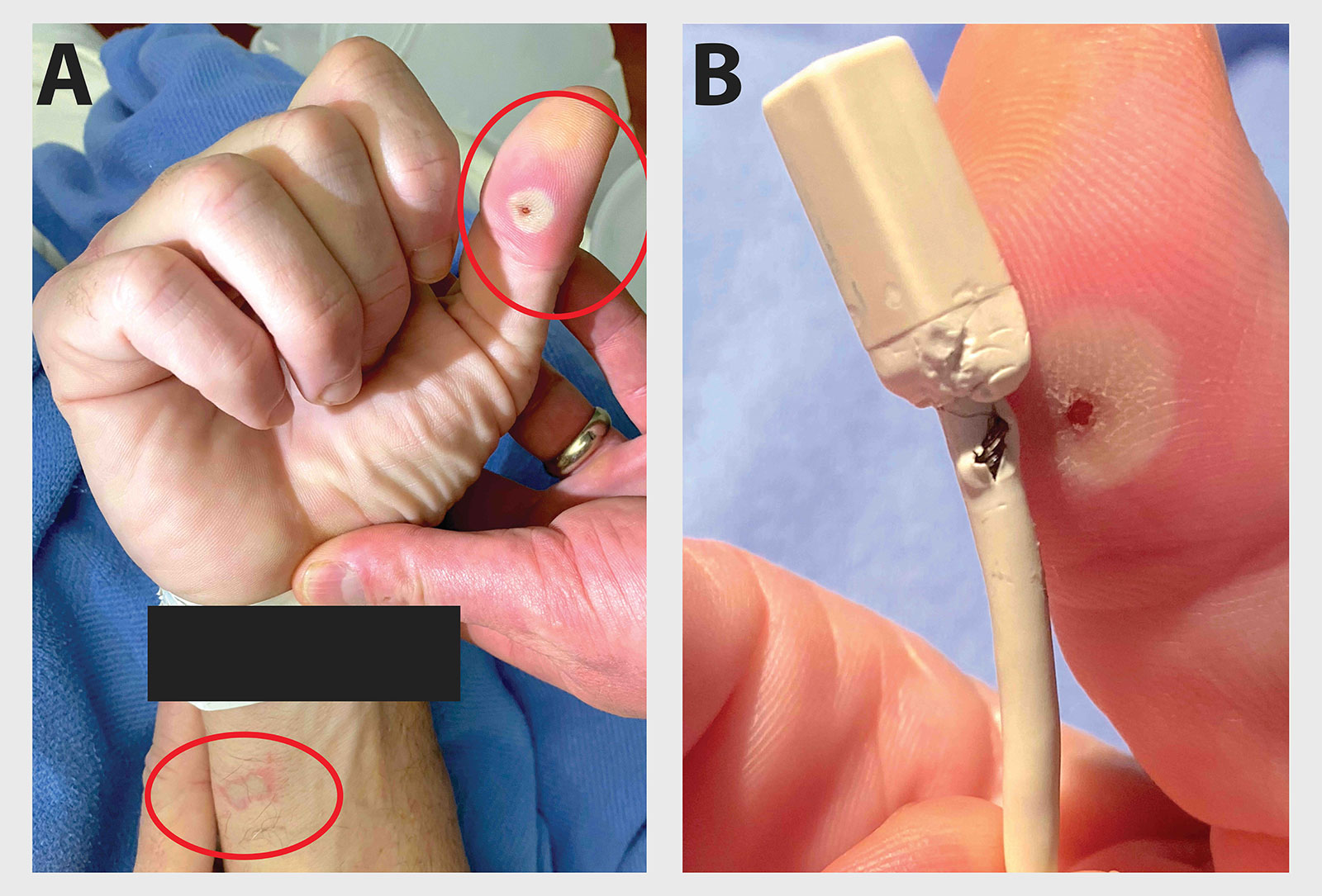
Figure 1: A. Injury to patient’s thumb and forearm after two hours of surgery with NMT monitoring using a damaged cable. B. Image of the damaged device in the proper orientation with exposed wire at the site of patient’s injury.
DISCUSSION
Descriptions of injury from monitoring devices4 or specifically nerve stimulators are numerous.5-7 There has also been a safety bulletin for this device.8 However, with correct usage and uncompromised device integrity, the chance of shock or burn should be very low. The manufacturer of the specific device in this incident offers an attachment which correctly positions the device without direct skin contact which could be considered a convenience and additional safety feature if used. In this case, the damaged cable was not recognized by providers, and because of the way the device can be placed in several orientations, it was only by chance that this complication did not occur with use in other patients (the accelerometer is cubical and can be attached with any of four sides to the patient’s thumb and in this case, the wire contacted the skin directly.) We believe the skin contact with the wire where the insulation had broken down allowed electrical current to flow from that site to the ground electrode at the site of ulnar nerve stimulation. The burn resulted from high energy dissipation in the form of heat as the current passed through the skin.9,10 The anesthesia record did not indicate the frequency of stimulation, but was likely between 1-5 minutes as is typical in our practice.
In response to this event, we made a number of changes at our institution. First, we removed all cables in use with any signs of insulation damage and returned them to the manufacturer for close inspection, including the specific cable that was used in this case report. We opened a dialogue with the manufacturer to discuss the specifics of the case and the resolution. The case was presented at our Morbidity and Mortality Conference, which included an education session about proper use for all anesthesia professionals stressing the importance of inspection of every device attached to patients prior to use. We also educated our anesthesia technicians who assist with room-turnover and processing of equipment. They now inspect the cables while cleaning according to manufacturer instructions and will remove equipment with any signs of damage. Finally, we have acquired the manufacturer specific hand-adapter for our QNMT device and are waiting for final approval on its use from our institution.
This case is an important reminder to inspect all devices that are attached to patients, especially those that are automated and hidden from plain view (i.e., tucked arms, drapes, etc.). While there is no guideline for interval of device evaluations, we suggest all devices be inspected for intact insulation at the time of application, prior to placement.
Gregory A. Chinn, MD, PhD, is an assistant professor of anesthesia at UCSF-Zuckerberg San Francisco General Hospital, San Francisco, CA, USA
Stefan G. Simon, MD, is a professor of anesthesia at UCSF-Zuckerberg San Francisco General Hospital, San Francisco, CA.
Andrew T. Gray, MD, is a professor of anesthesia at UCSF-Zuckerberg San Francisco General Hospital, San Francisco, CA.
Julin F. Tang, MD, is a professor of anesthesia at UCSF-Zuckerberg San Francisco General Hospital, San Francisco, CA.
John C. Markley, MD, is an associate professor of anesthesia at UCSF-Zuckerberg San Francisco General Hospital, San Francisco, CA.
Gregory Chinn, MD, PhD, Stefan Simon, MD, Julin Tang, MD, and John Markley, MD, have no conflicts of interest. Andrew Gray, MD, received equipment support from Rivanna Medical (Charlottesville, VA).
REFERENCES
- Thilen SR, Weigel WA, Todd MM, et al. 2023 American Society of Anesthesiologists practice guidelines for monitoring and antagonism of neuromuscular blockade: a report by the American Society of Anesthesiologists Task Force on Neuromuscular Blockade. Anesthesiology. 2023;138:13–41. PMID: 36520073.
- Caruso L, Lampotang S, Gravenstein N. Patient safety and quantitative neuromuscular transmission monitoring in 2022. APSF Newsletter. 2022;37:66. https://www.apsf.org/article/patient-safety-and-quantitative-neuromuscular-transmission-monitoring-in-2022/ Accessed November 30, 2023.
- Dubois V, Fostier G, Dutrieux M, et al. Philips Intellivue NMT module: precision and performance improvements to meet the clinical requirements of neuromuscular block management. J Clin Monit Comput. 2020;34:111–116. PMID: 30806937.
- Bruner John M R. Common abuses and failures of electrical equipment. Anesth Analg. 1972;51: 810–826. https://journals.lww.com/anesthesia-analgesia/citation/1972/09000/common_abuses_and_failures_of_electrical_equipment.39.aspx.
- Cooper JB, DeCesare R, D’Ambra MN. An engineering critical incident: direct current burn from a neuromuscular stimulator. Anesthesiology. 1990;73:168–172. PMID: 2360724.
- Gray AT. Excessive voltage output? Anesth Analg. 2001;93:515–516. doi: 10.1213/00000539-200108000-00055
- Hadzic A, Vloka J. Peripheral nerve stimulators for regional anesthesia can generate excessive voltage output with poor ground connection. Anesth Analg. 2000;91:1306. doi: 10.1213/00000539-200011000-00049
- Health and Human Services. URGENT – Medical Device Recall Philips IntelliVue Neuromuscular Transmission Patient Cable 989803174581. https://www.hsa.gov.sg/docs/default-source/announcements/field-safety-notices/hsa-6004101-026-17-09_45-fsn_redacted.pdf. Accessed December 15, 2023.
- Kouwenhoven WB. Electrical accidents. T Am Inst Elec Eng. 1937;56:1077–1079. doi: 10.1109/T-AIEE.1937.5057695
- Arnoldo BD, Purdue GF. The diagnosis and management of electrical injuries. Hand Clin. 2009;25:469–479. PMID: 19801121
Philips Response to APSF Newsletter Query—Re: NMT Cable Issue
Philips has received the report of the patient event related to the PhilipsIntelliVue Neuromuscular Transmission (NMT) Patient Cables 989803174581. At this time, we continue to review this report in accordance with the Philips Quality Management System and regulatory compliance requirements.
Regarding the incident report, we feel that it may benefit from inclusion of information from primary source documents such as the instructions for use (IFU) of the IntelliVue NMT Cable, which aligns with the recommendations the authors provide in the Discussion section of the manuscript.
For example, the device IFU indicates in a number of places the potential for an electrical shock hazard and potential for burns in case of use of a damaged cable. The IFU also stipulates that a visual inspection should be performed before every use—and to refrain from using a cable if it shows any signs of damage or if it has exceeded its use-by date (Figure 2).
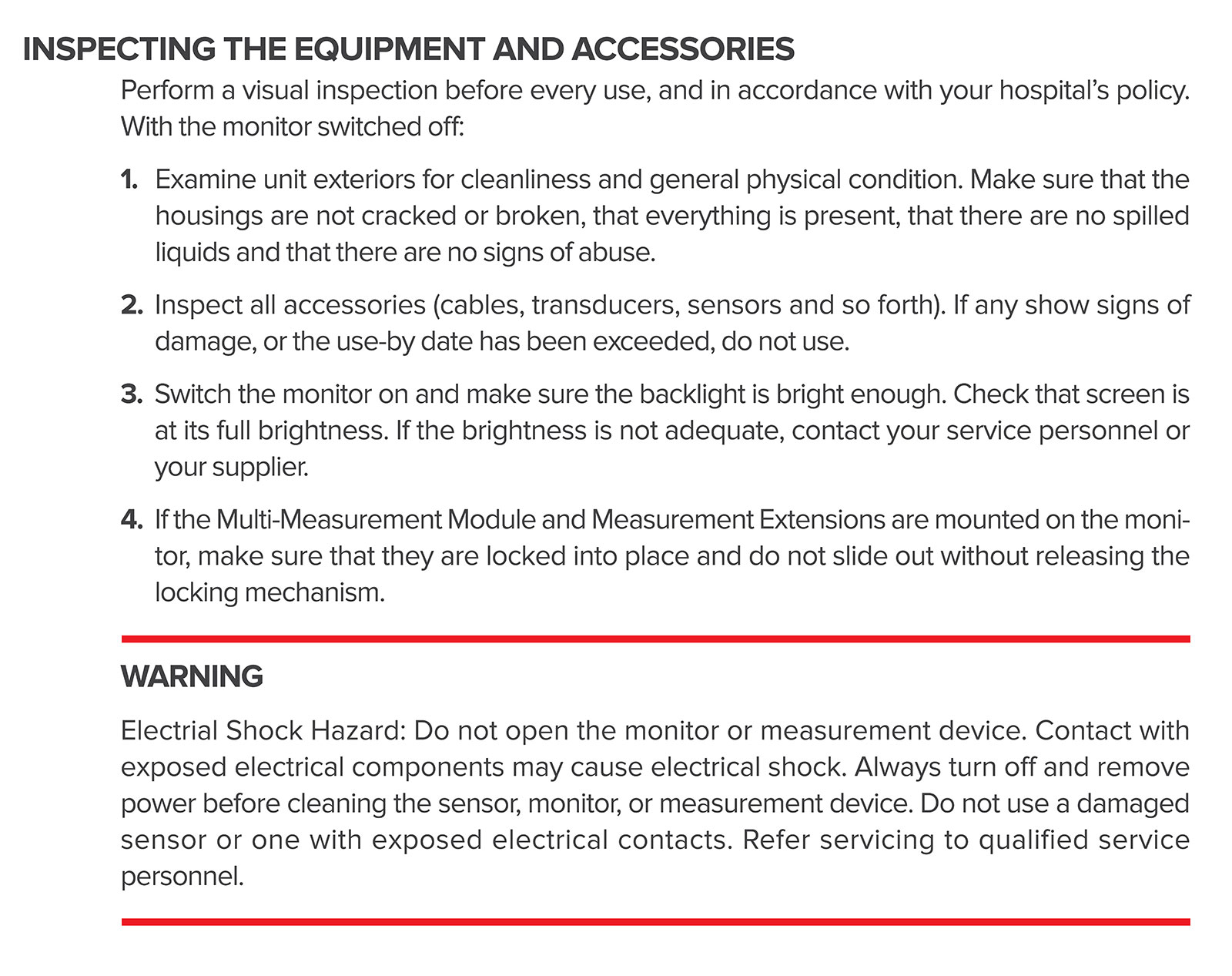
Figure 2: Device Instructions for Use. Permission to reuse Device Instructions for Use information from Phillips.
Furthermore, in 2017, Philips issued a voluntary field safety notice for NMT Cables manufactured between 2012 and 2017, regarding the potential for electrical shock hazard, and also enhanced the electrical insulation for the component. The following information was also added to the IFU at that time (Figure 3):
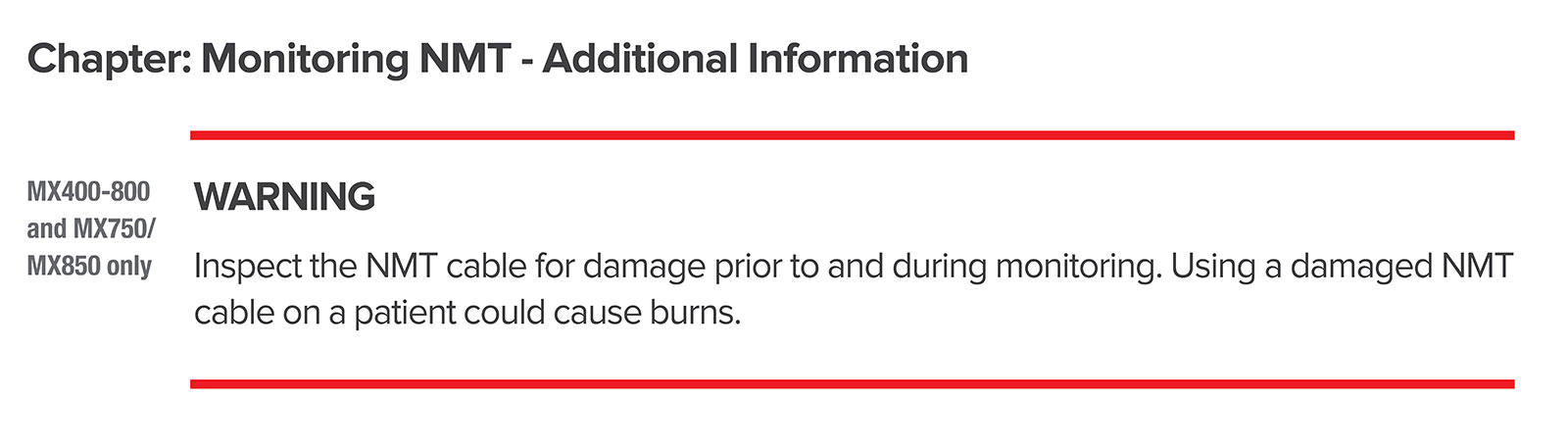
Figure 3: Device Instructions for Use on using damaged NMT cables. Permission to reuse Device Instructions for Use information from Phillips.
Additionally, the “Care and Cleaning” chapter of the IFU contains a general point that “After cleaning and disinfection, check the equipment carefully. Do not use if you see signs of deterioration or damage.”
Also worthy of note is that Philips recommends the use of the Philips NMT Hand Adapter (989803199211) to improve the measurement and to facilitate the application of the NMT sensor (Figure 4). The NMT hand adapter provides a secure fixation point for the NMT patient cable acceleration sensor without the need for applying it with adhesive tape.
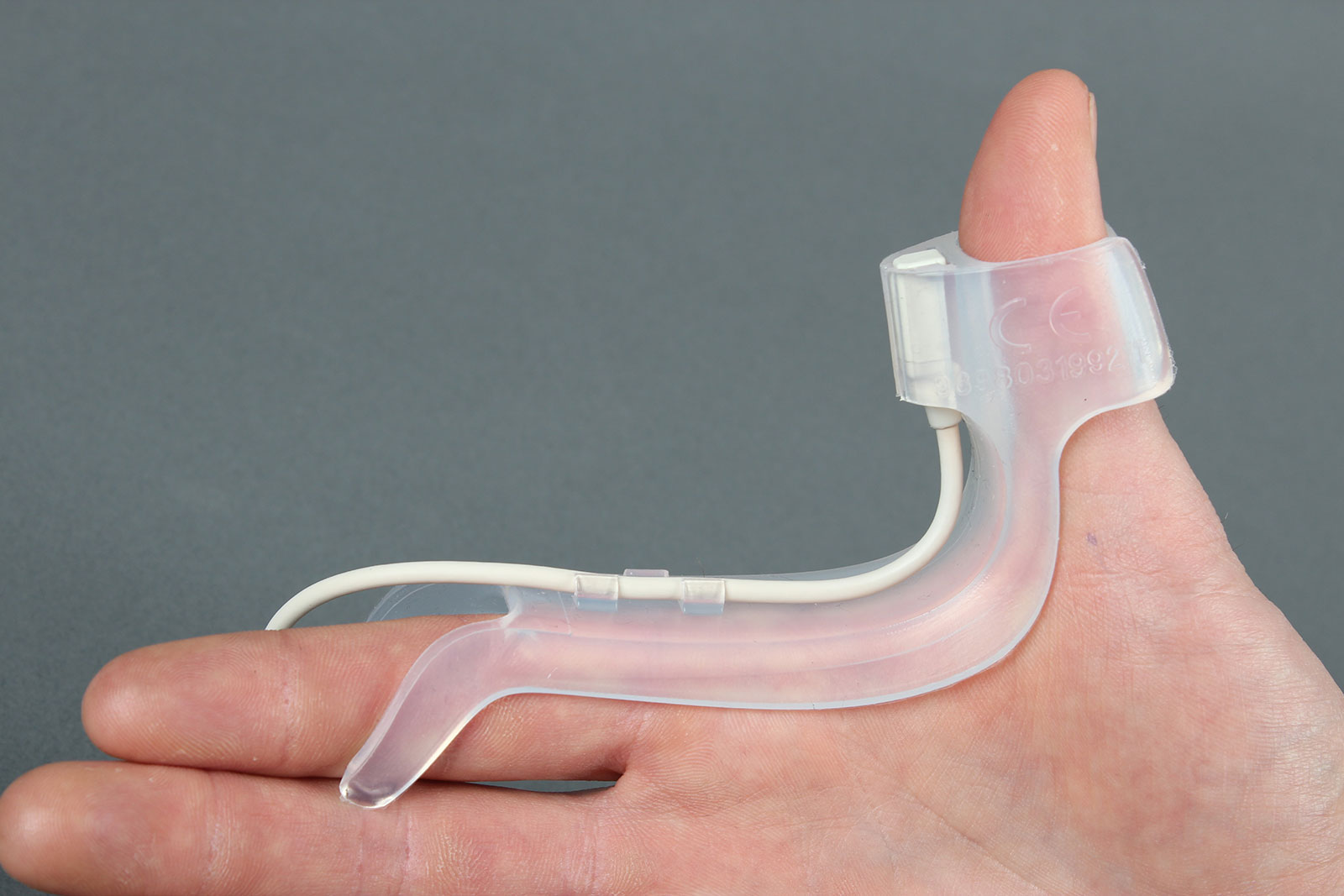
Figure 4: Philips NMT Hand Adapter (989803199211).
Please let us know if we may provide further information or support, and we will be sure to follow up.
Lorenzo Quinzio, MD
Product Marketing Lead,
Measurement Solutions
Hospital Patient Monitoring
Royal Philips
The author has no conflicts of interest other than being an employee at Philips.
The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or group responses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intention of APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
