The article discusses the advancements of the laryngeal mask airway (LMA) and its routine and non-routine uses. It analyzes the risk of aspiration with the LMA compared with the endotracheal tube. It also reviews whether mechanical ventilation is safe with the new generation of LMAs.
The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or group responses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intention of APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
Introduction
The laryngeal mask airway (LMA) was invented in 1983 by Archie Brain, MD, as an alternative airway device to the facemask and endotracheal tube (ETT).1 Since the establishment of the classical LMA, the device has undergone multiple improvements and modifications (Table 1). The LMA can provide a better quality of ventilation over a mask alone and with less instrumentation to the airway than tracheal intubation.2 Advantages of the LMA include the ease of use and less injury to airway tissues than ETTs, although trauma can result from forceful use of LMAs.3-6 With the LMA, there are fewer hemodynamic disturbances and postoperative complications than with an ETT.2 The LMA has been widely used in surgery requiring general anesthesia and as a rescue device for difficult airways.7 In the updated difficult airway algorithm, developed by the American Society of Anesthesiologists, the LMA is a priority apparatus for emergency noninvasive airway access.7 Many clinical investigations and much research have demonstrated that the LMA is a safe and reliable airway device.2,6,8,9 However, debate continues regarding nonstandardized use of the LMA in clinical settings, including with positive pressure ventilation (PPV) and muscle relaxants, in laparoscopic surgery, and with obese patients (Table 2). Concerns regarding LMA use can be categorized as follows: (1) inadequate seal of the LMA due to malposition; (2) airway injuries ranging from throat discomfort to permanent tissue damage; (3) aspiration risk; (4) safety of mechanical ventilation as opposed to spontaneous ventilation; and (5) safety in obese patients. Nonroutine uses of the LMA and potential safety issues will be discussed in this review.
Table 1: Evolution of the Laryngeal Mask Airway (LMA)1, 6, *
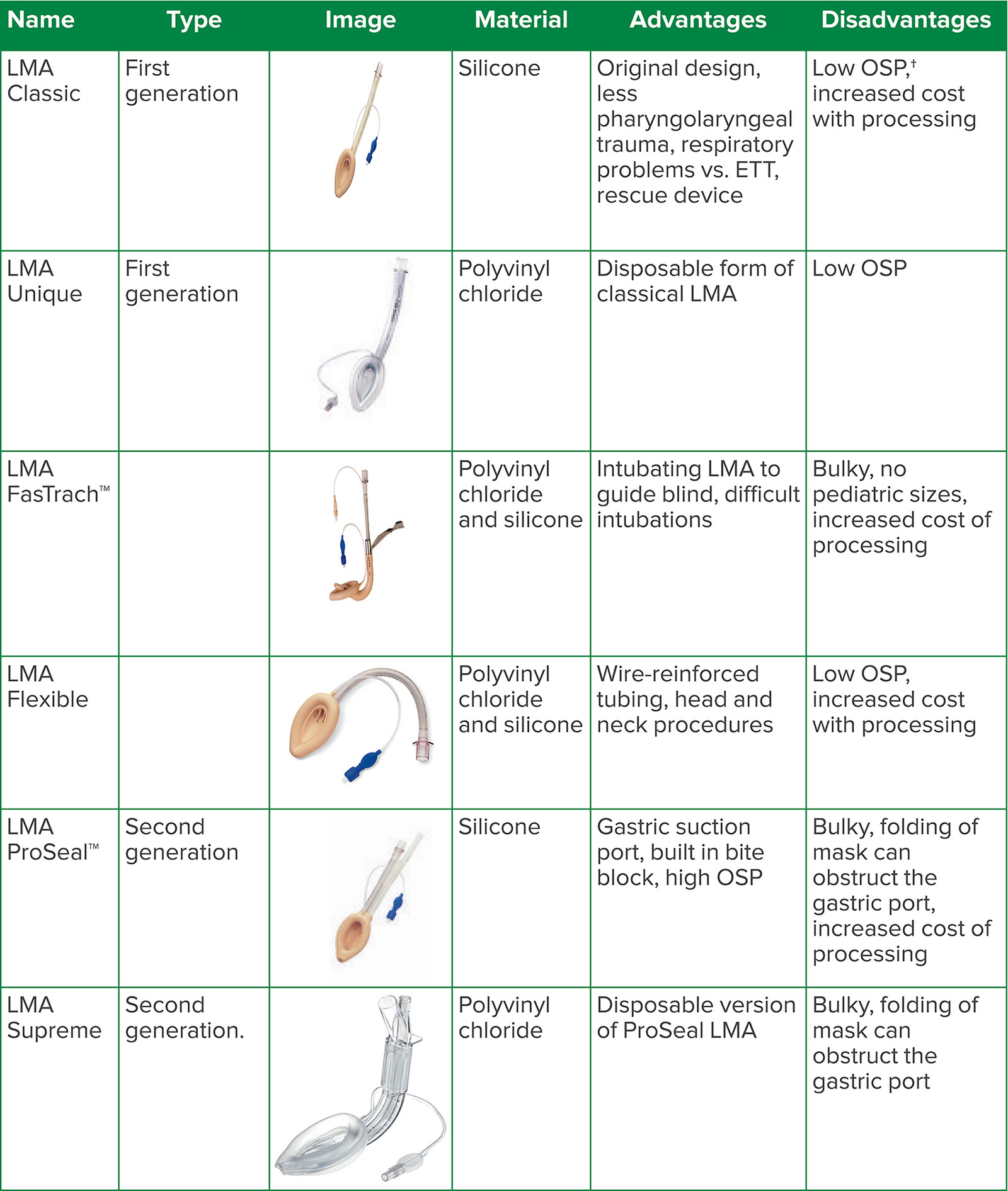
*More supraglottic devices exist and are manufactured by a variety of companies. This table includes first- and second-generation devices discussed in the review.
†OSP: oropharyngeal seal pressure. Lower OSP increases gastric insufflation and risk of aspiration.1
Images courtesy of Teleflex Incorporated and reproduced and modified with permission. © 2020 Teleflex Incorporated. All rights reserved.
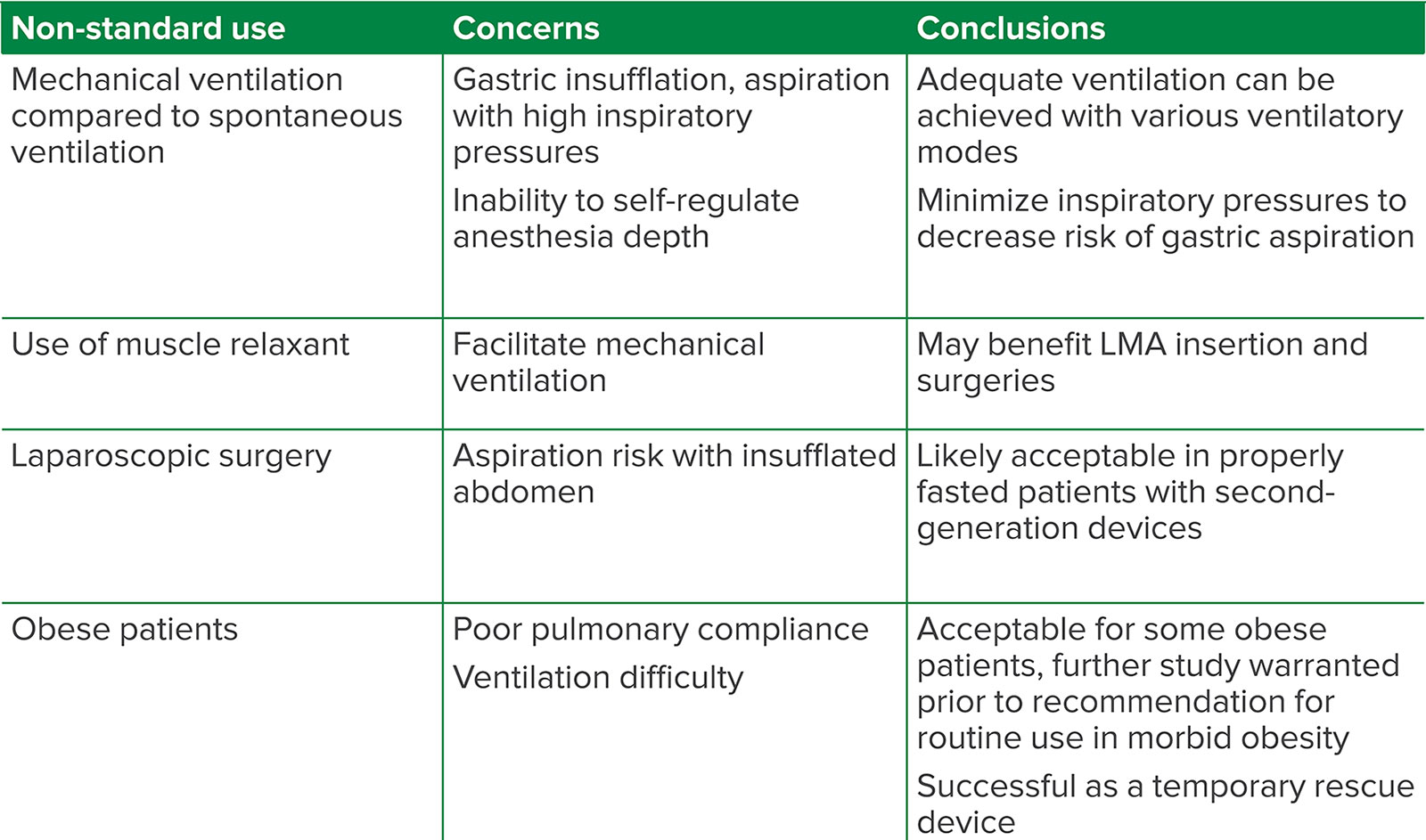
Table 2. Summary of Non-Standard Uses of the Laryngeal Mask Airway (LMA)
LMA Placement and Size Selection
The LMA may be easily placed following induction of general anesthesia, with or without a muscle relaxant.10 In a study by Hemmerling et al., the success rate of first attempt insertion was 92% with the use of muscle relaxant versus 89% without muscle relaxant.10 If the LMA size selected is too small, it may not create an adequate seal, leading to leakage, which may result in insufficient ventilation.11 If the device is too large, it may lead to reduced adaptability, also resulting in a poor seal or leak. This may also result in soft tissue, lingual nerve injury, or even pharyngeal damage if it was forcefully placed. Size 4 and 5 LMAs are appropriate in most average female and male adults, respectively. In a study by Asai et al., leaks were reduced with placement of the larger size LMAs in both males and females.11 Minimal inflation volumes were used to create an adequate seal, resulting in less pressure measured on the pharynx.11 Brimacombe et al. investigated pharyngolaryngeal complaints in 300 patients comparing LMA use with low cuff volumes and LMA with high cuff volumes and found a higher incidence of sore throat and dysphagia in the latter group.3 In a prospective study of 5,264 patients, Higgins et al. found that the incidence of a sore throat with an ETT versus an LMA was 45.4% and 17.5% of patients, respectively.4 Although the incidence of a sore throat may be higher with ETTs compared with LMAs, inappropriate LMA size and high cuff pressures may also contribute to significant pharyngolaryngeal complications; thus, importance should be placed more on minimizing intracuff volume.4-6,11 In a Cochrane review, Mathew et al. pooled 15 randomized controlled trials with 2,242 patients to assess whether it was better to remove the LMA under deep anesthesia or when patients are awake. The review concluded that there was not sufficient high-quality evidence to determine if one method was superior to the other.12
Aspiration Risk with LMA
A frequent concern regarding LMA use is the risk for aspiration, particularly when PPV is applied. The most common contraindications to LMA placement include patients at risk of aspiration such as during pregnancy, trauma, pre-existing gastroparesis, intestinal obstruction, or emergency surgery in nonfasted patients. Table 3 provides an overview of absolute and relative contraindications to the LMA. In appropriately fasted patients, several studies have identified the risk of aspiration with an LMA as extremely low.8,9 Brimacombe et al. reported the incidence of pulmonary aspiration with an LMA to be 2 per 10,000 compared with 1.7 per 10,000 for an ETT and facemask, in a similar patient cohort.9 In a study performed by Bernardini and Natalini with 65,712 surgical procedures, including 2,517 laparoscopic surgeries and major abdominal surgeries, there was no significant difference in the rate of aspiration for the classic LMA in comparison with an ETT while using PPV.8 In a meta-analysis, Park et al. compared second-generation LMAs to ETTs in 1,433 patients undergoing laparoscopic surgery and found no difference in oropharyngeal leak pressure, gastric insufflation, or aspiration.6 The lack of difference in oropharyngeal leak pressure suggests a degree of airway protection and sufficient mechanical ventilation even against an insufflated abdomen.6 LMAs have been successful in laparoscopic procedures, but caution with use is warranted. Second-generation devices may be more appropriate for laparoscopic surgery with higher oropharyngeal seal pressure and gastric suction port.6
Table 3. Absolute and Relative Contraindications to LMA8,9,13,14
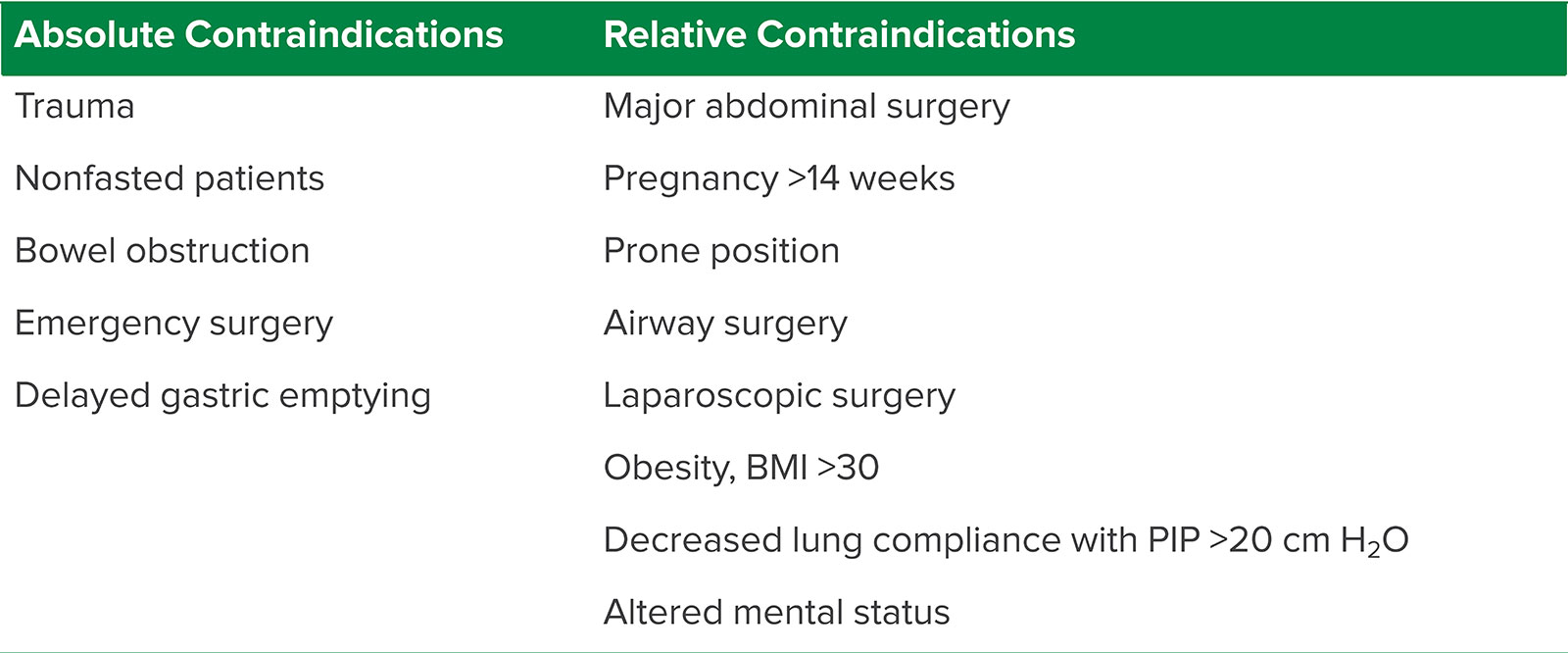
BMI = body mass index; LMA = laryngeal mask airway; PIP = peak inspiratory pressure
Some second-generation LMAs contain a gastric channel for placement of an orogastric tube to prevent aspiration (Table 1). In a large observational study, 700 appropriately fasted patients underwent general anesthesia for cesarean section with the LMA Supreme™.15 There were no reported cases of aspiration using the LMA Supreme™ with placement of an orogastric tube through the gastric port.15
Positive inspiratory pressure greater than 15 cm H2O has been suggested to lead to incompetence of the lower esophageal sphincter and result in insufflation of air into the stomach with the potential for aspiration.16 Devitt et al. assessed the leak fractions, measured from subtracting expiratory volume from inspiratory volume divided by inspiratory volume, and gastric insufflation comparing classical LMAs versus standard endotracheal intubation at various inspiratory pressures. The leak fraction increased with increasing positive pressure delivered through the LMA and remained low and unchanged in the ETTs. At an inspired pressure of 15 cm H2O, the gastric insufflation with LMA use was 2.1%, while it was 35.4% with a pressure of 30 cm H2O.17 In a Cochrane review comparing the ProSeal™ LMA, a second-generation LMA with a gastric suction port and a posterior cuff for an improved seal, with Classical LMA with PPV, Qamarul Hoda et al. concluded that there was no significant difference in rates of regurgitation.18 Both older and newer generations of the LMA have been successfully used without clinical signs of aspiration if inspiratory pressures are limited to 15 cm H2O or lower.17,18
Spontaneous Ventilation vs. Mechanical Ventilation
A benefit of LMA use is that it is less stimulating to a patient than an ETT; therefore, less anesthesia is often required.19 Due to increasing comfort with use and the development of a new generation of devices, LMAs are routinely used safely with mechanical ventilation.18,20-24 Radke et al. assessed the redistribution of ventilation by using electrical impedance tomography in patients undergoing general anesthesia with an LMA.22 They observed no redistribution of ventilation with patients breathing spontaneously, and found ventral redistribution under both pressure-controlled ventilation (PCV) and pressure support ventilation (PSV).22 Consequences of ventral distribution of ventilation include increased dead space and atelectasis.21,24 The use of volume control ventilation (VCV) with an LMA results in less compliance and higher peak inspiratory pressures compared to PCV. PCV, an alternative mode of ventilation, limits the inspired pressure to maintain a set tidal volume.22 End-tidal carbon dioxide was higher, tidal volumes were smaller, and oxygen saturation was lower in patients undergoing spontaneous breathing (SB) compared to PCV, VCV, and PSV modes.21,23 Brimacombe and Keller found improved oxygenation and ventilation with the LMA by using PSV compared with continuous positive airway pressure (CPAP).21
There was no difference in gastric insufflation, airway or cardiovascular complications, or problems ventilating patients in a study by Keller et al. comparing spontaneous ventilation to PPV.24,25 In a Cochrane review, the classic LMA was compared to the ProSeal™ LMA undergoing PPV.18 The ProSeal™ LMA had a better seal, suggesting that it may be more suitable for PPV; however, overall the quality of evidence was low.18 In a randomized controlled trial, Capdevila et al. examined various modes of ventilation, VCV, PSV, and SB, on emergence time and intraoperative ventilation.23 Time to classic LMA removal was prolonged in patients undergoing VCV compared with PSV or SB.23
Obesity and the LMA
Another area of controversy is LMA use in obese patients. Physiological changes seen in obese patients make them a challenging population, including a restrictive lung pattern due to abdominal contents limiting diaphragm motion and yielding less respiratory compliance.20 Insufflation during laparoscopic procedures can further impair lung compliance and make ventilation difficult.20 Cheong et al. found that in patients with a body mass index (BMI) over 30, there was a 2.5 times increased risk of having ventilatory problems.26 Zoremba et al. assessed postoperative lung function and saturations in obese patients (BMI 30 to 35) undergoing minor peripheral surgery with a ProSeal LMA™ vs. ETT.27 and found ventilation was adequate in both groups while postoperative pulmonary complications were decreased in the LMA group.27 Keller et al. showed that the ProSeal™ LMA was temporarily effective in ventilating obese patients with a BMI >35 prior to intubation.28 Although second-generation LMAs have been used in obese patients, further studies should be done to investigate the safety of LMA use in obese patients.
Summary
LMA design has evolved and clinical use has expanded significantly in recent decades. Evidence suggests that LMA use is safe with mechanical ventilation in appropriately fasted patients while minimizing the inspiratory pressures applied. Second-generation devices may minimize leak and limit gastric insufflation compared to first-generation LMAs. Muscle relaxant may be considered and has been shown to facilitate LMA insertion and mechanical ventilation. Use of LMA in obese patient remains controversial. Studies have proved successful ventilation of obese patients with a BMI below 30. However, in patients with higher BMIs, ventilation may be impaired due to physiologic changes in obesity. The LMA should always be considered as a rescue device for difficult ventilation or intubation, regardless of patient size. Appropriate LMA indications continue to be debated. It is important to recognize the potential complications and relative contraindications to the LMA and adjust a clinical algorithm, which would optimize the use of the LMA in airway management.
Shauna Schwartz, DO, is a cardiothoracic anesthesia fellow in the Department of Anesthesiology at the University of Florida College of Medicine, Gainesville, FL.
Yong G. Peng, MD, PhD, is a professor of Anesthesiology and chief of the Cardiothoracic Anesthesia Division in the Department of Anesthesiology and associate professor of Surgery, University of Florida College of Medicine, Gainesville, FL.
The authors have no conflicts of interest.
References
- Sharma B, Sahai C, Sood J. Extraglottic airway devices: technology update [published correction appears in Med Devices (Auckl).2018;1127]. Med Devices (Auckl). 2017;10:189–205.
- Brimacombe J. The advantages of the LMA over the tracheal tube or facemask: a meta-analysis. Can J Anaesth. 1995;42:1017–1023.
- 3. Brimacombe J, Holyoake L, Keller C, et al. Pharyngolaryngeal, neck, and jaw discomfort after anesthesia with the face mask and laryngeal mask airway at high and low cuff volumes in males and females. Anesthesiology. 2000;93:26–31.
- Higgins PP, Chung F, Mezei G. Postoperative sore throat after ambulatory surgery. Br J Anaesth. 2002;88:582–584.
- Figueredo E, Vivar-Diago M, Muñoz-Blanco F. Laryngo-pharyngeal complaints after use of the laryngeal mask airway. Can J Anaesth. 1999;46:220–225.
- Park SK, Ko G, Choi GJ, et al. Comparison between supraglottic airway devices and endotracheal tubes in patients undergoing laparoscopic surgery: a systematic review and meta-analysis. Medicine (Baltimore). 2016;95:e4598.
- Updated by the Committee on Standards and Practice Parameters, Apfelbaum JL, Hagberg, CA Caplan RA, et. al. The previous update was developed by the American Society of Anesthesiologists Task Force on Difficult Airway Management, Caplan RA, Benumof JL, Berry FA, et al; Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2013;118:251–270.
- Bernardini A, Natalini G. Risk of pulmonary aspiration with laryngeal mask airway and tracheal tube: Analysis on 65 712 procedures with positive pressure ventilation. Anaesthesia. 2009;64:1289–1294.
- Brimacombe JR, Berry A. The incidence of aspiration associated with the laryngeal mask airway: A meta-analysis of published literature. J Clin Anesth. 1995;7:297–305.
- Hemmerling TM, Beaulieu P, Jacobi KE, et al. Neuromuscular blockade does not change the incidence or severity of pharyngolaryngeal discomfort after LMA anesthesia. Can J Anaesth. 2004;51:728–732.
- Asai T, Howell TK, Koga K, Morris S. Appropriate size and inflation of the laryngeal mask airway. Br J Anaesth. 1998;80:470–474.
- Mathew PJ, Mathew JL. Early versus late removal of the laryngeal mask airway (LMA) for general anaesthesia. Cochrane Database of Syst Rev. 2015;(8):CD007082.
- Teleflex. LMA Better by Design. Accessed July 26, 2020. https://www.lmaco-ifu.com/ifu?category=1
- Kallar SK, Everett LL. Potential risks and preventative measures for pulmonary aspiration: new concepts in preoperative fasting guidelines. Anesth Analg. 1993;77:171–182.
- Yao WY, Li SY, Sng BL, et al. The LMA Supreme™ in 700 parturients undergoing Cesarean delivery: an observational study. Can J Anesth. 2012;59:648–654.
- Bouvet L, Albert ML, Augris C, et al. Real-time detection of gastric insufflation related to facemask pressure–controlled ventilation using ultrasonography of the antrum and epigastric auscultation in nonparalyzed patients: a prospective, randomized, double-blind study. Anesthesiology. 2014;120:326–334.
- Devitt JH, Wenstone R, Noel AG, O’Donnell MP. The laryngeal mask airway and positive-pressure ventilation. Anesthesiology. 1994;80:550–555.
- Qamarul Hoda M, Samad K, Ullah H. ProSeal versus Classic laryngeal mask airway (LMA) for positive pressure ventilation in adults undergoing elective surgery. Cochrane Database Syst Rev. 2017;7:CD009026.
- Wilkins CJ, Cramp PG, Staples J, Stevens WC. Comparison of the anesthetic requirement for tolerance of laryngeal mask airway and endotracheal tube. Anesth Analg. 1992;75:794–7
- Miller RD. Miller’s Anesthesia. 7th ed. Philadelphia, PA: Churchill Livingstone/Elsevier; 2010.
- Brimacombe J, Keller C, Hörmann C. Pressure support ventilation versus continuous positive airway pressure with the laryngeal mask airway: a randomized crossover study of anesthetized adult patients. Anesthesiology. 2000;92:
1621–1623. - Radke OC, Schneider T, Heller AR, Koch T. Spontaneous breathing during general anesthesia prevents the ventral redistribution of ventilation as detected by electrical impedance tomography: a randomized trial. Anesthesiology. 2012;116:1227–1234.
- Capdevila X, Jung B, Bernard N, et al. Effects of pressure support ventilation mode on emergence time and intra-operative ventilatory function: a randomized controlled trial. PLoS One. 2014;9:e115139.
- Keller C, Sparr HJ, Luger TJ, Brimacombe J. Patient outcomes with positive pressure versus spontaneous ventilation in non-paralysed adults with the laryngeal mask. Can J Anaesth. 1998;45:564–567.
- Soni N, Williams P. Positive pressure ventilation: what is the real cost? Br J Anaesth. 2008;101:446–457.
- Cheong G, Siddiqui S, Lim T, et al. Thinking twice before using the LMA for obese and older patients-a prospective observational study. J Anesth Clin Res. 2013;4:2.
- Zoremba M, Aust H, Eberhart L, et al. Comparison between intubation and the laryngeal mask airway in moderately obese adults. Acta Anaesthesiol Scand. 2009;53:436–442.
- Keller C, Brimacombe J, Kleinsasser A, Brimacombe L. The Laryngeal Mask Airway ProSeal™ as a temporary ventilatory device in grossly and morbidly obese patients before laryngoscope-guided tracheal intubation. Anesth Analg. 2002;94:
737–740.
