 Foreign body ingestions are common events among pediatric patients. Button battery ingestions are particularly dangerous. Although the incidence of button battery ingestions has not changed over the last 30 years,1 the rates of emergency department visits, major morbidity, and mortality have risen dramatically since the introduction of the 3-volt–20 mm lithium batteries in 2006.1-3 These batteries are larger and more powerful than their predecessors, which has increased the incidence of esophageal impaction and significant tissue injury.2 The overall incidence of major morbidity or mortality after button battery ingestion is 0.42%.1 However, in children under six years old who ingest batteries >20 mm, the rates of major complications are as high as 12.6%.2 All reported fatalities have occurred in children under five years old.4
Foreign body ingestions are common events among pediatric patients. Button battery ingestions are particularly dangerous. Although the incidence of button battery ingestions has not changed over the last 30 years,1 the rates of emergency department visits, major morbidity, and mortality have risen dramatically since the introduction of the 3-volt–20 mm lithium batteries in 2006.1-3 These batteries are larger and more powerful than their predecessors, which has increased the incidence of esophageal impaction and significant tissue injury.2 The overall incidence of major morbidity or mortality after button battery ingestion is 0.42%.1 However, in children under six years old who ingest batteries >20 mm, the rates of major complications are as high as 12.6%.2 All reported fatalities have occurred in children under five years old.4
The primary mechanism of injury is the generation of electrolytic current that hydrolyzes tissue fluids and produces hydroxide ions at the battery’s negative pole.2 This creates a highly alkaline environment that raises the local tissue pH up to 12 or 13, leading to liquefactive necrosis of adjacent tissues. They may also cause perforation and erosion into adjacent structures, including the airway, vasculature, mediastinal structures, or spinal cord. Most of the 67 fatalities reported to the National Capital Poison Center are due to hemorrhage from esophageal-vascular fistulae or complications of tracheoesophageal fistulae.4 The development of an aorto-esophageal fistula is an ominous finding, as there are only four reported cases of survival in the literature.5-8
Given the potential for significant morbidity and mortality, it is imperative to rapidly triage and manage patients who present with a confirmed or suspected button battery ingestion. Perioperative management guidelines, risk factors for significant injury, and new preoperative mitigation strategies are of particular importance for anesthesia professionals. The damage caused by button batteries is determined by the location and duration of impaction, as well as the orientation, size, and voltage of the button battery.9,10 Esophageal battery impactions prolong contact between the battery and esophageal tissue, increasing the risk of damage. Tissue damage begins to develop within 15 minutes of contact with a button battery, and the risk of severe injury increases with the duration of button battery exposure.11 Compromised tissues may continue to have progressive liquefactive necrosis for days to weeks after button battery removal.12 Due to these issues, the button battery must be removed via endoscopy emergently, preferably within 2 hours of ingestion, and the patient must be monitored postoperatively for signs of progressive injury.12
Unfortunately, foreign body ingestions in children are frequently unwitnessed, and the symptoms may easily be incorrectly attributed to respiratory or gastrointestinal illnesses, which significantly delays diagnosis.13 Therefore, a high index of clinical suspicion is necessary. In addition, many parents and health care providers are unaware of the dangers of button battery ingestion and may not seek emergency treatment.14 Even if the patient is promptly brought for medical care, the medical facility may not have the pediatric specialists and equipment required to manage the patient, including emergency physicians, otolaryngologists, gastroenterologists, general or cardiothoracic surgeons, and anesthesia professionals. If transfer to another facility is required, the battery removal will be further delayed.
Standardized protocols for the triage and management of patients with suspected button battery ingestion have been published by multiple groups.9,10,15,16 The goal of these guidelines is to identify high-risk patients and streamline the process of removing the button battery. Comprehensive management guidelines from the National Capital Poison Center can be found at www.poison.org/battery/guideline. The initial evaluation should include x-rays of the neck, chest, and abdomen to locate and identify the ingested object. Any foreign body impacted in the esophagus, symptomatic gastric button batteries, and batteries that are co-ingested with a magnet must be immediately removed. A conservative management approach may be taken if the child is >12 years old, asymptomatic, with no history of esophageal pathology, and with a known ingestion of a single battery < 12 mm diameter without other foreign bodies.
Table 1: Risk Stratification for Button Battery Ingestions in Children9
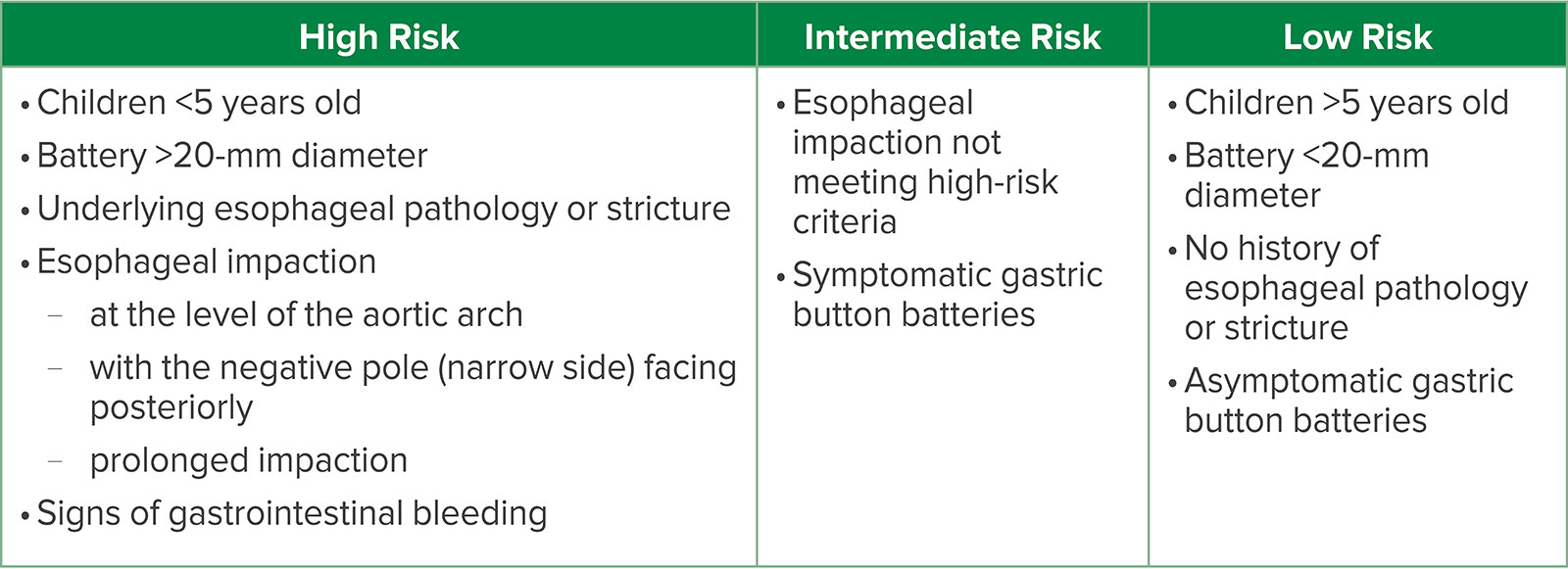
Once the decision is made to proceed with removal, a risk assessment must be performed (Table 1). Esophageal impactions are most likely to occur in young children (<5 years old), patients with underlying esophageal pathology or stricture, and after ingestion of larger batteries (>20 mm diameter). In addition, impaction at the level of the aortic arch, particularly with the negative pole (narrow side) of the battery facing posteriorly, increases the risk of vascular injury. Any sign of gastrointestinal bleeding is ominous and signals a potential vascular-esophageal fistula. Patients meeting any of these criteria are considered high risk. Those with an esophageal impaction not meeting the above criteria or a symptomatic gastric battery are deemed intermediate risk. Finally, asymptomatic patients and/or ingestion of small gastric batteries (<20 mm) in older children (>5 years old) with no history of esophageal pathology are low risk.9
Intermediate- and low-risk patients may be cared for in a general operating room by gastroenterologists with or without general surgeons on standby. For patients at high risk, consideration should be given to involving interventional cardiologists or cardiothoracic surgeons. They may require more invasive vascular access, hemodynamic monitoring, volume resuscitation, and blood product administration.
Detailed discussions of the anesthetic management and postoperative monitoring required for these patients have been described in other publications.9,10 The airway should be secured by rapid sequence induction. The team must be prepared for hemodynamic and/or respiratory instability around the time of battery removal, particularly if the battery has caused vascular or airway injury. After battery removal, a repeat endoscopy and bronchoscopy are performed to assess the esophagus and airway for injury.
Postoperatively, the patient must be monitored for progressive injury to the esophagus and surrounding tissues. The duration and acuity level of inpatient care depends on the initial injury seen during battery removal. Repeated anesthetics may be required for serial imaging studies and/or endoscopic evaluation.
Due to the potential for delayed button battery removal and ongoing tissue damage, several mitigation strategies have been investigated. Button batteries create an alkaline environment that ultimately leads to mucosal damage and liquefactive necrosis.12,17 Studies in cadaveric and live piglet models have demonstrated that irrigation with weakly acidic solutions prior to battery removal neutralizes the alkaline environment and decreases tissue damage compared to irrigation with saline.17,18 These solutions include common household beverages (juice, soda, and sports drinks) as well as viscous solutions (honey and syrup), which are safe for a child to ingest. Honey and sucralfate most effectively neutralize the alkaline environment created by the button battery. They are also associated with less extensive tissue damage and decreased rates of delayed esophageal perforation compared to saline irrigation.18 Both solutions are weakly acidic and form a viscous physical barrier between the battery and the tissue. In a separate study, irrigation with 0.25% acetic acid solution after button battery removal neutralized the pH of the esophageal tissue, which may also decrease the progression of tissue injury and delayed complications seen after button battery removal.17
Based on these studies, the management guidelines from the National Capital Poison Control Center now include recommendations to mitigate tissue injury prior to and after button battery removal.15 Honey and/or sucralfate should be administered orally (10 mL every 10 minutes) from the time of ingestion until button battery removal. Due to concerns for botulism in infants, patients <12 months old should not be given honey. Nothing should be administered orally if it has been >12 hours since battery ingestion or if there are concerns for esophageal perforation, mediastinitis, or sepsis. No other medications, fluids, or foods should be administered orally, and vomiting should not be induced as the dislodged battery may be aspirated and vomiting may cause or worsen esophageal perforation.
It is critical to note that while these interventions mitigate injury, the battery must still be emergently removed. Parents must proceed to the emergency department immediately, and removal must not be delayed due to the patient’s oral intake. After the battery is removed and there is no evidence of perforation, the esophagus may be irrigated with 0.25% acetic acid solution (50–150mL) to neutralize residual alkaline substances.
In conclusion, the dangers of button battery ingestions and the need for emergent battery removal are underappreciated by many parents and medical providers. Further, many clinicians are unaware of the current recommendations for mitigation strategies, and anesthesia professionals may inappropriately delay cases for patients who have recently ingested honey or sucralfate.14 Our group at Children’s Hospital Colorado created infographics for both parents (Image 1a) and anesthesia professionals (Image 1b) to address these issues. It is our hope that these infographics can be displayed in a variety of settings, such as in medical offices, on medical websites geared toward parents, and in medical journals, to help increase awareness of these recommendations. These infographics can be accessed on the Society for Pediatric Anesthesia website (www.pedsanesthesia.org). Although primary prevention of ingestion is the ultimate management goal, it is also important to publicize treatment guidelines to help decrease the serious and potentially fatal outcomes seen after button battery ingestions.
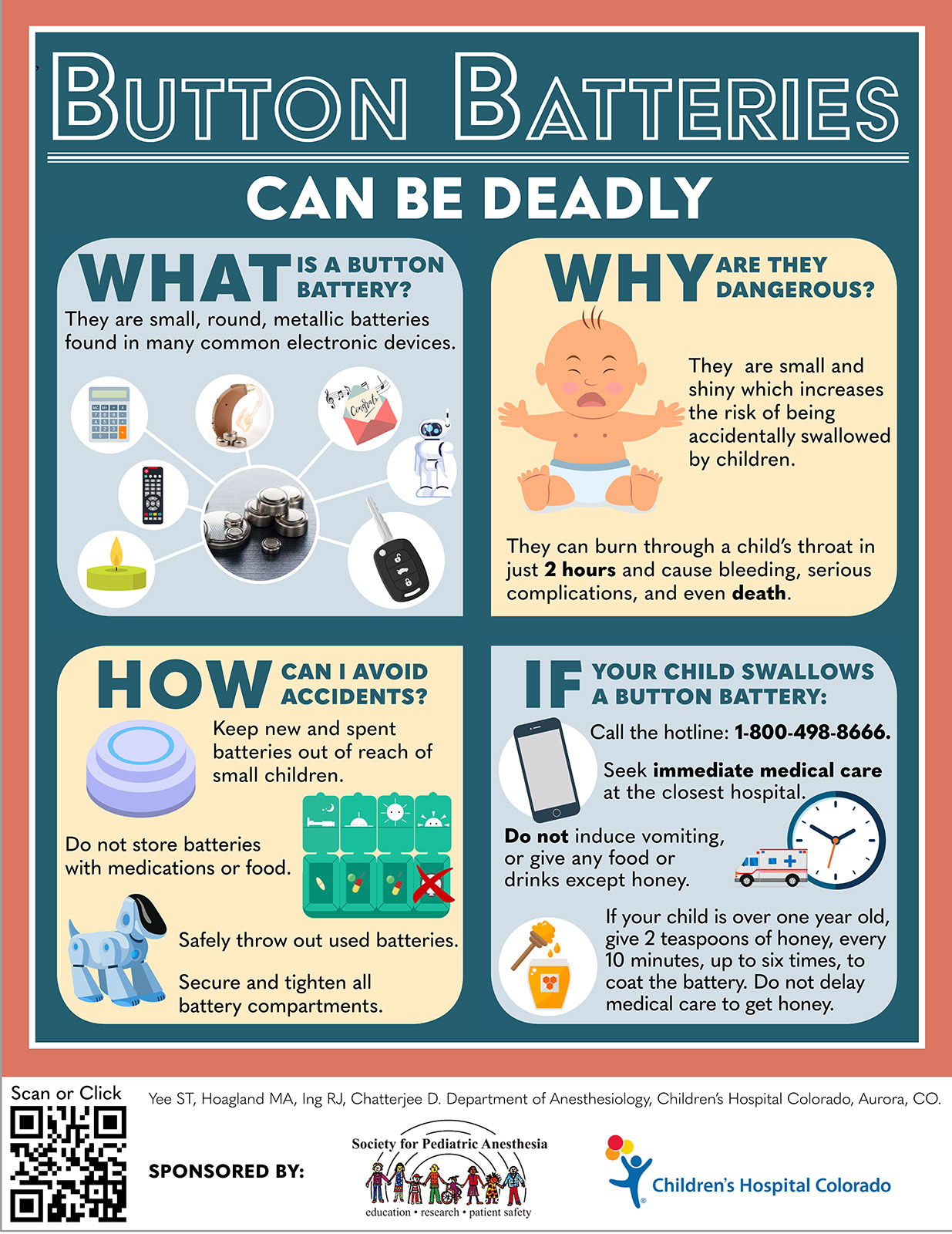
Figure 1a: Infographic describing the management of button battery ingestions for parents. Used with permission obtained by authors.
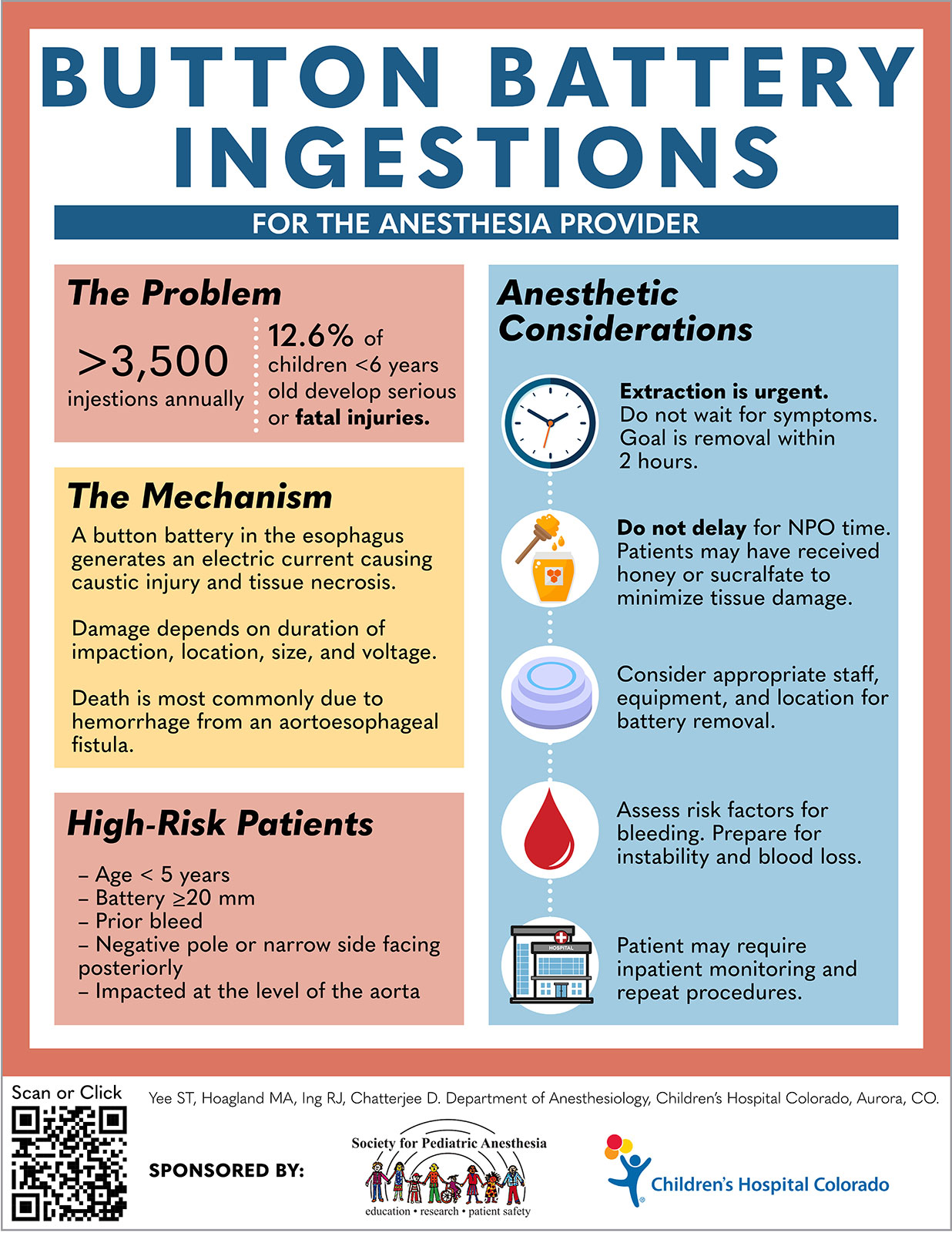
Figure 1b: Infographic describing the management of button battery ingestions for anesthesia providers. Used with permission obtained by authors.
Monica Hoagland, MD, is an associate professor of anesthesiology at Children’s Hospital Colorado, University of Colorado School of Medicine, Aurora, CO.
Sydney Lee, MD, is a pediatric anesthesiology fellow at Children’s Hospital Colorado, University of Colorado School of Medicine, Aurora, CO.
Richard Ing, MBBCh, FCA (SA), is a professor of anesthesiology at Children’s Hospital Colorado, University of Colorado School of Medicine, Aurora, CO.
Debnath Chatterjee, MD, FAAP, is an associate professor of anesthesiology at Children’s Hospital Colorado, University of Colorado School of Medicine, Aurora, CO.
The authors have no conflicts of interest.
References
- National Capital Poison Center. Button battery ingestion statistics. Available at: https://poison.org/battery/stats. Accessed July 12.2021
- Litovitz T, Whitaker N, Clark L, et al. Emerging battery-ingestion hazard: clinical implications. Pediatrics. 2010;125:1168–1177.
- Sharpe SJ, Rochette LM, Smith GA. Pediatric battery-related emergency department visits in the United States, 1990–2009. Pediatrics. 2012;129:1111–1117.
- National Capital Poison Center. Fatal button battery ingestions: 67 reported cases. Available at: https://poison.org/battery/fatalcases. Accessed July 12, 2021.
- Spiers A, Jamil S, Whan E, et al. Survival of patient after aorto-oesophageal fistula following button battery ingestion. ANZ J Surg. 2012;82:186–187.
- Mahajan S, Jaswal V, Thingnam SKS, Dogra N. Successful surgical management of an aorto-oesophageal fistula caused by button battery ingestion. Eur J Cardiothorac Surg. 2019;55:790–791.
- Wakimoto M, Willer BL, McKee C, et al. Successful management of an aorto-esophageal fistula following button battery ingestion: a case report and review of the literature. Saudi J Anaesth. 2021;15:193–198.
- Sinclair EM, Stevens JP, McElhanon B, et al. Development and repair of aorto-esophageal fistula following esophageal button battery impaction: a case report. J Pediatr Surg Case Rep. 2021;66.
- Hoagland MA, Ing RJ, Jatana KR, et al. Anesthetic implications of the new guidelines for button battery ingestion in children. Anesth Analg. 2020;130:665–672.
- Eck JB, Ames WA. Anesthetic implications of button battery ingestion in children. Anesthesiology. 2020;132:917–924.
- Tanaka J, Yamashita M, Yamashita M, Kajigaya H. Esophageal electrochemical burns due to button type lithium batteries in dogs. Vet Hum Toxicol. 1998;40:193–196.
- Jatana KR, Litovitz T, Reilly JS, et al. Pediatric button battery injuries: 2013 task force update. Int J Pediatr Otorhinolaryngol. 2013;77:1392–1399.
- Buttazzoni E, Gregori D, Paoli B, et al. Symptoms associated with button batteries injuries in children: an epidemiological review. Int J Pediatr Otorhinolaryngol. 2015;79:2200–2207.
- Cairns R, Brown JA, Lachireddy K, et al. Button battery exposures in Australian children: a prospective observational study highlighting the role of poisons information centres. Clin Toxicol. (Phila). 2019;57:404–410.
- National Capital Poison Center button battery ingestion triage and treatment guidelines. https://poison.org/battery/guideline. Accessed July 12, 2021.
- Sethia R, Gibbs H, Jacobs IN, et al. Current management of button battery injuries. Laryngoscope Investig Otolaryngol. 2021;6:549–563.
- Jatana KR, Rhoades K, Milkovich S, Jacobs IN. Basic mechanism of button battery ingestion injuries and novel mitigation strategies after diagnosis and removal. Laryngoscope. 2017;127:1276–1282.
- Anfang RR, Jatana KR, Linn RL, Rhoades K, Fry J, Jacobs IN. pH-neutralizing esophageal irrigations as a novel mitigation strategy for button battery injury. Laryngoscope. 2019;129:49–57.
