We submit that the preponderance of published literature suggests that perioperative handoffs are associated with patient harm, and that this harm may be mitigated by handoff standardization. However, many questions remain about the optimal conduct of perioperative handoffs. In this article, we describe evidence for the associations between handoffs and outcomes and the limited available evidence for what handoff practices are best for avoiding harm.
All Handoffs Are Not The Same
Perioperative handoffs are heterogeneous in settings, participants, and objectives. One way to categorize perioperative handoffs is by where and when they occur, e.g., preoperatively from floor-to-operating room (OR) or intensive care unit (ICU)-to-OR, and postoperatively from OR-to-ICU (see article by Dr. Lorinc in this issue). Another approach, proposed by Lane-Fall and colleagues, is a three-part taxonomy of handoffs based upon the type of transfer of care:
(1) shift changes, in which interchangeable clinicians exchange places (as in an intraoperative handoff between in-room anesthesia professionals), (2) duty relief, in which one clinician is relieved for a short time with the expectation of return (as with a meal break), and (3) transitions in care, during which a patient’s care is transferred from one team to another, and in which the patient may be moved from one site of care to another (as with OR-to-post-anesthesia care unit (PACU) or OR-to-ICU handoffs).1
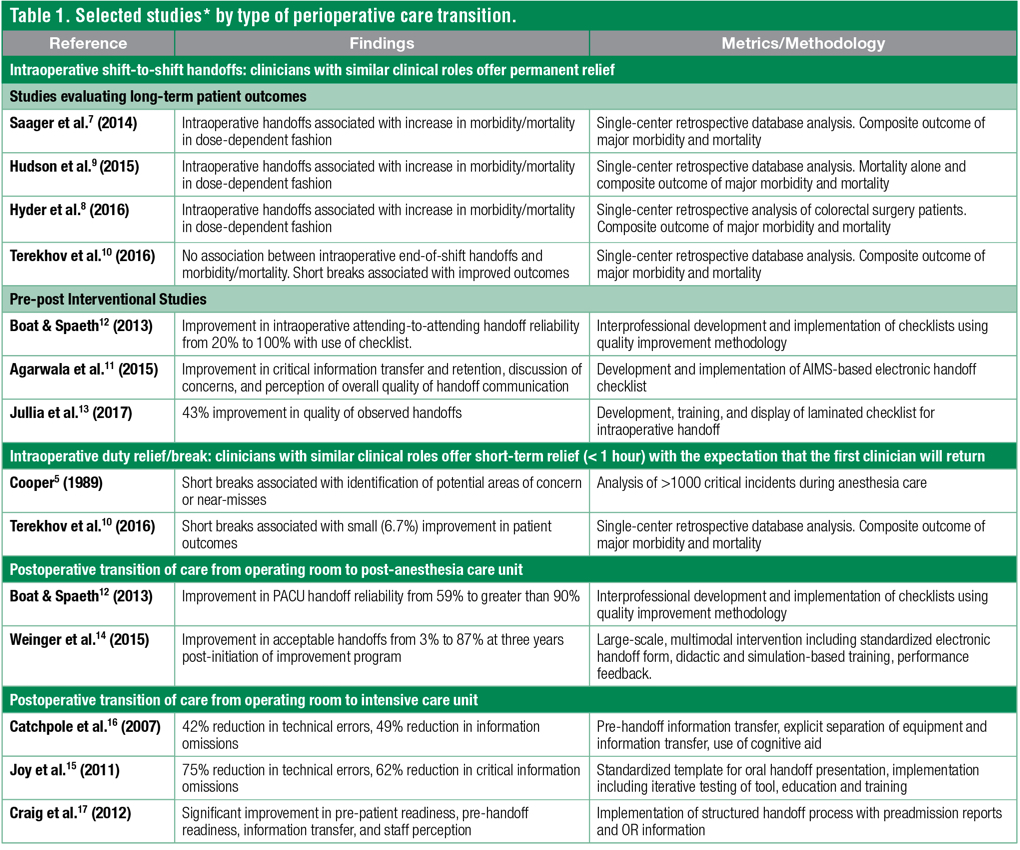
These three handoff types are variably represented in the published literature; transition articles outnumber shift change articles, which outnumber those addressing duty relief. A 2012 review offers an in-depth treatment of anesthesia handoffs.2 Here, we describe the evidence linking handoffs to patient outcomes, organized by the type of care transfer.
Shift change. Cooper and colleagues, more than 30 years ago, were the first to identify intraoperative handoffs as a patient safety concern.3-5 They found that handoffs could be an element in causing harm, but equally, if not more importantly, handoffs presented an opportunity: a fresh set of eyes could catch potential safety hazards, such as down-trending blood pressure or an empty vaporizer. In a later paper, Cooper suggested a checklist for conducting handoffs, but without a study of its effectiveness (Figure 1).5 Very few studies were published on the topic again until the 2000s, when Arbous et al. found a protective effect of having no intraoperative change of anesthesiologist in a retrospective case-control study.6 In the past few years, four retrospective single-center database studies have specifically investigated whether there is an association between intraoperative handoffs and patient adverse events.7-10 Three of the four studies found that handoffs were associated with an increased risk of composite outcomes including mortality,7-9 while a fourth found no such association.10
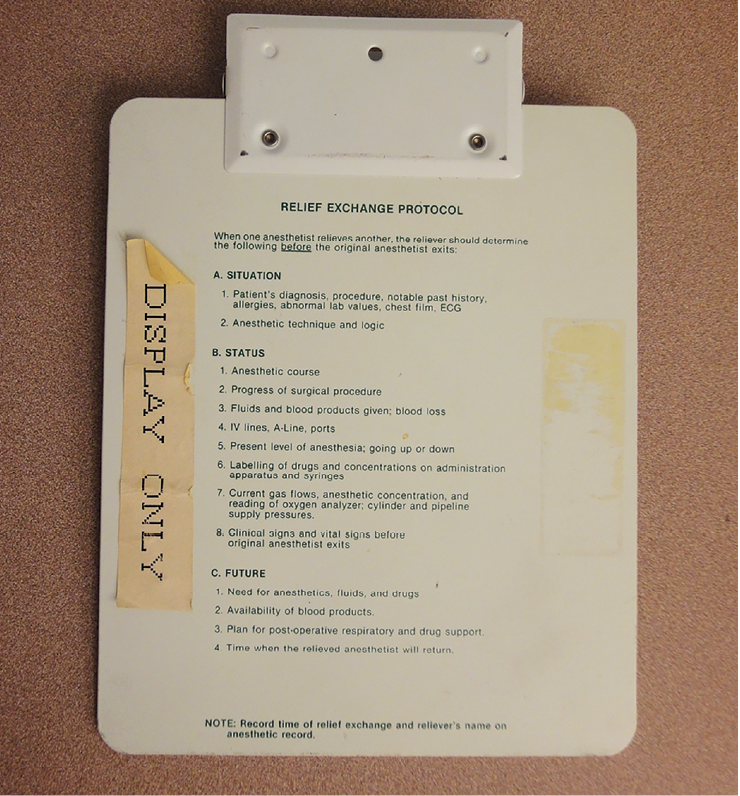
Figure 1. Cooper’s suggested checklist for intraoperative handoff, as printed on the back of a clipboard.
Few intraoperative handoff studies have included handoff interventions, and these have been primarily pre-post studies without true controls. One representative study by Agarwala et al. found an improvement in critical information transfer and retention with introduction of an electronic handoff checklist.11 Similarly, Boat et al. utilized quality improvement (QI) methodology to implement an intraoperative checklist, finding improved reliability of attending anesthesiologist handoffs at a pediatric hospital.12 A recent interventional cohort study by Jullia et al. did make use of a geographically distinct control group and found that development, training, and display of a laminated checklist for intraoperative handoffs improved the observed quality of handoffs by 43% as compared to the control group.13 Though evidence does not currently exist about the impact that these interventions may have on postoperative outcomes, it appears likely that structure and standardization can at least improve the transfer of information for intraoperative handoffs.
Duty relief. Only two studies have examined duty relief, Cooper et al. in 19824 and Terekhov et al. in 2016.10 Interestingly, both found an association between duty relief and improved patient outcomes. In the 1982 study by Cooper and colleagues of more than 1,000 critical incidents during anesthesia care, 28 of 96 total incidents associated with intraoperative relief were identified as favorable, where the introduction of the relief anesthetist led to the discovery of an error or other failure to provide optimal care. Only 10 incidents were identified as unfavorable, where some aspect of the relief process was identified as contributing to the cause of the incident.4 In a subsequent paper further discussing the merits of short breaks in an era where there was debate about the appropriateness of anesthesia professional relief, Cooper concluded “relief is probably better than no relief… relief that is not conducted safely is probably worse than no relief.”5 In Terekhov’s 2016 retrospective study of more than 140,000 cases at a large academic medical center, the total number of intraoperative handoffs was not found to be associated with postoperative adverse outcomes, but short breaks were associated with a 6.7% decrease in adverse outcomes.10 There is at least some evidence to support the common practice of giving multiple short breaks over the course of a clinical day, whether those breaks are often provided by experienced providers with fresh eyes, or that the ability to give breaks is associated with having enough staff to assist with crises.
Transitions in Care
Studies addressing care transitions tend to focus on one of two handoff types: postoperative handoffs from OR-to-PACU12,14 or from OR-to-ICU.15-17 These handoffs are similar in that they involve patient movement between sites of care, interprofessional communication, and participation of multiple care team members. In contrast to most published intraoperative handoff research, transitions studies tend to be interventional. The intervention is almost always handoff standardization of some type, specifying which clinicians should be involved and scripting communication with a checklist or template. Randomization is uncommon in these studies, perhaps owing to the difficulty in randomizing clinician behavior without contamination or spillover to other settings. To our knowledge, all the published transitions studies have shown standardization-related improvements in process outcomes such as information exchange; a handful of studies have suggested improvements in short-term patient outcomes.18,19
While there are dozens of studies now published relating to perioperative handoffs, the strength of the evidence can at best be called intermediate. Among the many limitations of the existing literature, some of the challenges include the preponderance of single-center studies, most with pre-post designs and without controls, the presence of the Hawthorne effect (i.e., the phenomenon in which behavior changes because it is being observed), and the lack of information about handoff intervention sustainability. There is limited evidence about how best to implement handoff improvement interventions. Perhaps most importantly, there is very little evidence supporting a clean link between handoff process outcomes and patient outcomes.
Nonetheless, several published papers about perioperative handoffs suggest that these handoffs are associated with patient outcomes, including adverse events, major morbidity, and mortality. While causality cannot be claimed, there are several handoff process elements and behaviors that are common across the majority of published studies showing improvement in process or patient outcomes.
Evidence for Specific Process Elements and Behaviors
Much of the early literature on perioperative handoff interventions has focused on the pediatric cardiac population. Catchpole and colleagues described development of a comprehensive handoff protocol for pediatric cardiac patients transferred to the ICU, using lessons learned from Formula 1 pit-stop crews.16 They used pre-handoff information transfer and explicitly separated equipment and technology transfer from information transfer. They also mandated a group discussion supported by a cognitive aid between the surgeon, anesthesia professional, and receiving team that included information about the surgical case, anticipated problems, and anticipated recovery plans. Technical errors fell by 42%, and information omissions fell by 49%.16 Joy and colleagues described implementation of a comprehensive handoff improvement intervention using QI methodology in a pediatric cardiac ICU.15 The intervention was a standardized template for oral handoff presentation, along with iterative testing of the tool, education, and training. The investigators found a 75% reduction in technical errors and a 62% reduction in critical information omissions.15 Other studies in the pediatric cardiac population have used similar strategies, utilizing cognitive aids, separating equipment transfer from verbal handoff, and calling attention to the importance of the receiving team verbalizing understanding and having the opportunity to ask questions.17,18 A 2012 systematic review of the published literature identified and summarized many of the common strategies employed in various studies (Figure 2).2,20
| Figure 2. Common handoff strategies employed in perioperative handoffs and in other high-stakes industries, as reported by Segall et al.2 and Patterson et al.20 | |
| • | Receiver preparation of monitors and equipment prior to patient arrival |
| • | Completion of urgent tasks prior to verbal handoff |
| • | Delay of transfer of responsibility during critical activities |
| • | Limitation of distractions and interruptions |
| • | Presence of all relevant team members |
| • | Use of face-to-face, two-way communication |
| • | Use of protocols to standardize processes |
| • | Use of structured checklists to guide complete information transfer |
| • | Receiver routinely reviewing pertinent data prior to handoff |
| • | Ensuring that giver has adequate knowledge about previous shift activities |
| • | Use of supporting documentation to assist with information transfer (e.g., labs, anesthesia chart) |
| • | Opportunity for questions and concerns |
| • | Use of closed-loop communication with read-back of critical information |
| • | Formal team or handoff training |
The evidence base for intraoperative shift-change handoffs is more limited. Two different studies on intraoperative handoffs by Boat12 and Agarwala11 both introduced checklists using QI methodology to assist with information transfer between providers at the end of shift, with inclusion of not only patient factors, but post-op plan and disposition. The Agarwala study also included items on the checklist for specific action steps (e.g., redosing antibiotics), as well as a reminder to introduce the incoming anesthesia professional to the OR team.
Can Anything Be Learned From Other High-Risk Industries?
The importance of the transition of responsibility from one team to another is not unique to the care of surgical patients, nor is it unique to the practice of medicine. In 2004, Patterson and colleagues used direct observation to analyze handoffs in several high-stakes industries where highly reliable information transfer is critical, including space shuttle mission control, nuclear power plants, a railroad dispatch center, and an ambulance dispatch center.20 Several strategies were identified as common across multiple settings, including the use of face-to-face, two-way communication with interactive questioning, limiting of interruptions and distractions, the delay of transfer of responsibility during critical activities, the receiver routinely reviewing pertinent data prior to handoff, the giver having adequate knowledge about previous shift activities, and the unambiguous transfer of responsibility.20 As a routine part of their training, air traffic controllers are taught to use closed-loop communication, with read back of critical information.
Many of these strategies have been used in the published studies on health care handoffs with good reason, as medicine is highly specialized with complex technology and potentially severe consequences for system failure, with responsibility for successful management spread amongst a team of people, as compared to a single individual. The similarities between medicine and other high-stakes environments may explain why handoff standardization has been embraced, despite the lack of “gold standard” evidence from randomized controlled trials. Most notably, the multicenter I-PASS study demonstrated a roughly 25% decrease in preventable adverse events after introduction of a comprehensive handoff standardization program for pediatric residents.21
A Checklist Is Not Enough
Over time, there are fewer studies that question whether handoffs should be standardized. Instead, studies question how to standardize, how much to standardize, and how to standardize handoffs in a way that complements clinician workflow instead of interfering with it. Indeed, standardization is at the core of all the interventional strategies described in the literature to decrease the potential harm from perioperative shift changes and transitions in care. Standardization, however, is not synonymous with the introduction of a checklist.
Checklists address only one function of handoffs—information exchange. Successful handoff standardization interventions not only include checklists or templates, but they also create expectations of clinician involvement, and they specify the ideal conditions for handoffs to occur. They also account for the complex nature of perioperative care, breaking up the handoff process into a series of non-overlapping steps to avoid distractions and threats to attention. In this way, clinicians are able to give their undivided attention to the handoff for a short period of time, improving the reliability of the process.
*The cited studies do not represent all published work on perioperative handoffs. More complete lists of references are available in two published handoff reviews.2,22 Click for Enlarged view
Moving Forward
While there is evidence supporting perioperative handoff standardization, there are at least two largely unaddressed aspects of perioperative handoffs. First, we do not know which standardization strategies are most useful. Published studies to date have compared one standardized process to the lack of a process, but have not compared two or more standardization strategies to each other. Second, we know very little about the implementation strategies that are effective in adopting and adhering to standardized handoffs. Clearly, there can be no true improvement in patient outcomes, even with the best standardized process, if the process is not adopted and durably followed by the clinicians responsible for patient care. For this reason, future studies require attention to implementation strategy. Implementation strategies that might be tested include customizing standardized handoffs to local clinicians’ needs, developing leadership buy-in, stakeholder engagement and involvement in intervention development, education and training, champion identification, iterative adaptation, auditing, and ideally, feedback to clinicians.
Overall, there is growing interest in handoffs amongst clinicians, QI leaders, and researchers. This attention is more than 35 years in the making,4 but is certainly in keeping with our specialty’s reputation as a leader in patient safety.
Dr. Agarwala is Division Chief, General Surgery Anesthesia and Associate Director, Anesthesia Quality and Safety at the Massachusetts General Hospital.
Dr. Lane-Fall is Assistant Professor of Anesthesiology and Critical Care at the Perelman School of Medicine of the University of Pennsylvania. She is Co-Director of the Penn Center for Perioperative Outcomes Research and Transformation and Assistant Director of the Penn Center for Healthcare Improvement and Patient Safety.
Neither author has any conflicts of interest to disclose.
References
- Lane-Fall MB, Brooks AK, Wilkins SA, et al. Addressing the mandate for hand-off education: A focused review and recommendations for anesthesia resident curriculum development and evaluation. Anesthesiology 2014;120:218–229a.
- Segall N, Bonifacio AS, Schroeder RA, et al. Can we make postoperative patient handovers safer? A systematic review of the literature. Anesth Analg 2012;115:102–115.
- Cooper JB, Newbower RS, Long CD, McPeek B. Preventable anesthesia mishaps: A study of human factors. Anesthesiology 1978;49:399–406.
- Cooper JB, Long CD, Newbower RS, Philip JH. Critical incidents associated with intraoperative exchanges of anesthesia personnel. Anesthesiology 1982;56:456–461.
- Cooper JB. Do short breaks increase or decrease anesthetic risk? Journal of Clinical Anesthesia 1989;1:228–231.
- Arbous MS, Meursing AEE, Van Kleef JW, et al. Impact of anesthesia management characteristics on severe morbidity and mortality. Anesthesiology 2005;102:257–268.
- Saager L, Hesler BD, You J, et al. Intraoperative transitions of anesthesia care and postoperative adverse outcomes. Anesthesiology 2014;121:695–706.
- Hyder JA, Bohman JK, Kor DJ, et al. Anesthesia care transitions and risk of postoperative complications. Anesth Analg 2016;122:134–144.
- Hudson CC, McDonald B, Hudson JK, et al. Impact of anesthetic handover on mortality and morbidity in cardiac surgery: A cohort study. J Cardiothor Vasc An 2015;29:11–16.
- Terekhov MA, Ehrenfeld JM, Dutton RP, et al. Intraoperative care transitions are not associated with postoperative adverse outcomes. Anesthesiology 2016;125:690–699.
- Agarwala AV, Firth PG, Albrecht MA, et al. An electronic checklist improves transfer and retention of critical information at intraoperative handoff of care. Anesth Analg 2015;120:96–104.
- Boat AC, Spaeth JP. Handoff checklists improve the reliability of patient handoffs in the operating room and postanesthesia care unit. Paediatric Anaesthesia 2013;23:647–654.
- Jullia M, Tronet A, Fraumar F, et al. Training in intraoperative handover and display of a checklist improve communication during transfer of care. EJA 2017;34:471–476.
- Weinger MB, Slagle JM, Kuntz AH, et al. A multimodal intervention improves postanesthesia care unit handovers. Anesth Analg 2015;121:957–971.
- Joy BF, Elliott E, Hardy C, et al. Standardized multidisciplinary protocol improves handover of cardiac surgery patients to the intensive care unit. Pediatric Critical Care Medicine 2011;12:304–308.
- Catchpole KR, De Leval MR, McEwan A, et al. Patient handover from surgery to intensive care: using Formula 1 pit-stop and aviation models to improve safety and quality. Paediatric Anaesthesia 2007;17:470–478.
- Craig R, Moxey L, Young D, et al. Strengthening handover communication in pediatric cardiac intensive care. Paediatric Anaesthesia 2012;22:393–399.
- Agarwal HS, Saville BR, Slayton JM, et al. Standardized postoperative handover process improves outcomes in the intensive care unit: A model for operational sustainability and improved team performance. Critical Care Medicine 2012;40:2109–2115.
- Kaufman J, Twite M, Barrett C, et al. A handoff protocol from the cardiovascular operating room to cardiac icu is associated with improvements in care beyond the immediate postoperative period. Joint Commission Journal on Quality and Patient Safety 2013;39: 306–311.
- Patterson ES, Roth EM, Woods DD, et al. Handoff strategies in settings with high consequences for failure: lessons for health care operations. International Journal for Quality in Health Care 2004;16:125–132.
- Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. NEJM 2014;371:1803–1812.
- Keebler JR, Lazzara EH, Patzer BS, et al. Meta-Analyses of the effects of standardized handoff protocols on patient, provider, and organizational outcomes. Human Factors: The Journal of the Human Factors and Ergonomics Society. November, 2016.
