The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or group responses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intention of APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
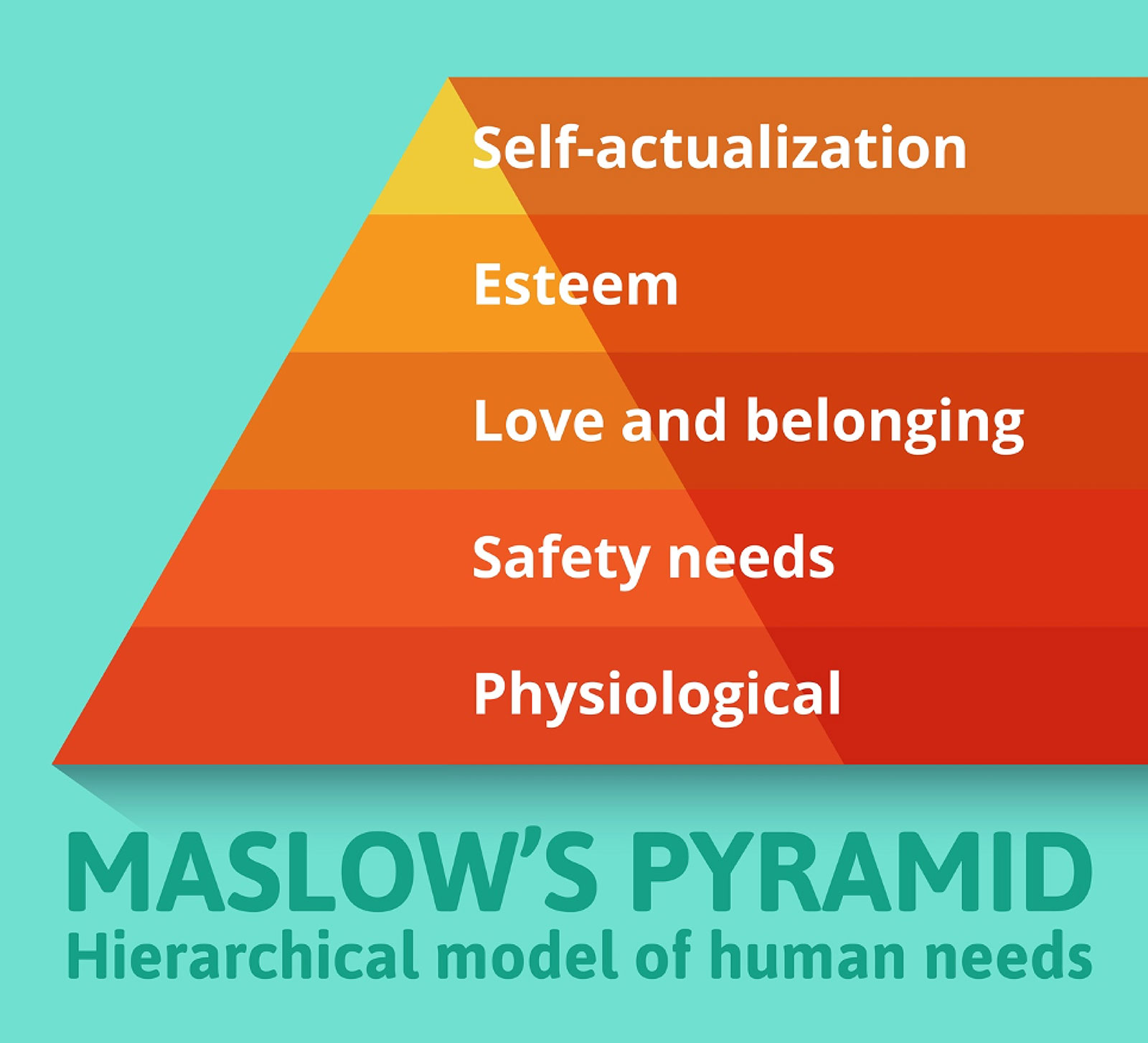
Figure 1: Maslow’s Hierarchical Model of Human Needs.
Clinician well-being has come to the forefront of discussions of not only health care worker satisfaction, but also sustainability of the health care industry. These discussions are occurring at every level, from the work of the National Academy of Medicine’s Action Collaborative on Clinician Well-Being and Resilience to sessions at society meetings, hospital well-being committees, lay press, and social media. What has become clearer with every dataset published is that systems-based solutions ought to be the focus for the clinician burnout and disengagement crisis we are currently in.1 With the impending worsening of workforce shortages anticipated within the coming years, this will be increasingly more important.2 Accordingly, many national organizations, including professional societies, have been collaborating for several years now to meet the challenge head-on and answer the question: What role can professional societies play in clinician well-being?
At the 2021 APSF Stoelting Conference, I had the opportunity to present the experience of the American Society of Anesthesiologists (ASA) and how we are approaching clinician well-being. The Committee on Physician Well-Being (COPWB) was established in 2019 just prior to the COVID-19 pandemic, but this came after years of engagement from a large number of anesthesiologists interested in various aspects of well-being. When the committee formed, in an effort to maintain the engagement of as many interested people as possible, four working groups were established to conduct the work of the committee: The Working Group on Systems & Policy That Impact Well-Being, Working Group on Education & Endeavors, Working Group on Clinician Mental Health & Suicide Prevention, and the Working Group on ASA Outreach. While Committee membership is by application only, any ASA member may participate in the Working Groups. We also made the decision to make the ASA Well-Being webpage publicly facing since many of the challenges faced are not unique to physicians and resources often serve all members of the health care team. The COPWB also endorsed a survey study to assess the state of burnout in U.S. attending anesthesiologists, focusing on potentially actionable demographic and practice-based factors. This survey study was scheduled to be distributed during the first week of March 2020.
Recently, this study of burnout in anesthesiologists was published with nearly 4,000 respondents.3 Using the Maslach Burnout Inventory, which assesses occupational burnout across the three domains of emotional exhaustion, depersonalization, and a low sense of personal accomplishment, the authors assessed both high risk for burnout (reaching threshold levels of emotional exhaustion or depersonalization), and burnout syndrome (simultaneously reaching threshold levels of emotional exhaustion, depersonalization and a low sense of personal accomplishment). The findings, representing the state of affairs prior to the peak of the COVID-19 pandemic (survey responses mostly from the first half of March, 2020), demonstrated 59% of US attending anesthesiologists were at high risk for burnout and nearly 14% had the burnout syndrome. While the incidence data are important, the associations between burnout and various demographic and practice-based factors is also informative. Primarily, the response to the question, “How supported do you feel in your work-life?” was significantly associated with burnout. If one espoused little to no support in their work-life, they had an adjusted odds ratio of 6.7 for being at high risk for burnout and an odds ratio of 10 for burnout syndrome. This information has bolstered the COPWB’s commitment to focus on an end-goal of promoting a culture of well-being and support within our workplaces, as described below.
The working groups had just begun to tackle their respective agendas when the COVID-19 pandemic hit in full force; it became quickly apparent that the pandemic-associated experiences, stressors, and imbalances were very heterogeneous and many people raised concerns about the experiences of women and others underrepresented in medicine (e.g., racial and ethnic minority individuals). In response to this, the ASA established an ad hoc Committee on Systemic Life Imbalances, charged with assessing the unequal burdens shouldered by many within our ranks and how groups and departments could address those differential challenges.
As discussions began, it was immediately evident that not only were these imbalances entrenched long before COVID-19, but they represented a challenge that only sweeping organizational culture change could adequately address.
One of the first work-products from the Committee on Physician Well-being was a brief “one-pager” resource on “Creating a Culture of Well-being for Healthcare Workers,” which can be downloaded from the ASA Well-being website. This document approaches workplace culture by addressing the need to satisfy higher levels of Maslow’s Hierarchy of needs (Figure 1), starting with our most basic survival needs, then rising to the higher-level needs attached to a sense of meaning and purpose. The approach is structured not by the outdated and traditional “command and control” rubric of organizational leadership, but instead by robust and open two-way communication, free from fear of retribution, and reinforced by accountability and enhanced communication from leadership. Such a workplace culture would foster collaboration among all stakeholders within the organization, ultimately building stronger, more inclusive teams.
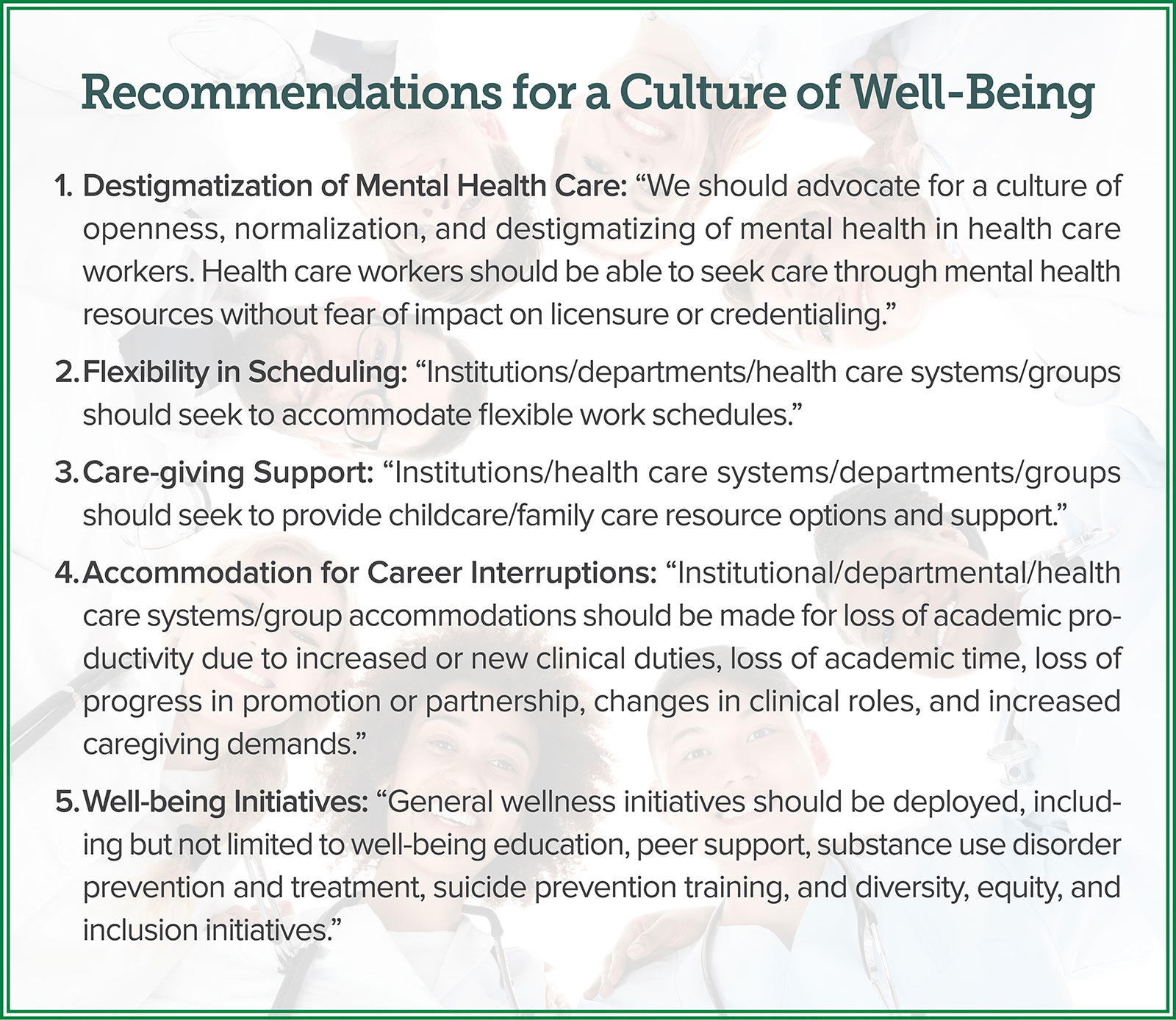
This “one-pager” served as a rational starting point for addressing the diversity of needs within our anesthesia workforce. In a joint statement between the ad hoc Committee on Systemic Life Imbalances and the Committee on Physician Well-being, the “ASA Statement on Creating Cultures of Well-being for Healthcare Workers” was proposed as a resolution and approved by the ASA House of Delegates at the 2021 ASA Annual Meeting in October. This statement advocates for a five-point approach to transforming work culture and is supported by four well-sourced documents providing more granular and pragmatic detail to the recommendations.
The approach is somewhat intuitive in terms of its approach to a balanced work and home life, but also considers pandemic-specific interruptions to various career trajectories. Many of these may seem particularly daunting given current staffing shortages, but nonetheless represent recommended goals as rebuilding occurs. The recommendations are as follows (where italicized, amended to be inclusive of all health care workers) and are available at https://www.asahq.org/standards-and-guidelines/asa-statement-on-creating-a-culture-of-well-being-for-health-care-workers:
Our intention is for these recommendations to serve as a framework for workplace improvements, ultimately leading to an improved culture of support for our broader workforce. The challenges faced by anesthesiologists are not unique to them, and we encourage all professional societies to develop and adopt similar strategies if they have not already done so. Collaborations among professional societies, representing varying perspectives, can only serve to strengthen our collective response to health care worker needs.
To say that the COVID-19 pandemic shifted the ways in which we think about many aspects of life would be an understatement. Many of the things we felt we had to do a certain way were simply done a different way for over a year. While disruptive, this also established a creative mindset. Coupled with a broad openness to discussing aspects of work-life integration, mental health, and well-being, this creative mindset represents an opportunity to transform work culture in a way not previously believed feasible. Put simply—the cracks have been revealed—we can choose to pave over and ignore the faults in our system, or we can work to repair them and build back stronger than ever imagined.
Amy E. Vinson, MD, FAAP, is an assistant professor of Anaesthesia, Harvard Medical School, senior associate in Perioperative Anesthesiology, Boston Children’s Hospital, director of Clinician Well-Being, Department of Anesthesiology, Critical Care & Pain Medicine, and chair, American Society of Anesthesiologists Committee on Physician Well-Being.
The author has no conflicts of interest.
References
- National Academy of Medicine, National Academies of Sciences, Engineering and Medicine. Taking action against clinician burnout: a systems approach to professional well-being. The National Academies Press; 2019. doi.org/10.17226/25521
- Oslock WM, Satiani B, Way DP, et al. A contemporary reassessment of the US surgical workforce through 2050 predicts continued shortages and increased productivity demands. Am J Surg. 2021;223:28–35. Published online 2021. doi.org/10.1016/j.amjsurg.2021.07.033
- Afonso AM, Cadwell JB, Staffa SJ, Zurakowski D, Vinson AE. Burnout rate and risk factors among anesthesiologists in the United States. Anesthesiology. 2021;134:683–696. doi.org/10.1097/aln.0000000000003722
