INTRODUCTION
Peripheral nerve blocks (PNB) are safe and effective alternatives or supplements to general anesthesia. They may improve pain control both during and after surgery, thus avoiding many of the side effects of systemic opioids. PNBs may also lead to improved patient satisfaction, decreased resource utilization, and may be better for the environment by decreasing usage of anesthetic gases and other medications.
The use of PNB has increased over time. One study using the National Anesthesia Clinical Outcomes Registry analyzed data from 12,911,056 outpatient surgeries between 2010 and 2015 and found a marked increase in overall PNB.1 With the growing use of peripheral nerve blocks in the United States, we want to examine safety issues surrounding the procedures. Specifically, we will examine the safety of nerve blocks as it relates to nerve injury, recognition, and treatment of local anesthetic systemic toxicity (LAST), and appropriate health care professional performance of timeouts to avoid wrong-sided blocks.
USING ULTRASOUND-GUIDED PERIPHERAL NERVE BLOCKS TO ENHANCE PATIENT SAFETY
Ultrasound-guided PNBs have rapidly become the preferred approach among many anesthesia professionals. The use of ultrasound guidance when compared to peripheral nerve stimulation may lead to significantly improved block success, decreased need for rescue analgesia, decreased pain during performance of the block, and lower rates of vascular and pleural puncture. While there is no convincing evidence that ultrasound-guided regional anesthesia reduces the risk of pneumothorax for certain blocks such as paravertebral and supraclavicular blocks, the ability to visualize the pleura may provide confidence that the pleural space has not been violated.2
It has been suggested that the risk of nerve injury would be further reduced by utilizing ultrasound to directly visualize the needle and target nerve. However, the existing literature generally does not support the argument that ultrasound-guided blocks reduce the incidence of postoperative neurologic symptoms as compared with other techniques such as peripheral nerve stimulation. The primary source of PNB-mediated neurologic injury is likely mechanical injury to the fascicle and/or injection of local anesthetic into a fascicle causing myelin and axonal degeneration. Fortunately, most neurologic symptoms after PNB are transient. The incidence of long-term nerve injury reported from the 3 largest registries is 4 per 10,000 peripheral nerve blocks, which is similar to the historic incidence associated with peripheral nerve stimulation guided blocks.2 Part of this lack of difference may be due to the quality of the ultrasound equipment and the skill of the proceduralist in identifying the intended nerve. Operators may not adequately visualize the needle tip and misinterpret surrounding artifacts. Needle movement and/or hydrodissection may not ensure lack of needle to nerve contact or vascular injection of local anesthetics. In another registry, the incidence of adverse events across all peripheral regional anesthetics was 1.8 per 1,000 blocks for postoperative neurologic symptoms lasting longer than 5 days, but only 0.9 per 1,000 blocks for postoperative neurologic symptoms lasting longer than 6 months.3 It is worth noting that patients with preexisting neuropathy may be at an increased risk of postoperative neurologic dysfunction. Avoidance of intraneural injection is of paramount importance to patient safety.4
Conversely, the use of ultrasound does significantly reduce the risk of LAST. A recent study provided strong evidence that the use of ultrasound may play a part in decreasing the incidence of LAST.5 Ultrasound guidance allows for real-time guidance of the needle to avoid vascular injury and subsequent intravascular injection of local anesthetic. While the use of ultrasound minimizes the incidence of LAST (2.7 per 10,000 cases), strict attention must still be directed to this possibility and providers should be ever vigilant for its occurrence.6
LOCAL ANESTHETIC SYSTEMIC TOXICITY
In 1998, Weinberg and colleagues published the first case report suggesting that an infusion of a soybean oil emulsion, which was normally used for total parenteral nutrition solution, could prevent (by pretreatment) or reverse cardiac arrest caused by bupivacaine overdose in the intact, anesthetized rat.7 It was almost two decades later that a LAST report was published concerning a patient undergoing a PNB for shoulder surgery, who subsequently developed cardiac arrest. The patient failed to respond to standard resuscitative efforts for approximately 20 minutes, but achieved normal vital signs shortly after receiving a 100 ml bolus of lipid emulsion. The patient had a complete recovery with no neurologic deficits or cardiovascular sequelae.8
The American Society of Regional Anesthesia and Pain Medicine in 2010 published its LAST checklist, which has undergone revisions in 2012, 2017, and most recently in 2020.9 (Figure 1). The checklist was revised most recently due to simulation and user feedback that highlighted the failure to emphasize the differences between LAST resuscitation efforts and Advanced Cardiac Life Support (ACLS)-guided resuscitation. Animal studies have demonstrated some of the standard medications used for ACLS, such as code dose epinephrine and vasopressin, worsen outcomes in LAST.10,11 When simulation subjects chose to use both LAST and ACLS checklists, the resulting confusion and missteps led to delayed and sometimes wrong treatment. Admonitions were placed at the top of previous checklists, but these did not eliminate the placed errors. The 2020 redesign was purposed to incorporate a standard triangular caution sign to highlight the differences between LAST and ACLS resuscitation. The 2020 update also simplified lipid emulsion dosing for patients over 70 kg to a single 100 ml bolus followed by an infusion rather than employing a weight-based calculation.9
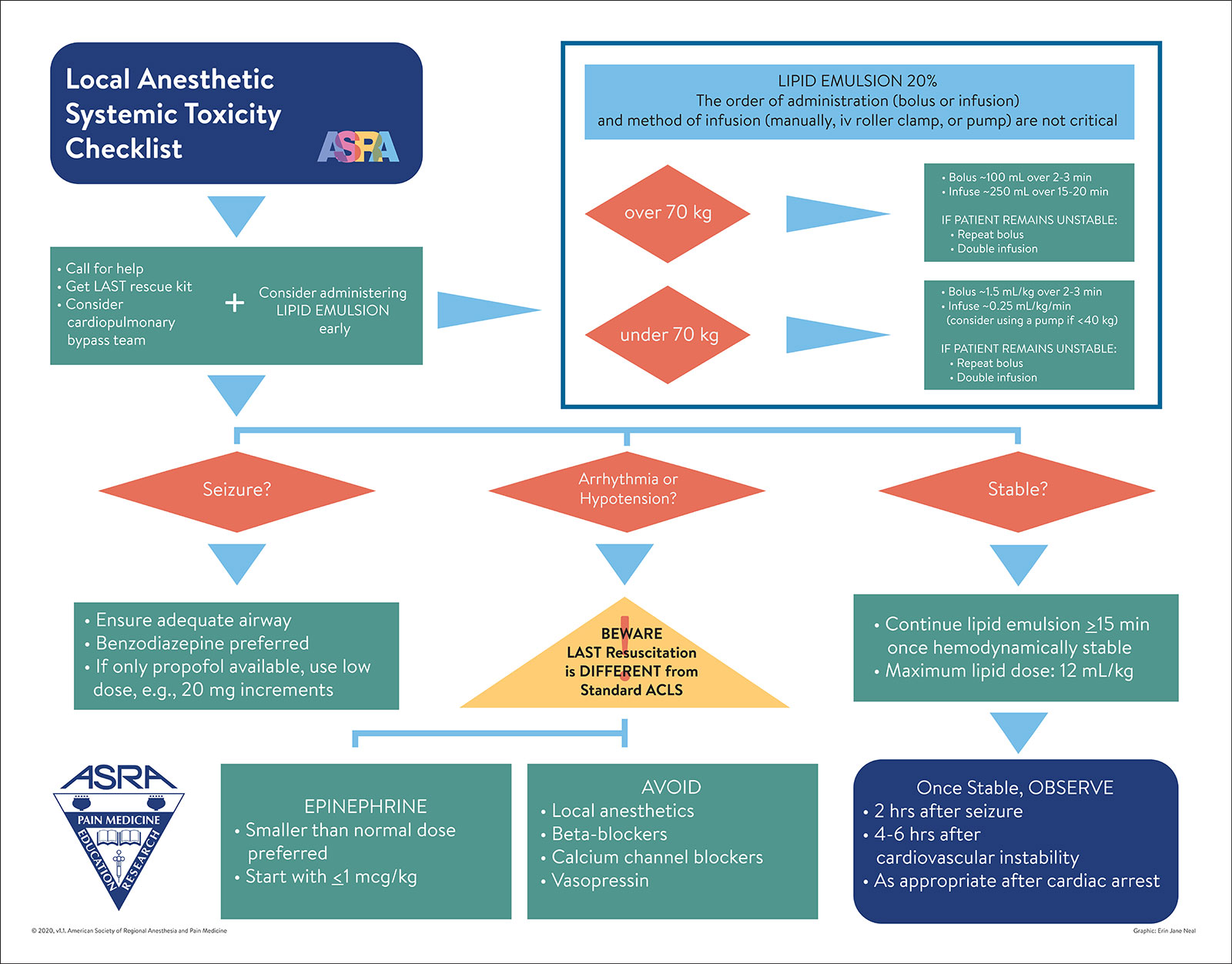
Figure 1. Local Anesthetic Systemic Toxicity Checklist.
Used with the permission of the American Society of Regional Anesthesia and Pain Medicine.
THE RISK OF PERIPHERAL NERVE BLOCKS UNDER SEDATION
It has been a quarter of a century since a case report brought to everyone’s attention the risk of placing a thoracic epidural in a patient while under general anesthesia.12 The patient suffered a spinal cord injury after four attempts at epidural placement. However, there is scant literature in the adult population that provides guidance as to the safety or risk of placing regional blocks in patients under general anesthesia. In the pediatric population, placing regional blocks in anesthetized patients is considered safe. This comes from data from the Pediatric Regional Anesthesia Network, a multi-institutional research consortium which created a registry of more than 50,000 regional anesthetic blocks in children under 18 years of age.13 Conversely, in adult patients, based on no rigorous scientific evidence, the primary practice is placing regional anesthetics in patients prior to induction of general anesthesia. Sedation may improve the safety and success of block placement and lead to greater patient satisfaction by enhancing the operating conditions for the anesthesia professionals performing the block.14 Additional studies are needed to determine the true risk and benefit of placing PNBs under general anesthesia in adults.
PREVENTION OF WRONG-SIDED BLOCKS
Wrong-Sided Blocks are “Never Events” That Still Occur
Wrong-sided procedures are considered “Never Events,” but still occur at a rate of 7.5 per 10,000 procedures.15 The term “Never Event” was first introduced in 2001 by Ken Kizer, MD, former CEO of the National Quality Forum (NQF), in reference to egregious medical errors that should never happen.16 Over time, the term’s use has been extended to designate adverse events that are unambiguous, serious, and usually preventable. Since the initial Never Event list was developed in 2002, it has been revised multiple times over the years and now comprises 29 “serious reportable events” grouped into 7 categories.17
There are certain characteristics identified in most wrong-sided blocks (Table 1). Prior to starting the nerve block, visual confirmation of the correct procedure location is performed by both the patient and nurse using institution-specific standards, which can include placing a wristband marked with the word “yes” on the side corresponding to the surgery or marked clearly by the surgeon or provider performing the procedure. Involving the patient in the process prior to receiving sedation or anesthesia leads to decreased error and may enhance patient satisfaction as patients may feel they are active participants in the process and gain confidence in their providers.14
Table 1: Factors that Contribute to Wrong-Sided Blocks15
| Characteristics of Wrong-Sided Blocks |
| Failure to verify site preoperatively |
| Failure to mark area adequately by the surgeon |
| Rushed, inadequate, or absent anesthesia timeout |
| Distractions |
| Patient position changes |
| Scheduling changes |
| Poor communication |
The clinician placing the regional anesthetic block should discuss the operative/invasive procedure with the patient before administering anesthesia/moderate sedation. The patient should verbalize agreement of the correct procedure and surgical site, and the discussion and patient verbalization should be documented on the consent form. Communication barriers (e.g., sight and hearing impairments, a non-English-speaking patient, as well as the patient’s emotional status) should be addressed by all providers so that the patient is able to fully participate in preoperative discussions. Measures taken to address communication barriers should be documented in the medical record.
All relevant documentation including the consent form, history of present illnesses, and diagnostic data should be verified by the preprocedural nurse/procedural team. If there are any discrepancies or uncertainties, the preprocedural nurse/procedural team should call the surgeon for clarification prior to starting the procedure.
Immediately prior to performing the peripheral nerve block, the proceduralist should engage in the “Universal Protocol” and take a preprocedural “timeout” (Figure 2). “Timeout” must be performed immediately prior to incision or starting the procedure. The “timeout” process should be conducted in the location where the procedure will be done and should involve the immediate members of the procedural team, including the individual performing the procedure, the circulating nurse, and other active participants who will be participating in the procedure from the beginning.

Figure 2. Workflow for Timeout Procedure for Performing a Peripheral Nerve Block.
At a minimum the following should be done before performing a regional block:
When the anesthesia professional is about to begin the regional anesthesia block, they should confirm the site is marked by the individual performing the block using the same method as described above. This has been our practice, but other institutions may have different protocols in place.
CONCLUSION
In summary, regional anesthesia is a safe supplement or alternative to general anesthesia that can improve patient satisfaction and decrease opioid usage along with its side effects. While nerve blocks are already quite safe, it is essential to ensure maximum safety while delivering excellent care. As the utilization of regional anesthesia continues to grow, it is imperative for us to perform regional anesthesia blocks as safely as possible by considering ultrasound guidance when available, understanding LAST recognition and resuscitation, and executing proper pre-procedural checklists to avoid wrong-sided blocks.
Christina Ratto, MD, is a clinical assistant professor at the Keck School of Medicine, Los Angeles, CA.
Joseph Szokol, MD, JD, MBA, is a clinical professor at the Keck School of Medicine, Los Angeles, CA.
Paul Lee, MD, MS, is a clinical assistant professor at the Keck School of Medicine, Los Angeles, CA.
The authors have no conflicts of interest.
REFERENCES
- Gabriel RA, Ilfeld BM. Use of regional anesthesia for outpatient surgery within the United States: a prevalence study using a nationwide database. Anesth Analg. 2018;126:2078–84. PMID: 28922231.
- Neal JM, Brull R, Horn JL, et al. The Second American Society of Regional Anesthesia and Pain Medicine evidence-based medicine assessment of ultrasound-guided regional anesthesia: executive summary. Reg Anesth Pain Med. 2016;41:181–194. PMID: 26695878.
- Sites BD, MD, Taenzer AH, Herrick MD. Incidence of local anesthetic systemic toxicity and postoperative neurologic symptoms associated with 12,668 ultrasound-guided nerve blocks an analysis from a prospective clinical registry. Reg Anesth Pain Med. 2012;37:478–482. PMID: 22705953.
- Brull R, McCartney C, Chan V. El-Beheiry H. Neurological complications after regional anesthesia: contemporary estimates of risk. Anesth Analg. 2007;104:965–975. PMID: 17377115.
- Barrington MJ, Kluger R. Ultrasound guidance reduces the risk of local anesthetic systemic toxicity following peripheral nerve blockade. Reg Anesth Pain Med. 2013; 38:289-99. PMID: 23788067.
- El-Boghdadly K, Pawa A, Chin KJ. Local anesthetic systemic toxicity: current perspectives. Local Reg Anesth. 2018;11:35–44. Published online 2018 Aug 8. PMID: 30122981.
- Weinberg GL, VadeBoncouer T, Ramaraju GA, et al. Pretreatment or resuscitation with a lipid infusion shifts the dose-response to bupivacaine-induced asystole in rats. Anesthesiology. 1998;88:1071–1075. PMID: 9579517.
- Rosenblatt MA, Abel M, Fischer GW, et al. Successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine-related cardiac arrest. Anesthesiology. 2006;105:217–218. PMID: 16810015.
- Neal JM, Neal EJ, Weinberg GL. American Society of Regional Anesthesia and Pain Medicine local anesthetic systemic toxicity checklist: 2020 version. Reg Anesth Pain Med. 2021;46:81–82. PMID: 33148630.
- Hiller DB, Di Gregorio G, Ripper R, et al. Epinephrine impairs lipid resuscitation from bupivacaine overdose. Anesthesiology. 2009;111:498–505. PMID: 19704251.
- Di Gregorio G, Schwartz D, Ripper R, et al. Lipid emulsion is superior to vasopressin in a rodent model of resuscitation from toxin-induced cardiac arrest. Crit Care Med. 2009;37: 993–999. PMID: 19237909.
- Bromage PR, Benumof JL. Paraplegia following intracord injection during attempted epidural anesthesia under general anesthesia. Reg Anesth Pain Med. 1998;23:104–107. PMID: 9552788.
- Taenzer AH, Walker BJ, Bosenberg AT, et al. Asleep versus awake: does it matter? Pediatric regional block complications by patient state: a report from the Pediatric Regional Anesthesia Network. Reg Anesth Pain Med. 2014;39: 279–283. PMID: 24918334.
- Kubulus C, Schmitt KC, Albert N, et al. Awake, sedated or anaesthetised for regional anaesthesia block placements? A retrospective registry analysis of acute complications and patient satisfaction in adults. Eur J Anaesthl. 2016;33:715–724. PMID: 27355866.
- Barrington MJ, Uda Y, Pattullo SJ, Sites BD. Wrong-site regional anesthesia: review and recommendations for prevention? Curr Opin Anesthesiol. 2015;28:670–684. PMID: 26539787.
- Kizer KW, Stegun MB. Serious reportable adverse events in health care. In: Henriksen K, Battles JB, Marks ES, et al., eds. Advances in patient safety: from research to implementation (volume 4: programs, tools, and products). Advances in Patient Safety. Rockville, 2005:339–352.
- Agency for Healthcare Research and Quality. Patient Safety Network. Never events.https://psnet.ahrq.gov/primer/never-events Accessed December 13, 2023.
