APSF’s annual Pierce Memorial lecture this year, titled “Integrating Behavior and Technology for Anesthesia Patient Safety,” was delivered October 14, 2023, during the ASA Annual Meeting in San Francisco.
Ellison C. “Jeep” Pierce, Jr., MD, the inspirational founding President of the APSF (Figure 1), first considered anesthesia patient safety as a junior attending when he was assigned to give a lecture on “anesthesia accidents.” The topic later became a consuming passion, fueled in part by the tragic death of a friend’s daughter from an unrecognized accidental esophageal intubation during an anesthetic for dental surgery. As Chief of Anesthesia at New England Deaconess/Harvard, he collected accident case reports from all over the country and often lamented the significant number of deaths from esophageal intubations.

Figure 1: Ellison C. (Jeep) Pierce, Jr., MD (1929–2011): Chairman, New England Deaconess Hospital; ASA President; founding President, Anesthesia Patient Safety Foundation.
A 1982 television exposé/documentary, “The Deep Sleep: 6000 Will Die or Suffer Brain Damage,”1 detailing catastrophic anesthesia accidents, attracted great public attention. This coincided with E.C. Pierce’s impending American Society of Anesthesiologists (ASA) presidency and gave him the opportunity to initiate attention and projects on patient safety within the ASA. Awareness of anesthetic mishaps in England stimulated E.C. Pierce, MD, along with Jeff Cooper, PhD, and Richard Kitz, MD, both from Mass General/Harvard to convene in Boston in 1984 the “International Conference on Preventable Anesthesia Mortality and Morbidity,” immediately after which the APSF was conceived—with the intent of involving physicians, CRNAs, as well as relevant corporate and regulatory entities—completely independent of the bureaucratic inhibitions of government and large organizations. Based on my prior experience as a newspaper reporter and editor, E.C. Pierce, MD, asked me to create and edit the APSF Newsletter, which was and is still the largest circulation anesthesia publication in the world. A 2010 special issue recounts the history of the first 25 years of the APSF.2
Coincidentally at the same time, the captive company providing malpractice insurance to all Harvard faculty physicians and hospitals came to the nine Harvard hospital Chiefs of Anesthesia with the concern that anesthesia claims were excessive: anesthesiologists were 3% of the faculty, but generated 12% of the insurance company payout.3 To investigate and address this problem, the Harvard Risk Management Committee was created. I was named Chair of that committee, because of an episode the previous year in which I directed the investigation and remediation of a catastrophic oxygen pipeline accident at an Army hospital in Alabama. The committee studied in great detail all the Harvard anesthesia malpractice claims from the creation of the insurance company in 1976 through 1984 and realized that most of the catastrophic accidents involved unrecognized issues with patient ventilation. The Harvard Standards for intraoperative monitoring4 were created—not guidelines or recommendations, but mandatory standards of care, so that the medical-legal implication of ignoring them was perfectly clear. After some convincing, these standards were adopted at Harvard on July 1, 1985. The last catastrophic accident that would have been prevented by safety monitoring of that era in the Harvard system occurred the following month. Importantly, while the behavior of continuous monitoring of ventilation and circulation were required as core principles of this “safety monitoring,” the technologies of capnography and pulse oximetry were only mentioned as possible methods. These technologies did not become mandatory standards until several years later when the profession in general recognized their enormous value in extending the human senses, thus providing much earlier warning of untoward developments (such as an esophageal intubation) and allowing for more timely diagnoses and institution of corrective treatment. Demonstrating the dramatic efficacy of safety monitoring in virtually eliminating intraoperative catastrophic anesthesia accidents was not amenable to the classic statistically significant p value of less than 0.05 seen in randomized prospective controlled trials. However, great success was clear as malpractice insurance premiums for Harvard anesthesiologists decreased by 66% from 1986–1991. Large reductions in premiums could only come from substantial decreases in the number and severity of anesthesia accidents. Further, a retrospective analysis5 of the catastrophic accidents that provoked the monitoring standards in the first place showed that application of the principles of safety monitoring would have prevented those patient-injury events.
STANDARDS SPREAD
The Harvard monitoring standards inspired the expanded ASA Standards for Basic Intraoperative Monitoring6 (essentially every anesthesia record today, paper or electronic, has a check box for “ASA monitors applied”), which, in turn, led to the creation by an independent group of what became the much-expanded World Federated Societies of Anesthesia International Standards, first adopted in 1992, with multiple updates in the years since.7 Careful appreciation of all the standards over the years reveals that, as important as the monitoring devices and technologies are, it is the behavior of the anesthesia professionals interpreting and reacting to the generated signals that is the final common pathway for maintaining anesthesia patient safety.
Current intraoperative monitoring practices are prescribed by the ASA Standards and, also, the 2023 ASA Practice Parameter on monitoring and antagonism of neuromuscular blockade,8 which strongly recommends quantitative rather than qualitative monitoring of ulnar nerve train-of-four count. Brain monitoring is covered by an ASA “Practice Advisory,” but the APSF published revised recommendations9 for (among other things) awareness prevention using processed EEG. Use of video laryngoscopes for all intubations is not yet addressed, but significant published research favors this, and it may become a recommendation or even a de facto standard of care in the future.
DISTRACTION DANGER
A dangerous misperception about patient safety may exist among anesthesia professionals because now there are far fewer catastrophic intraoperative patient injuries from lack of monitoring than in the 1970s. This remarkable success, considering that what we do is inherently dangerous, can lead to complacency and a relaxation of vigilance, which is, after all, the ASA motto. Distractions have always existed, but today the issue is computers, tablets, and cell phones in the operating room, and the anesthesia professional being on social media, or surfing the internet, shopping on Amazon or E-Bay, gaming, texting, or even talking on the phone. Debate has occurred and opinions can differ, but it is undeniable that if a patient-injury event occurs when anesthesia personnel are voluntarily distracted, as testified to by others in the operating room at the time, the legal liability could be dramatic.10 One possibly related idea is whether there could be an eventual role for continuous high-resolution multi-angle audio-video recording of the monitors of all the activity in the operating room. Highly accurate technology exists,11 but the costs and legal implications likely would influence this new integration of cutting-edge technology with human behavior.
ADDITIONAL TECHNOLOGY ADVANCES
The Next Frontier of Safety Technology Has Begun
Advanced technology applications are integrating with direct bedside intensive care unit (ICU) management at the University of Pennsylvania, where a remote monitoring system, with two-way audiovisual connections, covers more than 450 ICU beds from one central location, is integrated with the electronic health record, and can provide early-warning alerts.12 A fascinating speculative corollary is whether, one day, such a system might be applicable also to anesthesia care.
“Smart” alarms are a logical step in integrating technology and clinician behavior during anesthetics in the operating room. Safety monitoring is intended to provide the earliest possible warning of abnormal or untoward signals from multiple simultaneous measurements and, thus, maximize time for appropriate response to prevent danger/injury. The original 1988 idea of smart alarms13 was to pull all the monitoring signals and alarms into one display. Much evolution, research, development, and testing has occurred since then, the most dramatic of which has been developed by researchers from the University of Michigan, where the “Alert Watch® OR” system with its multiple iterations provides a reactive decision support system with a graphical human-machine interface that was inspired by the multifunction primary flight display used by pilots in modern aviation. It not only alerts anesthesia professionals to abnormalities, but it can also suggest a cause and confirmatory testing (Figure 2). An extensive report14 concluded that, so far, the system improved process measures, but not postoperative clinical outcomes.
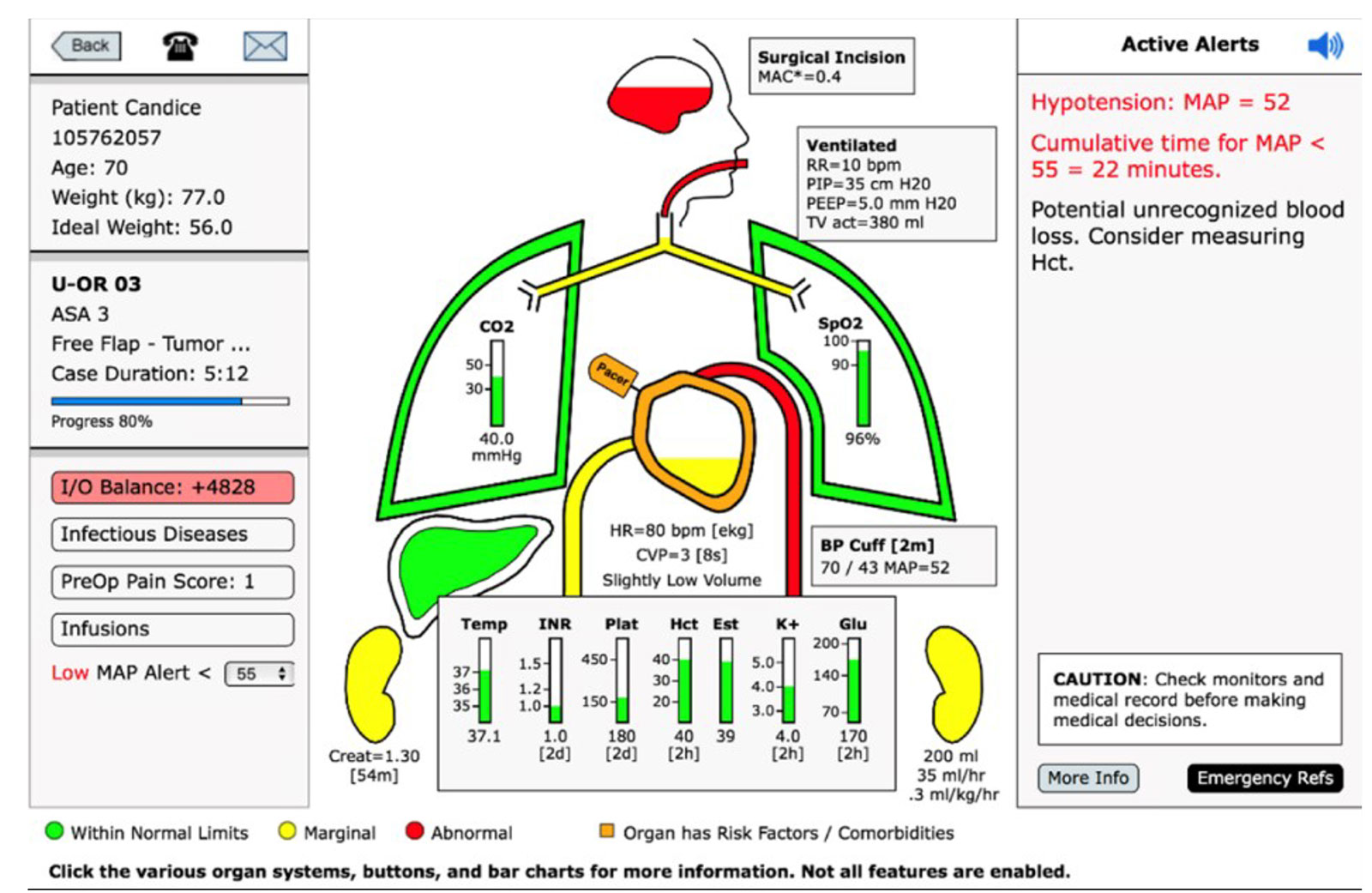
Figure 2. Prototype sample monitor/alert/decision support screen from “Alert-Watch OR.”18
SMARTER ALARMS AND AI
Smarter Alarms May Enhance the Technology-Behavior Interface
“Smarter” alarms are a bridge toward the application of artificial intelligence to anesthesia care. They enhance the technology-behavior interface by introducing machine learning and predictive analytics. Multiple studies have demonstrated programs that automatically analyze arterial line waveforms and predict hypotension during an anesthetic, 5–15 minutes in advance. Of course, it is the clinician’s response that determines the value of the warning. A step closer to artificial intelligence is a system that preoperatively considers all patient characteristics and parameters to predict hypotension following the induction of general anesthesia. Retrospective analysis showed this system to be 72% accurate, which the researchers considered “modest performance.”15
True AI (and maybe the robots of the future directed by it) is not here yet, but it is a popular topic.16 The potential appears limitless. A system developed at Michigan is being studied which considers all factors for a patient, predicts risks of adverse outcomes, weighs the potential “burden” of each, considers potential actions to mitigate each, and then calculates which action leads to the least overall burden, thus rendering a judgment and recommendation.15 Predictions for expanding AI to the entirety of perioperative medicine are offered in a remarkable recent article,17 with a fascinating illustration (Figure 3).
Implementation of Artificial Intelligence is Analogous to Safety Monitoring in 1980s
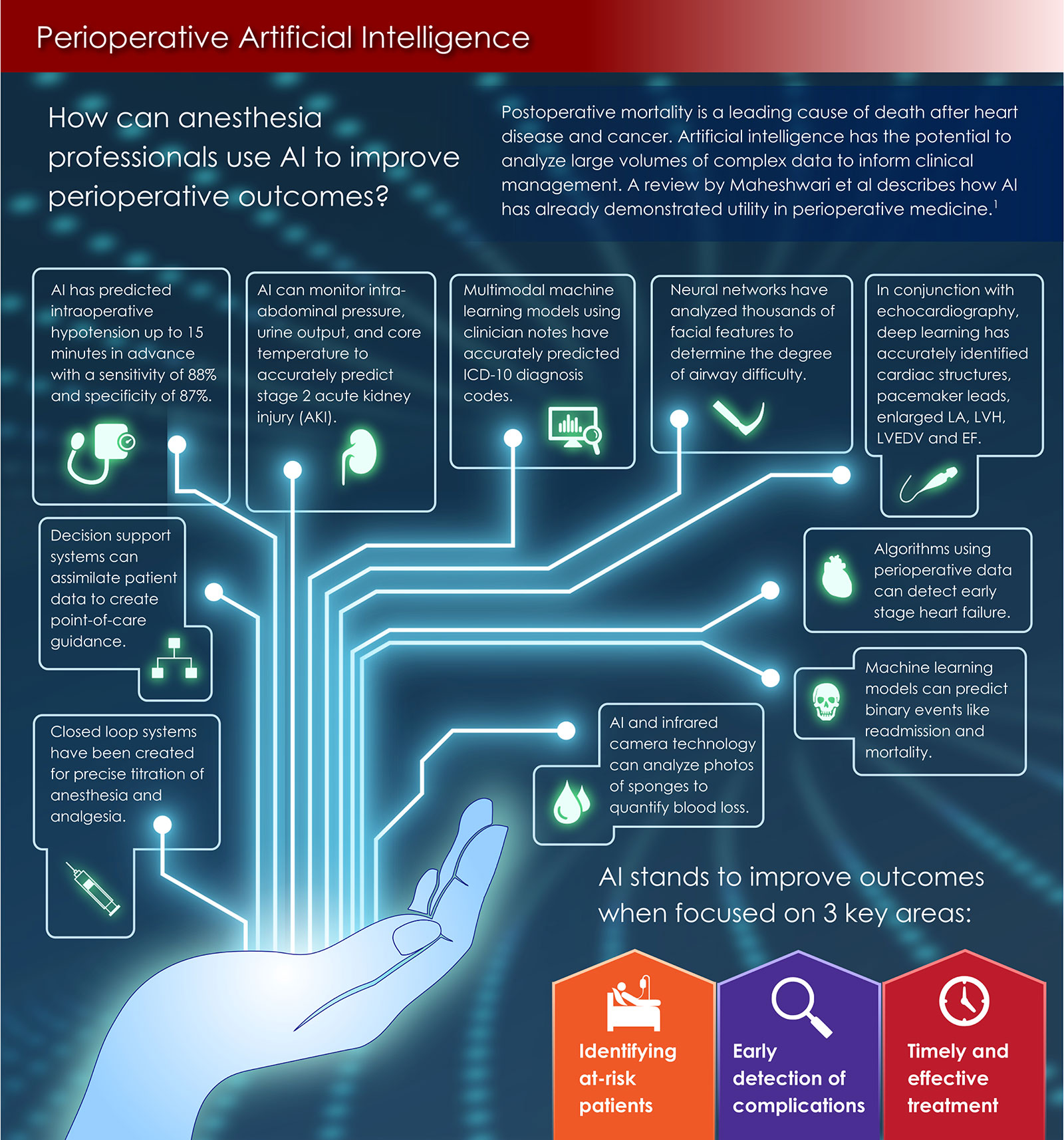
Figure 3. Perioperative artificial intelligence application models.19 Permission for use and modification granted from Anesthesia & Analgesia. Nathan N. Perioperative artificial intelligence: infographic. Anesth Analg. 2023;136:636.
So far, technology cannot replace the human behavior it must elicit. The intraoperative pattern is always the same—the earliest possible alert to untoward developments allows maximum time for corrective diagnosis and response. Implementation of AI is essentially an analogy to the adoption of “safety monitoring” strategy in the late 1980s (particularly with its vast extension of human senses by the sensitivity/accuracy of capnography and pulse oximetry)—which led to the virtual elimination of intraoperative anesthesia catastrophes. Practice improvements from AI will not be as obvious or dramatic when compared to the implementation of the original safety monitoring standards, but may become the standard of care. This is excellent, but, as Jeep Pierce, the APSF inspirational founding leader who is honored through this lectureship, reminded us: we must be ever “vigilant” (the ASA motto), because there will always be human error.
John H. Eichhorn, MD, the 2023 APSF Pierce Memorial lecturer, was the founding editor and publisher of the APSF Newsletter. Living in San Jose, CA, as a retired professor of anesthesiology, he continues to serve on the APSF Editorial Board.
The author has no conflicts of interest.
REFERENCES
- Janice Tomlin (producer): The Deep Sleep: 6,000 will die or suffer brain damage, WLS-TV Chicago, 20/20. April 22, 1982
- Eichhorn JH. The APSF at 25: pioneering success in safety, but challenges remain. APSF Newsletter 2010;25:21-24,35–39. PMID: 22253277. Accessed December 14, 2023.
- Eichhorn JH. The history of anesthesia patient safety. In: Ball C, Bacon D, Featherstone P (eds,) Broad horizons—the history of anesthesia beyond the operating room. International Anesthesiology Clinics. 2018;56:56-93.
- Eichhorn JH, Cooper JB, Cullen DJ, et al. Standards for patient monitoring during anesthesia at Harvard Medical School. JAMA. 1986;256:1017–1020. PMID: 3735628.
- Eichhorn JH. Prevention of intraoperative anesthesia accidents and related severe injury through safety monitoring. Anesthesiol. 1989;70:572–577. PMID: 2929993.
- American Society of Anesthesiologists. Standards for Basic Anesthetic Monitoring. (last amended October 20, 2010) (original approval: October 21, 1986) ( https://www.asahq.org/standards-and-practice-parameters/standards-for-basic-anesthetic-monitoring ).
- Merry AF, Cooper JB, Soyannwo O, et al. International standards for a safe practice of anesthesia. Can J Anesth. 2010;57:1027–1034. PMID: 20857254.
- ASA Task Force on Neuromuscular Blockade. 2023 American Society of Anesthesiologists practice guidelines for monitoring and antagonism of neuromuscular blockade. Anesthesiol 2023;138:13–41. PMID: 36520073.
- Committee on Technology. APSF-endorsed statement on revising recommendations for patient monitoring during anesthesia. APSF Newsletter. 2022;37:7–8. (https://www.apsf.org/article/apsf-endorsed-statement-on-revising-recommendations-for-patient-monitoring-during-anesthesia/.) Accessed November 30, 2023.
- Thomas BJ. Distractions in the operating room: an anesthesia professional’s liability? APSF Newsletter. 2017;31:59–61. (https://www.apsf.org/article/distractions-in-the-operating-room-an-anesthesia-professionals-liability/) Accessed November 30, 2023.
- Michaelsen, K. Cameras in the OR: reimaging patient safety. ASA Monitor. 2023;37:38. doi: 10.1097/01.ASM.0000949632.42292.92
- Scott, M. “The Tele-ICU – Now and in the Future.” APSF Stoelting Conference, Las Vegas, NV; September 7, 2023. (www.apsf.org)
- Watt RC, Miller KE, Navabi MJ, et al. An approach to “smart alarms” in anesthesia monitoring. Anesthesiol. 1988;89:A241. doi: 10.1097/00000542-198809010-00240
- Kheterpal S, Shanks A, Tremper K. Impact of a novel multiparameter decision support system on intraoperative processes of care and postoperative outcomes. Anesthesiol. 2018;128:272–282. PMID: 29337743.
- Mathis M. “Machine learning & predictive analytics.” APSF Stoelting Conference, Las Vegas, NV; September 6, 2023. (https://www.apsf.org/event/apsf-stoelting-conference-2023/). Accessed December 8, 2023.
- Kennedy S. “Exploring the Role of AI in Anesthesiology.” Health IT Analytics, July 20, 2023. (https://healthitanalytics.com/features/exploring-the-role-of-artificial-intelligence-in-anesthesiology )
- Maheshwari K, et al. Artificial intelligence for perioperative medicine: perioperative intelligence. Anesth Analg. 2023;136:637–45. PMID: 35203086.
- Tremper KK, Mace JJ, Gombert JM. et al. Design of a novel multifunction decision support display for anesthesia care: AlertWatch® OR. BMC Anesthesiol. 2018;18:16. PMID: 29402220.
- Nathan N. Perioperative artificial intelligence: infographic. Anesth Analg. 2023;136:636. PMID: 36928148.
