BACKGROUND
The principles of Situation Awareness (SA) originated in aviation psychology, a field that bears similarities to medicine in its daily challenges of dealing with complex, dynamic, and often unforeseen situations. David Gaba, MD, an anesthesiologist at Stanford University and former member of the Board of Directors of the APSF recognized this connection nearly 30 years ago and introduced the concept of SA to the field of anesthesiology.1 Two decades later, SA experienced a resurgence through the combined efforts of its originator, Mica Endsley, PhD, an engineer,2 and an anesthesiologist, Christian Schulz, MD.3 With this contribution, we aim to bring the concept into focus once again and highlight its critical importance for patient safety, as errors in SA often underlie patient harm.4,5
SITUATION AWARENESS
SA is a three-tiered concept that involves a cyclical sequence of perceiving individual elements of information from the environment (SA Level 1), comprehending their collective meaning (SA Level 2), and finally projecting the meaning of that comprehension into the immediate future (SA Level 3). Only when the relevant information is perceived can its importance be understood and then used to predict where the situation may lead. In other words, SA serves as the foundation of our decision-making ability by constructing a mental model of a given situation and its near future, enabling us to predict the consequences of our actions. Our capacity to build SA is positively influenced by our experience, knowledge, and training. Conversely, factors like fatigue, excessive workload, and system complexity have a negative impact on it (Figure 1).6
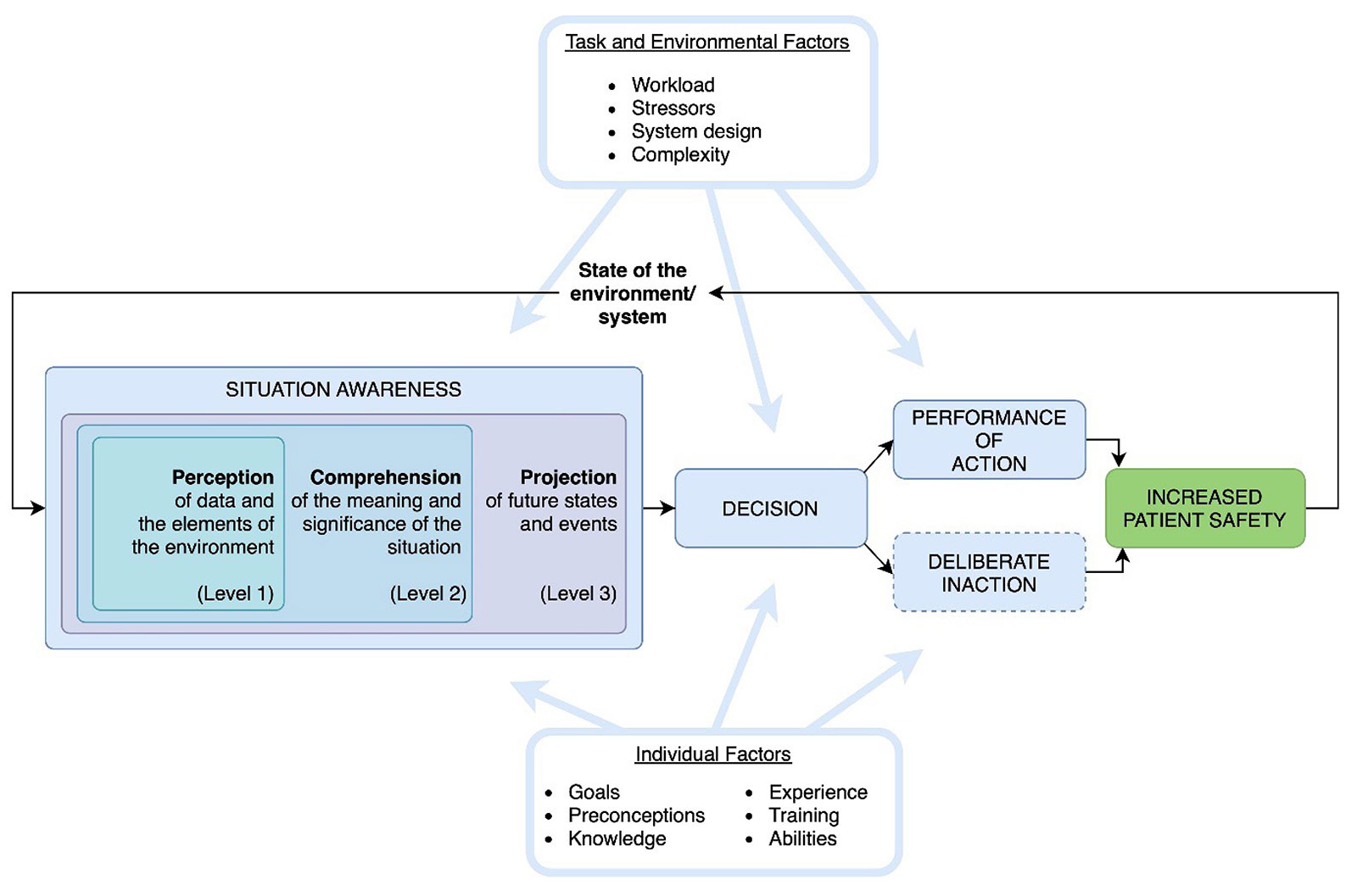
Figure 1: Depicts the three-tiered concept of situation awareness and factors that positively and negatively affect it. This is a public domain image created by the study authors.
Figure 1 illustrates that effective SA can lead to improved patient safety. To demonstrate this notion, consider an example from anesthesia practice: a care provider initially observes gradual drops in blood pressure, then an increase in the volume of blood in the suction canisters, and an increasingly nervous surgeon (SA Level I). Only then can they understand that this is likely a bleeding situation (SA Level II) and anticipate that, depending on the severity, assistance will be required (SA Level III). A decision can now be made to pick up the phone and call for help, thus initiating the next steps. Over time, the cycle must continuously repeat so that the specialist can adapt to new challenges and optimize patient safety. By reducing the effort required to build SA, caregivers can make patient safety decisions faster and with less workload.
Figure 1 is based on Endsley’s model of situation awareness,2 adapted by the authors to demonstrate the impact of situation awareness on patient safety. At least three quarters of errors in medicine, much like in aviation, are human errors, or ultimately situation awareness errors.
SITUATION AWARENESS: SIMILARITIES AMONG MEDICAL AND AVIATION ERROR
The World Health Organization states “First, do no harm” as the most fundamental principle of health care.7 Nevertheless, approximately one in ten patients experience adverse events in health care settings, with over 50% of harm deemed preventable.8,9 Typical adverse incidents that may lead to preventable harm to patients include medication errors, unsafe surgical practices (such as performance of non-routine procedures by inexperienced surgeons, wrong-site surgery, retained surgical instruments, or anesthesia-related errors), health care-associated infections, and incorrect diagnoses.7 Based on analyses of malpractice claims and critical incident reporting system cases, Schulz et al. found that three quarters or more of all errors in anesthesiology and intensive care can be attributed to deficiencies in SA.3,10
AVIATION AND SITUATION AWARENESS
In aviation, a parallel challenge exists, with approximately 80–85% of accidents attributed to SA problems.11 In fact, the three worst U.S. airline accidents in the last two decades—Asiana Airlines Flight 214 in San Francisco,12 Colgan Air Flight 3407 in Buffalo, NY,13 and Comair Flight 5191 in Lexington, KY14—were all attributed to SA errors. In the 1930s, decades before the term SA was coined, the aviation industry recognized that machines had become too complex for humans to operate them safely without checklists and has since achieved its current high safety standards by improving technology and training, implementing the use of standard operating procedures such as checklists, and increasing awareness to optimize SA.15
In medicine, Schulz et al. identified that the most common types of errors were Level I errors, in which the individuals failed to perceive information available to them in their environment, such as when a caregiver fails to notice a change in blood pressure because he or she is preoccupied with setting respiratory parameters. Misinterpretation of perceived information and incorrect projection of the situation into the near future were the second and third most common subtypes of errors.4,10 The top ten patient safety priorities listed by the Anesthesia Patient Safety Foundation are of paramount importance.16 As we address these priorities, it is essential to view them through the lens of SA optimization in order to maximize patient safety at its core.
WHAT CAN WE DO TO IMPROVE SITUATION AWARENESS AND PATIENT SAFETY?
To answer this central question, we need to consider the primary purpose of SA design: to efficiently transfer goal-relevant information to the decision-makers, enabling them to make informed and timely therapeutic decisions with minimal cognitive effort. In the book Designing for Situation Awareness, Mica Endsley, PhD, specifies eight points to consider when focusing on systems optimized for SA.6 When applied to health care, these include, but are not limited to, organizing and displaying relevant information around the care provider’s main goals to facilitate perception and understanding of the most important data, such as through the use of checklists or intuitive visualization techniques. In order for users to make efficient decisions while maintaining a comprehensive understanding of complex situations, critical cues must be easily identifiable through salient signals that attract our attention, such as through changes in color, form, or frequency. This can be accomplished by utilizing our innate parallel processing abilities and optimizing information delivery in accordance with the principles of human visual information processing. In addition, the implementation of novel technologies based on predictive algorithms can directly support level 3 SA projections.
We hope that these principles, when implemented in medicine, can help achieve the goal of the World Health Organization’s Global Patient Safety Action Plan: “to achieve the maximum possible reduction in avoidable harm due to unsafe health care globally”.7 The focus of safety design efforts should be to optimize SA from all angles by considering the task, environmental, and individual factors outlined in Figure 1.
Comparing SA in medicine and aviation, a person would need daily anesthesia for 548 years to encounter the 1:200,000 mortality risk estimated for a healthy patient,17 while flying daily for 25,000 years to face a fatal plane crash, as per the International Air Transport Association Safety Performance Report of 2023.18 Although these mortality events are uncommon, lack of SA leads to a much higher number of nonlethal critical incidents. It is important to address inadequate SA, as it is the root cause of most patient safety issues and can be improved through the application of SA-oriented design.
David W. Tscholl, MD, is a consultant of anesthesiology at the Institute of Anesthesiology, University and University Hospital Zurich, Zurich, Switzerland
Cynthia A. Hunn, MD, is a resident of anesthesiology at the Institute of Anesthesiology, University and University Hospital Zurich, Zurich, Switzerland.
Greta Gasciauskaite, MD, is a resident of anesthesiology at the Institute of Anesthesiology, University and University Hospital Zurich, Zurich, Switzerland.
David W. Tscholl, MD, has received grants, research funding, or honoraria from Koninklijke Philips N.V., Amsterdam, The Netherlands; Instrumentation Laboratory—Werfen, Bedford, MA. Swiss Foundation for Anaesthesia Research, Zurich, Switzerland; and the International Symposium on Intensive Care and Emergency Medicine Brussels, Belgium. Cynthia A. Hunn, MD, and Greta Gasciauskaite, MD, have no conflicts of interest.
REFERENCES
- Gaba DM, Howard SK, Small SD. Situation awareness in anesthesiology. Human Factors. 1995;37:20–31. PMID: 7790008.
- Endsley MR. Toward a theory of situation awareness in dynamic systems. Human Factors. 1995;37:32–64. doi: 10.1518/001872095779049543
- Schulz CM, Endsley MR, Kochs EF, et al. Situation awareness in anesthesia: concept and research. Anesthesiology. 2013;118:729–742. PMID: 23291626.
- Schulz CM, Burden A, Posner KL, et al. Frequency and type of situational awareness errors contributing to death and brain damage: a closed claims analysis. Anesthesiology. 2017;127:326–337. PMID: 28459735
- Schulz CM, Krautheim V, Hackemann A, et al. Situation awareness errors in anesthesia and critical care in 200 cases of a critical incident reporting system. BMC Anesthesiol. 2016;16:4. PMID: 26772179.
- Endsley MR. Designing for situation awareness: an approach to user-centered design. 2nd ed. CRC Press Inc. Boca Raton, FL, USA; 2011.
- World Health Organization. Patient safety. https://www.who.int/news-room/fact-sheets/detail/patient-safety. Accessed November 12, 2023.
- Slawomirski L, Klazinga N. The economics of patient safety: from analysis to action. Organisation for Economic Co-operation and Development. https://www.oecd.org/health/health-systems/Economics-of-Patient-Safety-October-2020.pdf. Accessed November 12, 2023.
- Panagioti M, Khan K, Keers RN, et al. Prevalence, severity, and nature of preventable patient harm across medical care settings: systematic review and meta-analysis. BMJ. 2019;366:l4185. PMID: 31315828.
- Schulz CM, Krautheim V, Hackemann A, et al. Situation awareness errors in anesthesia and critical care in 200 cases of a critical incident reporting system. BMC Anesthesiol. 2016;16:4. PMID: 26772179.
- Jones DG, Endsley MR. Sources of situation awareness errors in aviation. Aviat Space Environ Med. 1996;67:507–512. PMID: 8827130.
- Board NTS. Descent below visual glidepath and impact with seawall, Asiana Airlines Flight 214, Boeing 777-200ER, HL7742, San Francisco, California July 6, 2013. 2014. https://www.ntsb.gov/investigations/accidentreports/reports/aar1401.pdf. Accessed November 15, 2023.
- Board NTS. Loss of control on approach, Colgan Air, Inc., Operating as Continental connection flight 3407, Bombardier DHC-8-400, N200WQ, Clarence Center, New York, February 12, 2009. 2010. https://www.ntsb.gov/investigations/accidentreports/reports/aar1001.pdf. Accessed November 15, 2023.
- Board NTS. Attempted takeoff from wrong runway, Comair Flight 5191, Bombardier CL-600-2B19, N431CA, Lexington, Kentucky, August 27, 2006. 2007. https://www.ntsb.gov/investigations/AccidentReports/Reports/AAR0705.pdf. Accessed November 14, 2023.
- University of Calgary |VP Services| Environment HaS. Safety Moment. Use of checklists as an administrative control. https://www.ucalgary.ca/risk/sites/default/files/teams/13/EHS_SM__Use_of_Checklists_as_an_Administrative_Control.pdf. Accessed November 13, 2023
- Greenberg S. The APSF revisits its top 10 patient safety priorities. APSF Newsletter. 2021;36:48,53. https://www.apsf.org/article/the-apsf-revisits-its-top-10-patient-safety-priorities/
- Essentials CCH. How safe is anesthesia? 5 common concerns. https://health.clevelandclinic.org/safe-anesthesia-5-things-know. Accessed November 14, 2023.
- IATA. IATA releases 2022 airline safety performance. https://www.iata.org/en/pressroom/2023-releases/2023-03-07-01/. Accessed November 13, 2023.
