The recently published 2022 ASA guidelines for managing the difficult airway are a significant change from previous guidelines. These changes are meant to assist clinicians in decision-making. As airway management equipment improves, human factor concerns, team-based performance, and cognitive errors remain hurdles to safe airway management. Change can be difficult and, in this article, the authors highlight some of the important changes to the guidelines.
Robert Glazer, founder and chairman of the Board of a global partner marketing agency, shares a blog every Friday called “Friday Forward,” which we highly recommend (https://www.robertglazer.com/fridayfwd/). In it, he described the four stages of change:
- Confusion and surprise—“Huh? why did you change that?”
- Reacting to differences—“Why is this different, not sure I like that.”
- Pining for the past—“Oh, I wish I had the old version back, this sucks.”
- Adaptation and acceptance—“Hmm, this may actually be better, I think I like it.”
Many of you may have had one of these reactions to the new ASA practice guidelines for managing the difficult airway. Regardless of which stage of change you’re in, this article will highlight changes to the guidelines and usher you closer to the final stage of change.
Guideline history
The initial ASA Practice Guidelines for Management of the Difficult Airway were published in 1993. Since then, the ASA Committee on Standards and Practice Parameters (now the Committee on Practice Parameters) has been tasked with reviewing each guideline published by the various task forces every five years. Additionally, each guideline must undergo a complete revision at least every ten years. This version, published in January 2022, is the revision of the 2013 ASA Guidelines.1 This article summarizes the fundamental changes to the previous guidelines and emphasizes important considerations to enhance patient safety in airway management.
New International Perspectives
The guidelines were developed by a task force of 15 members, including anesthesiologists and methodologists representing the United States, India, Ireland, Italy, Switzerland, and several subspecialty organizations.
Guidance for Both Pediatric Patients and Adults
Traditionally, these guidelines have focused on adult airway management. However, anesthesia professionals are increasingly managing children. These guidelines include evidence and expert opinion on pediatric difficult airway management, which is a significant change that makes the guidelines more comprehensive.
New Technology, Literature, and Expert Opinion Evidence
This update summarizes evidence from reviewing thousands of abstracts pared down to 560 references. Additionally, this iteration surveyed expert consultants, ASA members, and ten participating organizations on topics where the scientific evidence was scant or equivocal. It also updates the equipment and technology available for standard and difficult airway management.
Emphasis on Oxygen Delivery and CO2 Confirmation
This version emphasizes oxygen administration throughout difficult airway management and during extubation. Additionally, it emphasizes using capnography to confirm tracheal intubation as in previous versions.
Situational Awareness of Attempts, the Passage of Time, and Oxygen Saturation
These updated guidelines emphasize the importance of paying attention to the elapsed time during airway management. Too often, a team can suffer from task fixation, leading to multiple attempts using a single approach and failure to consider alternatives. Additionally, awareness of the oxygen saturation can enable early intervention and decision-making and limit the number of attempts. This increased situational awareness may help clinicians progress steadily through their planned airway management and recognize the need for a surgical airway earlier. A team-centered approach is best, and one approach is to assign an observer not involved with direct airway management as the arbiter of task fixation.
Pre-induction Decision Chart for Awake vs. Asleep Airway Management
Previous guidelines have been valuable for planning and identifying potential obstacles in developing a difficult airway management strategy. They included questions that helped with decision-making regarding awake airway management. However, judgment errors (i.e., not performing awake intubation when indicated) have led to failed airway securement, according to several reviews.2,3 To further support decision-making, this update includes a decision tree to aid in determining when awake airway management is indicated (Figure 1, Part 1). This decision tree is an extension and evolution of a work product published in 2004 by a task force member and adapted for the 2022 ASA algorithm.4 Awake intubation of the adult patient should be considered when there is (1) difficult ventilation (face mask/supraglottic airway), (2) increased risk of aspiration, (3) intolerance of brief apnea, or (4) expected difficulty with emergency invasive airway access.
Additionally, the new figures directly address the unanticipated difficult airway by including entry points after failed intubation after routine induction.
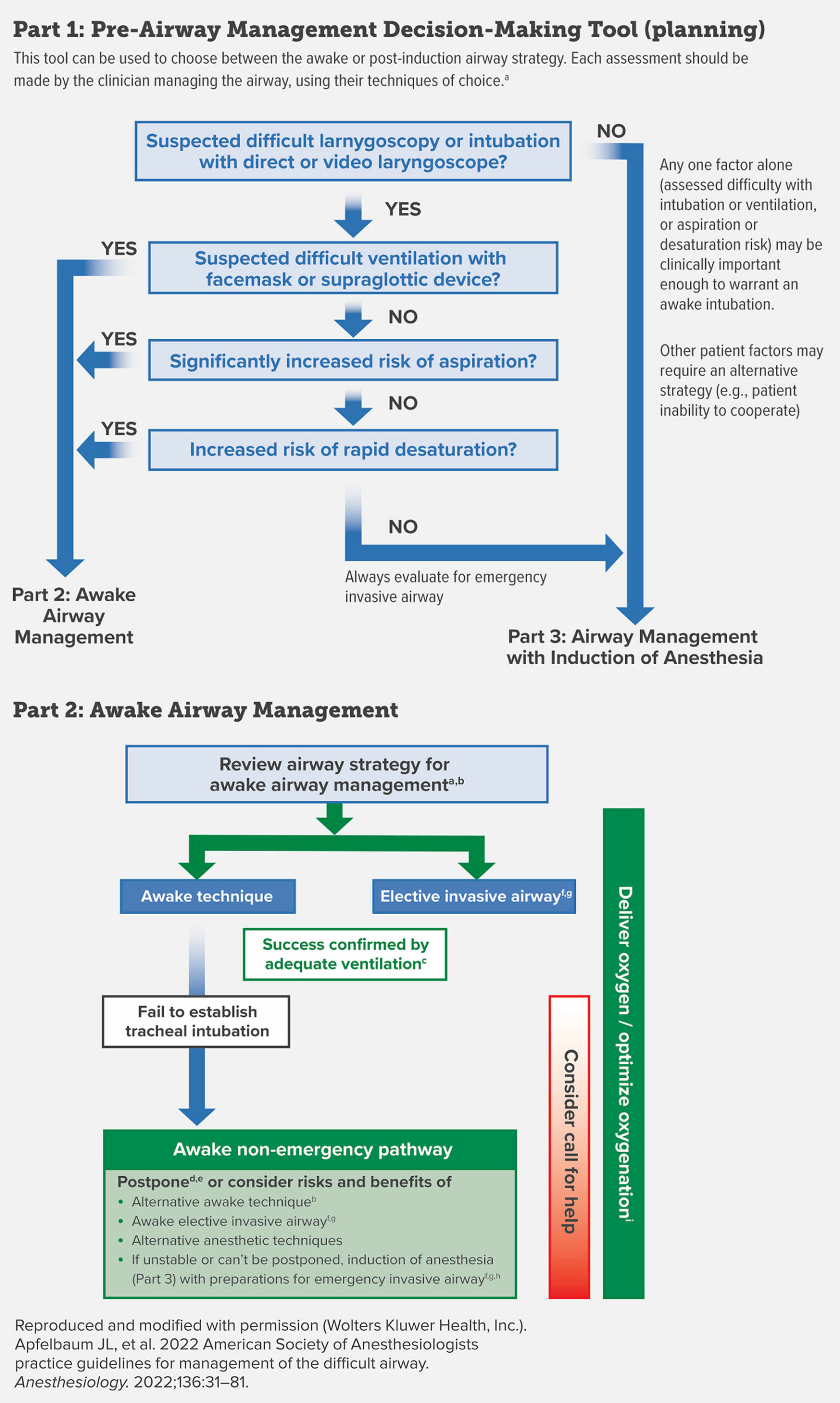
Figure 1, Parts 1 and 2: Difficult Airway Infographic for Adult Patients.
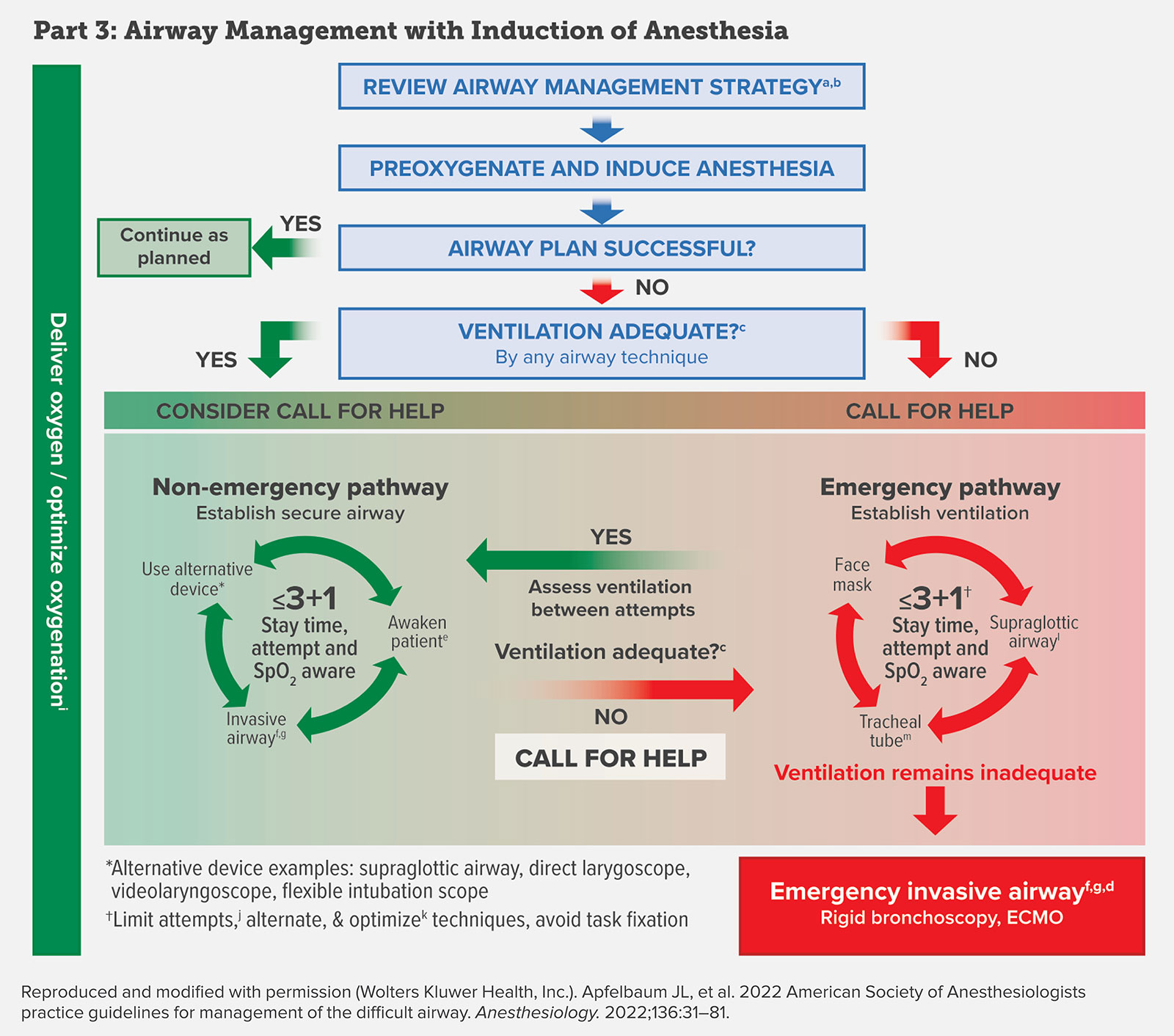
Figure 1, Part 3: Difficult Airway Infographic for Adult Patients.
Difficult airway infographic: Adult patient example. This figure provides three tools to aid in airway management for the patient with a planned, anticipated difficult, or unanticipated difficult airway. Part 1 is a decision tool that incorporates relevant elements of evaluation and is intended to assist in the decision to enter the awake airway management pathway or the airway management with the induction of anesthesia pathway of the ASA difficult airway algorithm. Part 2 is an awake intubation algorithm. Part 3 is a strategy for managing patients with induction of anesthesia when an unanticipated difficulty with ventilation (as determined by capnography) with a planned airway technique is encountered. a. The airway manager’s assessment and choice of techniques should be based on their previous experience; available resources, including equipment, availability, and competency of help; and the context in which airway management will occur. b. Review airway strategy: Consider anatomical/physiologic airway difficulty risk, aspiration risk, infection risk, other exposure risk, equipment and monitoring check, role assignment, and backup and rescue plans. Awake techniques include flexible intubation scope, videolaryngoscopy, direct laryngoscopy, supraglottic airway, combined devices, and retrograde wire-aided. c. Adequate ventilation by any means (e.g., face mask, supraglottic airway, tracheal intubation) should be confirmed by capnography, when possible. d. Follow-up care includes postextubation care (i.e., steroids, racemic epinephrine), counseling, documentation, team debriefing, and encouraging patient difficult airway registry. e. Postpone the case/intubation and return with appropriate resources (e.g., personnel, equipment, patient preparation, awake intubation). f. Invasive airways include surgical cricothyroidotomy, needle cricothyroidotomy with a pressure-regulated device, large-bore cannula cricothyroidotomy, or surgical tracheostomy. Elective invasive airways include the above, retrograde wire-guided intubation, and percutaneous tracheostomy. Other options include rigid bronchoscopy and ECMO. g. Invasive airway is performed by an individual trained in invasive airway techniques, whenever possible. h. In an unstable situation or when airway management is mandatory after a failed awake intubation, a switch to the airway management with the induction of anesthesia pathway may be entered with preparations for an emergency invasive airway. i. Low- or high-flow nasal cannula, head elevated position throughout procedure. Noninvasive ventilation during preoxygenation. j.The intent of limiting attempts at tracheal intubation and supraglottic airway insertion is to reduce the risk of bleeding, edema, and other types of trauma that may increase the difficulty of mask ventilation and/or subsequent attempts to secure a definitive airway. Persistent attempts at any airway intervention, including ineffective mask ventilation, may delay obtaining an emergency invasive airway. A reasonable approach may be to limit attempts with any technique class (i.e., face mask, supraglottic airway, tracheal tube) to three, with one additional attempt by a clinician with higher skills. k. Optimize: suction, relaxants, repositioning. Face mask: oral/nasal airway, two-hand mask grip. Supraglottic airway: size, design, repositioning, first versus second generation. Tracheal tube: introducer, rigid stylet, hyperangulated videolaryngoscopy, blade size, external laryngeal manipulation. Consider other causes of inadequate ventilation (including but not limited to laryngospasm and bronchospasm). l. First versus second generation supraglottic airway with intubation capability for initial or rescue supraglottic airway. m. Videolaryngoscopy as an option for initial or rescue tracheal intubation.
New Algorithms and Infographics for Adult and Pediatric Difficult Airway Management
Tremendous time and effort were spent improving the new infographic’s flow and “real-time” usability. The new algorithm now includes a section that includes options involved in deciding to proceed with an awake airway (Figure 1, Part 2) as well as a section that is more amenable to “real-time” use (Figure 1, Part 3). The graphical design flows more like a cognitive aid than an algorithm, but requires review and familiarity before real-time use.
Both infographics are color-coded to represent the ability to ventilate. Green represents easy ventilation, yellow marginal, and red impossible ventilation. A time-out should occur before the start of airway management to discuss the care plan.
The team should identify the primary airway manager, the backup airway manager, the equipment to be used, and the person available to help if feasible. Both infographics highlight the importance of assessing ventilation after each attempt or intervention; the results of this assessment may move the clinician to a different point in the algorithm.
The pediatric algorithm highlights three main tools for managing a child with a difficult airway: the supraglottic airway (SGA), flexible intubation scope (FIS), and video laryngoscopy (VL) (Figure 2). These devices can be combined (e.g., FIS + SGA or FIS +VL) if they fail individually. These tools are most applicable to use in the easy ventilation zone; however, when ventilation is difficult, the clinician should focus on their best attempts to reestablish ventilation using a facemask, supraglottic airway device, and adjuncts, as well as their best attempt to perform tracheal intubation with the technique most likely to be successful. Both infographics highlight the importance of limiting attempts. The pediatric algorithm highlights the importance of distinguishing between functional and anatomical obstruction as their treatments differ. Drugs are required for functional obstruction and devices such as oropharyngeal, nasopharyngeal, and supraglottic airway devices for anatomic obstruction. A team debrief should be considered after airway management to codify lessons learned, allow team members to express any difficult emotions, and identify gaps for improvement.
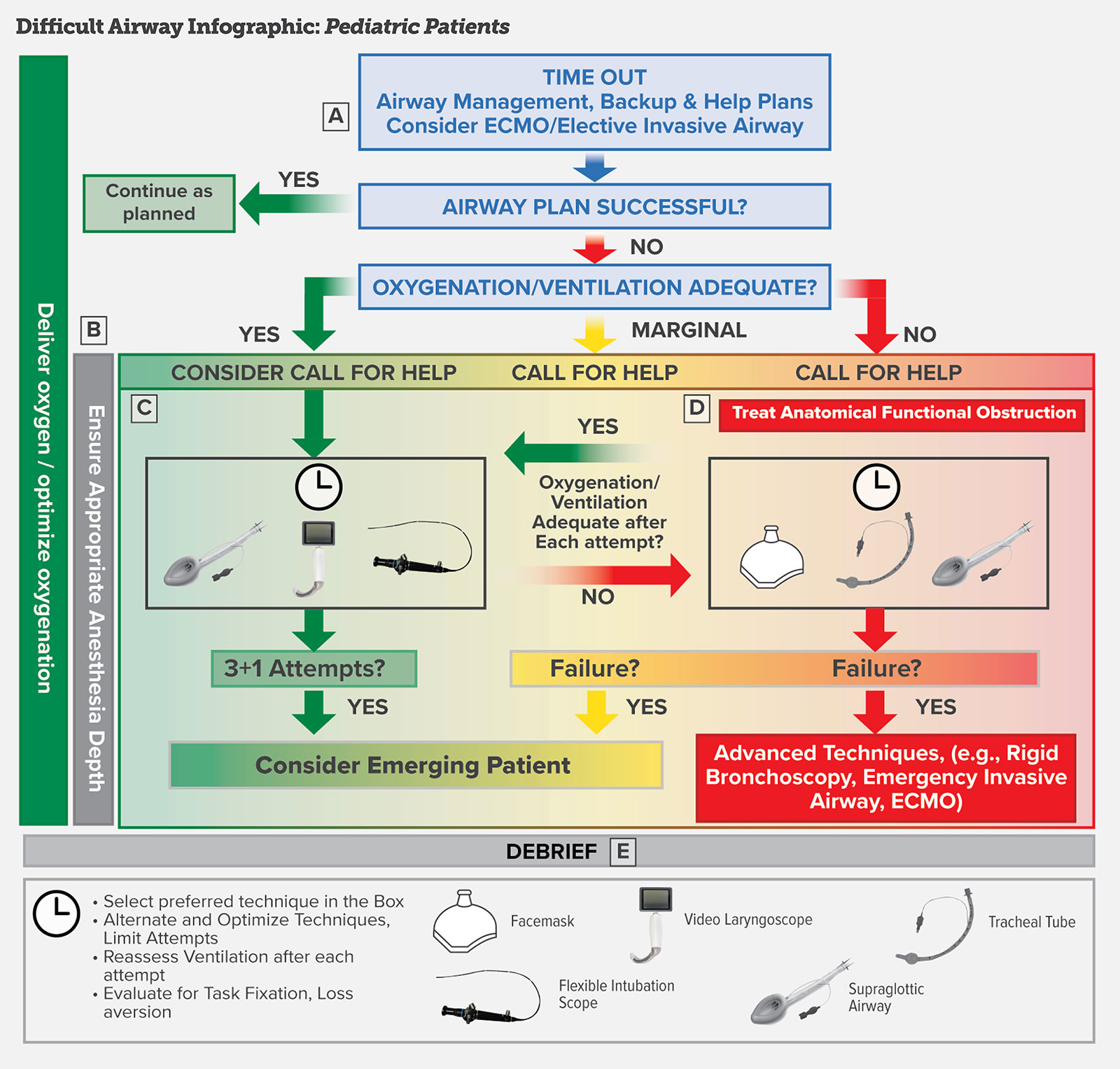
Figure 2: Difficult Airway Infographic: Pediatric Patients
Difficult airway infographic: Pediatric patient example. A. Time Out for identification of the airway management plan. A team-based approach with identification of the following is preferred: the primary airway manager and backup manager and role assignment, the primary equipment and the backup equipment, and the person(s) available to help. Contact an ECMO team/otolaryngologic surgeon if noninvasive airway management is likely to fail (e.g., congenital high airway obstruction, airway tumor, etc.). B. Color scheme. The colors represent the ability to oxygenate/ventilate: green, easy oxygenation/ventilation; yellow, difficult or marginal oxygenation/ventilation; and red, impossible oxygenation/ventilation. Reassess oxygenation/ventilation after each attempt and move to the appropriate box based on the results of the oxygenation/ventilation check. C. Nonemergency pathway (oxygenation/ventilation adequate for an intubation known or anticipated to be challenging): deliver oxygen throughout airway management; attempt airway management with the technique/device most familiar to the primary airway manager; select from the following devices: supraglottic airway, videolaryngoscopy, flexible bronchoscopy, or a combination of these devices (e.g., flexible bronchoscopic intubation through the supraglottic airway); other techniques (e.g., lighted stylets or rigid stylets may be used at the discretion of the clinician); optimize and alternate devices as needed; reassess ventilation after each attempt; limit direct laryngoscopy attempts (e.g., one attempt) with consideration of standard blade videolaryngoscopy in lieu of direct laryngoscopy; limit total attempts (insertion of the intubating device until its removal) by the primary airway manager (e.g., three attempts) and one additional attempt by the secondary airway manager; after four attempts, consider emerging the patient and reversing anesthetic drugs if feasible. Clinicians may make further attempts if the risks and benefits to the patient favor continued attempts. D. Marginal/emergency pathway (poor or no oxygenation/ventilation for an intubation known or anticipated to be challenging): treat functional (e.g., airway reflexes with drugs) and anatomical (mechanical) obstruction; attempt to improve ventilation with facemask, tracheal intubation, and supraglottic airway as appropriate; and if all options fail, consider emerging the patient or using advanced invasive techniques. E. Consider a team debrief after all difficult airway encounters: identify processes that worked well and opportunities for system improvement and provide emotional support to members of the team, particularly when there is patient morbidly or mortality.
Developed in collaboration with the Society for Pediatric Anesthesia and the Pediatric Difficult Intubation Collaborative: John E. Fiadjoe, MD; Thomas Engelhardt, MD, PhD, FRCA; Nicola Disma, MD; Narasimhan Jagannathan, MD, MBA; Britta S. von Ungern-Sternberg, MD, PhD, DEAA, FANZCA; and Pete G. Kovatsis, MD, FAAP.
Pediatric Highlights
The early consideration of extracorporeal membrane oxygenation (ECMO) is highlighted in pediatric airway management. Airway management after inhaled induction is typical, while awake intubation is not commonly performed in children. The guidelines emphasize the importance of maintaining an adequate depth of anesthesia with ventilation assessment after every intubation attempt. The minimum number of attempts should be performed. Other rescue techniques to consider include rigid bronchoscopy by a clinician familiar with the method. Airway exchange catheters should be used with caution in children and used by clinicians experienced with their use. There is a small margin for error, and potential severe outcomes such as pneumothorax and pneumomediastinum may occur if the catheter perforates the airway.
Devices and Technology
Meta-analyses of randomized trials have demonstrated that video-assisted laryngoscopy in patients with predicted difficult airways improves laryngeal views and first-attempt intubation success compared to direct laryngoscopy.5-15 These results were equivocal when comparing video-assisted laryngoscopy to flexible intubation scopes. Interestingly, randomized studies were also equivocal for the same outcomes when hyperangulated video laryngoscopes were compared to non-angulated video laryngoscopes in anticipated difficult airway patients.13 Combination techniques may improve intubation success in patients with anticipated difficult airways. For example, using a flexible intubation scope through a supraglottic airway had a higher first-attempt success rate than using the flexible intubation scope alone.16-19
Extubation and Documentation
The guidelines highlight the importance of having an extubation strategy and preparing for reintubation if necessary. Consideration should be given to the personnel, the extubation location, and the equipment available. After extubation of difficult airway patients, clinicians should consider using an airway exchange catheter or laryngeal mask to allow rapid reintubation. The guidelines highlight the importance of communication and documentation. The clinical management must be communicated to the patient and documented in a letter. The patient should be encouraged to register with an emergency notification service. A detailed note should be added to the medical record.
ASA House of Delegates (HOD) Approval
The ASA HOD must approve all work products from the ASA Committee on Standards and Practice Parameters. A working draft of the guidelines was placed on the ASA website for all to review. All submitted comments were considered for inclusion. Interestingly, one of the common comments was that a portion of the ASA membership preferred the previous black and white algorithm style. Therefore, the algorithm was mainly kept in its original form with some minor modifications (Figure 3 and 4) after ASA HOD approval at the ASA annual meeting in October 2021.
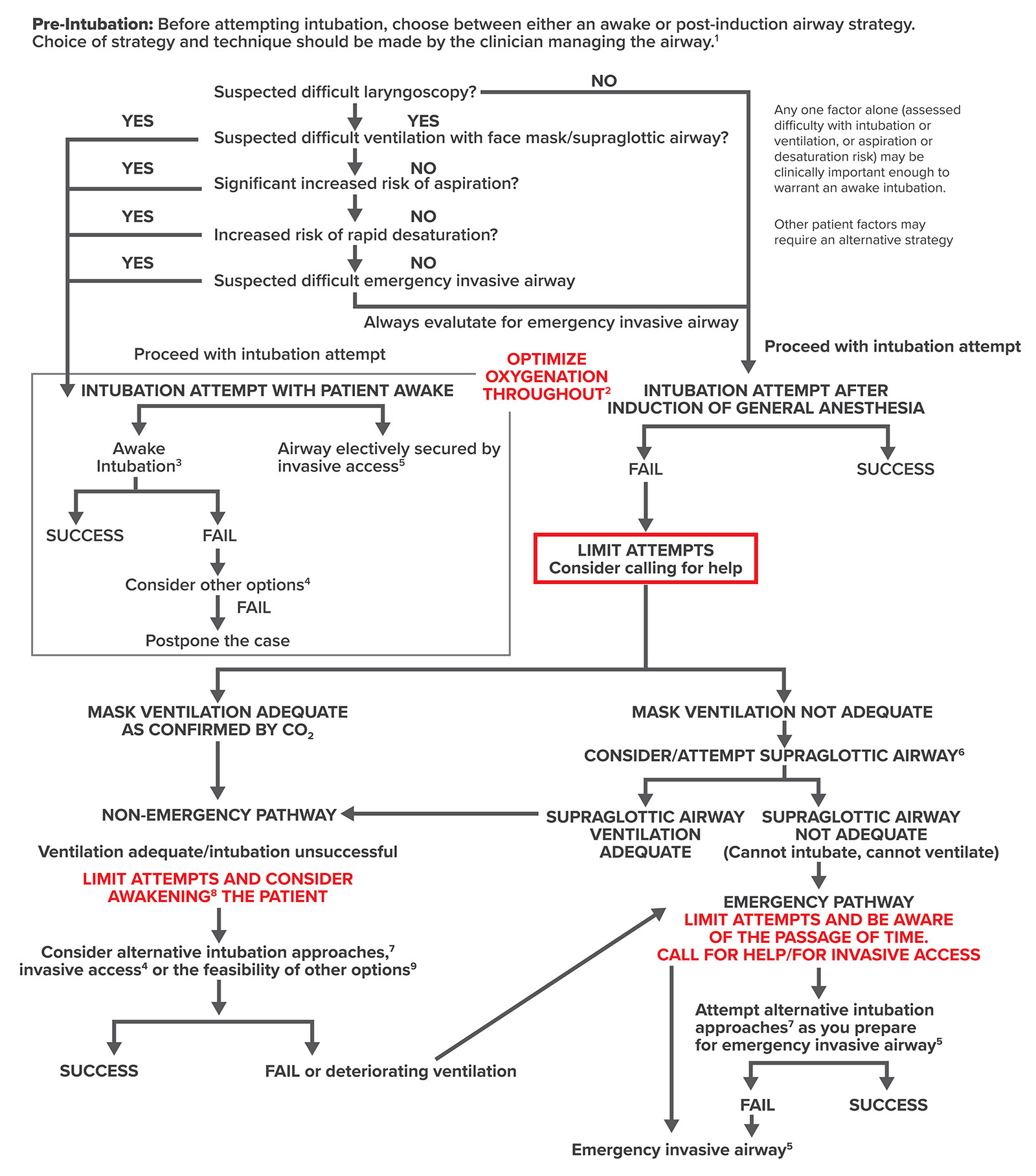
Figure 3: ASA Difficult Airway Algorithm: Adult Patients.
Figure 3. Difficult airway algorithm: Adult patients. 1. The airway manager’s choice of airway strategy and techniques should be based on their previous experience; available resources, including equipment, availability and competency of help; and the context in which airway management will occur. 2. Low- or high-flow nasal cannula, head elevated position throughout procedure. Noninvasive ventilation during preoxygenation. 3. Awake intubation techniques include flexible bronchoscope, videolaryngoscopy, direct laryngoscopy, combined techniques, and retrograde wire-aided intubation. 4. Other options include, but are not limited to, alternative awake technique, awake elective invasive airway, alternative anesthetic techniques, induction of anesthesia (if unstable or cannot be postponed) with preparations for emergency invasive airway, and postponing the case without attempting the above options. 5. Invasive airway techniques include surgical cricothyrotomy, needle cricothyrotomy with a pressure-regulated device, large-bore cannula cricothyrotomy, or surgical tracheostomy. Elective invasive airway techniques include the above and retrograde wire–guided intubation and percutaneous tracheostomy. Also consider rigid bronchoscopy and ECMO. 6. Consideration of size, design, positioning, and first versus second generation supraglottic airways may improve the ability to ventilate. 7. Alternative difficult intubation approaches include but are not limited to video-assisted laryngoscopy, alternative laryngoscope blades, combined techniques, intubating supraglottic airway (with or without flexible bronchoscopic guidance), flexible bronchoscopy, introducer, and lighted stylet or lightwand. Adjuncts that may be employed during intubation attempts include tracheal tube introducers, rigid stylets, intubating stylets, or tube changers and external laryngeal manipulation. 8. Includes postponing the case or postponing the intubation and returning with appropriate resources (e.g., personnel, equipment, patient preparation, awake intubation). 9. Other options include, but are not limited to, proceeding with procedure utilizing face mask or supraglottic airway ventilation. Pursuit of these options usually implies that ventilation will not be problematic.
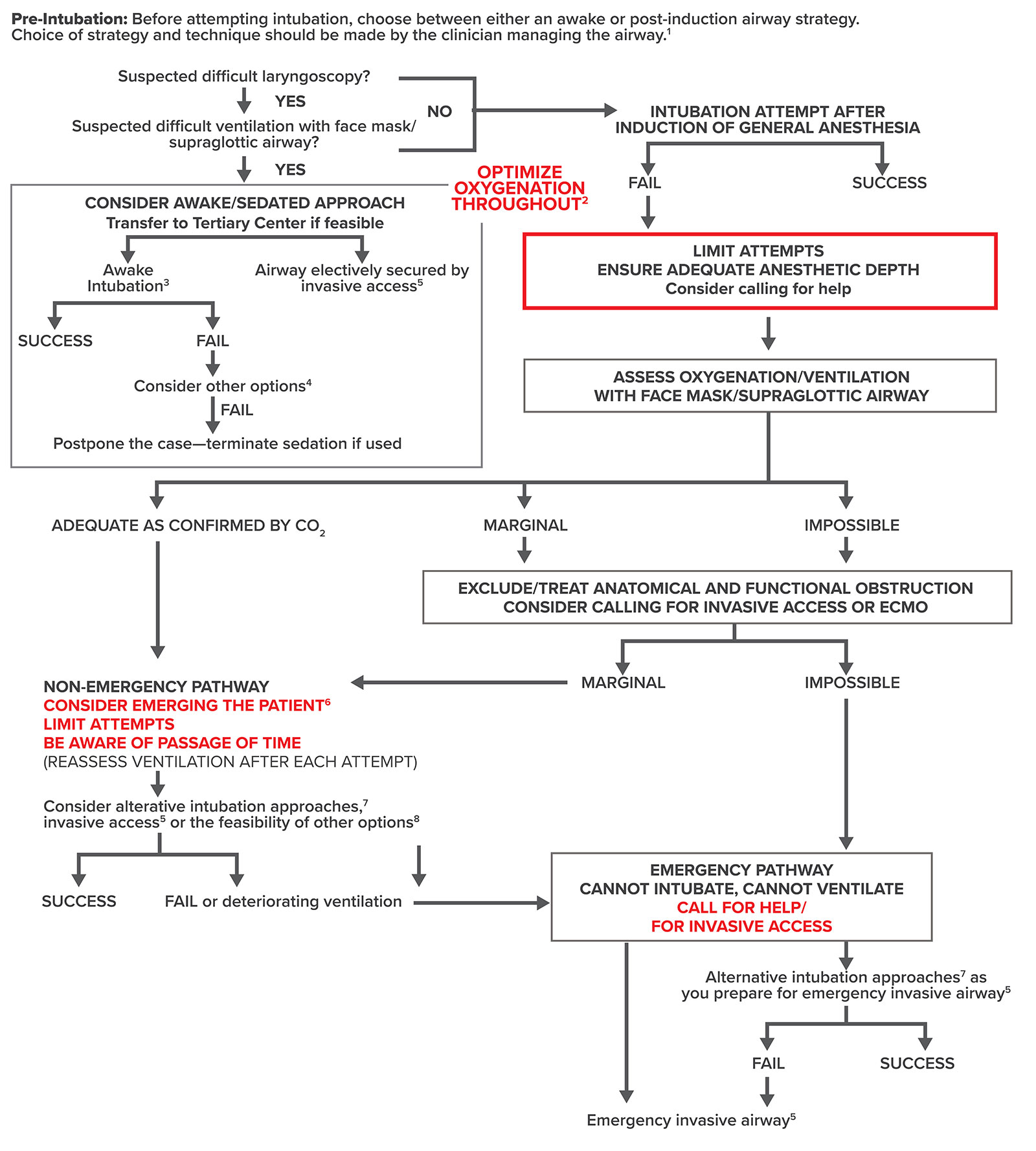
Figure 4: ASA Difficult Airway Algorithm: Pediatric Patients.
Figure 4. Difficult airway algorithm: Pediatric patients. 1. The airway manager’s assessment and choice of techniques should be based on their previous experience; available resources, including equipment, availability, and competency of help; and the context in which airway management will occur. 2. Low- or high-flow nasal cannula, head elevated position throughout procedure. Noninvasive ventilation during preoxygenation. 3. Awake intubation techniques include flexible bronchoscope, videolaryngoscopy, direct laryngoscopy, combined techniques, and retrogradewire-aided intubation. 4. Other options include, but are not limited to, alternative awake technique, awake elective invasive airway, alternative anesthetic techniques, induction of anesthesia (if unstable or cannot be postponed) with preparations for emergency invasive airway, or postponing the case without attempting the above options. 5. Invasive airway techniques include surgical cricothyroidotomy, needle cricothyroidotomy if age-appropriate with a pressure-regulated device, large-bore cannula cricothyroidotomy, or surgical tracheostomy. Elective invasive airway techniques include the above and retrograde wire–guided intubation and percutaneous tracheostomy. Also consider rigid bronchoscopy and ECMO. 6. Includes postponing the case or postponing the intubation and returning with appropriate resources (e.g., personnel, equipment, patient preparation, awake intubation). 7. Alternative difficult intubation approaches include, but are not limited to, video-assisted laryngoscopy, alternative laryngoscope blades, combined techniques, intubating supraglottic airway (with or without flexible bronchoscopic guidance), flexible bronchoscopy, introducer, and lighted stylet. Adjuncts that may be employed during intubation attempts include tracheal tube introducers, rigid stylets, intubating stylets, or tube changers and external laryngeal manipulation. 8. Other options include, but are not limited to, proceeding with procedure utilizing face mask or supraglottic airway ventilation. Pursuit of these options usually implies that ventilation will not be problematic.
Developed in collaboration with the Society for Pediatric Anesthesia and the Pediatric Difficult Intubation Collaborative: John E. Fiadjoe, MD; Thomas Engelhardt, MD, PhD, FRCA; Nicola Disma, MD; Narasimhan Jagannathan, MD, MBA; Britta S. von Ungern-Sternberg, MD, P.D, DEAA, FANZCA; and Pete G. Kovatsis, MD, FAAP.
Conclusions
These new guidelines are the first to include evidence from both adults and pediatric airway management. Although cloaked in the same garments (style, process and format) they radically depart from previous versions. They highlight the importance of risk assessment, provide a new decision tree to help determine when to consider awake airway management, awareness of task fixation and time passage, limiting the number of tracheal intubation attempts, and assessing ventilation after every intervention. Finally, they highlight the need to confirm intubation with capnography, plan for extubation, document the airway management in the medical record, and provide documentation to the patient. Welcome to the final stage of change.
John Fiadjoe, MD, is executive vice chairman in the Department of Anesthesiology, Critical Care and Pain Medicine at Boston Children’s Hospital, Boston, MA.
David Mercier, MD, is an associate professor at the University of Texas Southwestern Department of Anesthesiology and Pain Management in Dallas, TX.
John Fiadjoe, MD, received an APSF Grant in the past. David Mercier, MD, has no conflicts of interest.
References
- Apfelbaum JL, Hagberg CA, Connis RT, et al. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology. 2022; 136:31–81. 34762729. Accessed April 22, 2022.
- Cook TM, Woodall N, Frerk C. Fourth National Audit Project. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia. Br J Anaesth. 2011;106:617–631. 21447488. Accessed April 22, 2022.
- Joffe AM, Aziz MF, Posner KL, et al. Management of difficult tracheal intubation: a closed claims analysis. Anesthesiology. 2019;131:818–829. 31584884. Accessed April 22, 2022.
- Rosenblatt WH. The Airway Approach Algorithm: a decision tree for organizing preoperative airway information. J Clin Anesth. 2004;16:312–316. 15261328. Accessed April 22, 2022.
- Aziz MF, Dillman D, Fu R, et al. Comparative effectiveness of the C-MAC video laryngoscope versus direct laryngoscopy in the setting of the predicted difficult airway. Anesthesiology. 2012;116:629–636. 22261795. Accessed April 22, 2022.
- Ali QE, Amir SH, Ahmed S. A comparative evaluation of King Vision video laryngoscope (channelled blade), McCoy, and Macintosh laryngoscopes for tracheal intubation in patients with immobilized cervical spine. Sri Lankan J Anaesthesiol. 2017;25:70. https://slja.sljol.info/articles/abstract/10.4038/slja.v25i2.8200/. Accessed April 22, 2022.
- Cordovani D, Russell T, Wee W, et al. Measurement of forces applied using a Macintosh direct laryngoscope compared with a Glidescope video laryngoscope in patients with predictors of difficult laryngoscopy: a randomised controlled trial. Eur J Anaesthesiol. 2019;36:221–226. 30308524. Accessed April 22, 2022.
- Gupta N, Rath GP, Prabhakar H. Clinical evaluation of C-MAC videolaryngoscope with or without use of stylet for endotracheal intubation in patients with cervical spine immobilization. J Anesth. 2013;27:663–670. 23475442. Accessed April 22, 2022.
- Hazarika H, Saxena A, Meshram P, Kumar Bhargava A: A randomized controlled trial comparing C-MAC D Blade and Macintosh laryngoscope for nasotracheal intubation in patients undergoing surgeries for head and neck cancer. Saudi J Anaesth. 2018; 12:35–41. 29416454. Accessed April 22, 2022.
- Jungbauer A, Schumann M, Brunkhorst V, et al. Expected difficult tracheal intubation: a prospective comparison of direct laryngoscopy and video laryngoscopy in 200 patients. Br J Anaesth. 2009;102:546–550. 19233881. Accessed April 22, 2022.
- Liu L, Yue H, Li J. Comparison of three tracheal intubation techniques in thyroid tumor patients with a difficult airway: a randomized controlled trial. Med Princ Pract. 2014;23:448–452. 25171459. Accessed April 22, 2022.
- Malik MA, Subramaniam R, Maharaj CH, et al. Randomized controlled trial of the Pentax AWS, Glidescope, and Macintosh laryngoscopes in predicted difficult intubation. Br J Anaesth. 2009; 103:761–768. 19783539. Accessed April 22, 2022.
- Serocki G, Bein B, Scholz J, et al. Management of the predicted difficult airway: a comparison of conventional blade laryngoscopy with video-assisted blade laryngoscopy and the GlideScope. Eur J Anaesthesiol. 2010;27:24–30. 19809328. Accessed April 22, 2022.
- Serocki G, Neumann T, Scharf E, et al. Indirect videolaryngoscopy with C-MAC D-Blade and GlideScope: a randomized, controlled comparison in patients with suspected difficult airways. Minerva Anestesiol. 2013;79:121–129. 23032922. Accessed April 22, 2022.
- Zhu H, Liu J, Suo L, et al. A randomized controlled comparison of non-channeled King Vision, McGrath MAC video laryngoscope and Macintosh direct laryngoscope for nasotracheal intubation in patients with predicted difficult intubations. BMC Anesthesiol. 2019;19:166. 31470814. Accessed April 22, 2022.
- Bhatnagar S, Mishra S, Jha RR, et al. The LMA Fastrach facilitates fibreoptic intubation in oral cancer patients. Can J Anaesth. 2005;52:641–645. 15983153. Accessed April 22, 2022.
- Hanna SF, Mikat-Stevens M, Loo J, et al. Awake tracheal intubation in anticipated difficult airways: LMA Fastrach vs. flexible bronchoscope: a pilot study. J Clin Anesth. 2017; 37:31–37. 28235524. Accessed April 22, 2022.
- Langeron O, Semjen F, Bourgain JL, et al. Comparison of the intubating laryngeal mask airway with the fiberoptic intubation in anticipated difficult airway management. Anesthesiology. 2001;94:968–972. 11465622. Accessed April 22, 2022.
- Shyam R, Chaudhary AK, Sachan P, et al. Evaluation of Fastrach laryngeal mask airway as an alternative to fiberoptic bronchoscope to manage difficult airway: a comparative study. J Clin Diagn Res. 2017;11:UC09-12. 28274023. Accessed April 22, 2022.
