Wrong-site procedures are considered “Never Events,” but still occur at an estimated national rate of 7.5 per 10,000 procedures.1 Wrong-side nerve blocks are likely to continue to occur as multimodal anesthetic management gains popularity as a way to reduce opioid-based anesthetics. Consequently, Envision Physician Services, a national multispecialty physician group, approached Memorial Healthcare System in Hollywood, Florida, with the idea of bringing hospital staff together to develop strategies that would help avert wrong-site blocks. This led to the implementation of two new protocols: a visual confirmation with a colored bracelet of the correct side and a patient-directed timeout procedure led by the patient.
New Protocols
Envision and Memorial Healthcare System enlisted a large cross-functional team that consisted of Envision Physician Services senior leadership to provide insights from a clinical and patient care perspective. Registered nurses were also brought in to ensure that the workflow could be adopted among nursing staff.
Visual confirmation of the correct procedure location is performed by both the patient and nurse placing a bright green wristband marked with the word “yes” on the side corresponding to the surgery. The wristband can be seen from anywhere in the room and may reduce the risk of performing the procedure on the incorrect side, especially when the patient changes positions before the nerve block is administered. If a bilateral regional anesthetic is performed, such as a transverse abdominis plane (TAP) block the patient reads the script in the preoperative area and green bands are placed on both arms.
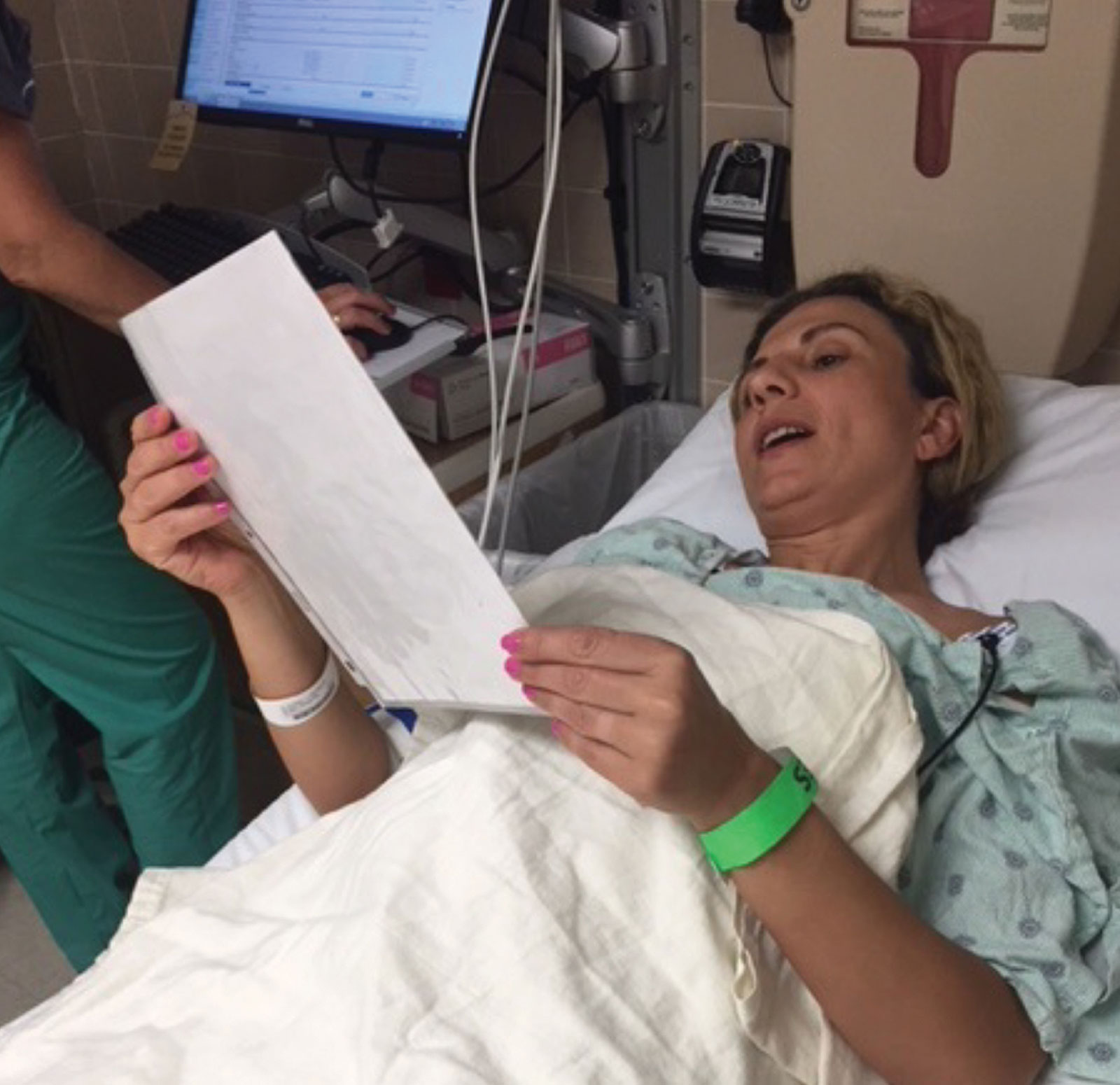
Figure 1. Depicts the patient directed timeout before a regional nerve block. Patient also wears a bright green colored bracelet to alert providers to the side on which the nerve block will be placed.
The second measure involves giving the patient a script to lead the anesthesia timeout (Figure 1). The script includes eight steps and confirms personal information such as allergies, surgery type and block location with proper identification markers. Providers from Envision and Memorial Healthcare System observed that with the patient as the leader, the timeout seems to proceed in an orderly manner, and all members of the medical team may remain focused and engaged in a consistent, thorough, and standardized timeout process. The new patient-led timeout process still incorporates all the major aspects of a timeout recommended by the Joint Commission,2 including proper documentation and conducting the timeout before the procedure is administered, involving all appropriate clinical team members, and at minimum, confirming the patient identity, procedure type, and site of the procedure.
Improved Patient Satisfaction and Safety
The team noticed that the new protocols may have helped boost satisfaction for both patients and clinicians. By becoming active participants, patients may gain a sense of empowerment and control over their care and confidence in the clinical team. The wristband also may increase clinician confidence by providing an immediate visual prior to initiation of any procedure. This has been so well received that the surgeons have started to request similar wristbands for procedures regardless of whether or not a regional anesthetic is performed.
Additionally, the patient-led timeout may safeguard against confirmation bias among the clinical team. For example, if a physician leads the timeout and asks the patient if the surgery is on the left side when it should be on the right, a nervous patient may agree, and the nurse may assume that the physician and patient identified the correct side. The script helps the care team avoid confirmation bias by using general phrases such as, “Put the wristband on the same side on which you’re having the surgery.” The patient then has ownership in their care for indicating the correct side. If a patient is unable or unwilling to lead the timeout process or is unable to verify the information, the team proceeds with the traditional timeout led by the nurse and physician. When the patient takes the lead, it may reduce provider fatigue, as the clinical team may often be rushed from doing multiple timeouts back to back, leading to shortcuts and distractions, and may reinvigorate those same health care professionals to respect the value of the “timeout.”
National Rollout
Memorial Regional Hospital South in Hollywood, Florida, piloted the innovative protocols for nearly two years, during which time more than 100 patients participated. In early 2018, Memorial Healthcare System, one of the largest public health care systems in the United States, rolled out the protocols to all six of its hospitals.
Envision Physician Services is now building on that momentum and plans to roll the procedures out to all of its anesthesia professionals in the next year as a standardized practice. These adjustments to how we approach delivering care hopefully will increase patient satisfaction, while reducing the risk of wrong-site blocks. Leadership from Envision Physician Services plans to study many of these outcomes as they apply to the implementation of the present protocol. However, the authors wish to share the cultural change and processes so other practices may start thinking about the option to introduce these initiatives.
Adam L. Blomberg, MD, is the chief of Anesthesiology for Memorial Healthcare System in Hollywood, Florida, and the regional medical director and national education director for Envision Physician Services’ Anesthesia Division. Joseph Loskove, MD, is Envision Physician Services senior vice president of Anesthesia. Cameron Howard, MD, is regional director of enhanced recovery for Memorial Healthcare System and vice chief of Anesthesia at Memorial Hospital West. David Sacks, MD, is the chief of Anesthesiology for Memorial Regional South Hospital. Dr. Blomberg and Dr. Sacks led the implementation of the pilot program at Memorial Regional South and rollout to the health system.
Dr. Blomberg, Dr. Loskove, Dr. Howard, and Dr. Sacks have no conflicts of interest to declare regarding the content in this article.
Special acknowledgment to Senior Vice President of Anesthesia Joseph Loskove, MD, and Chief Clinical Officer Gilbert Drozdow, MD, along with their colleagues Cameron Howard, MD, David Sacks, MD, and registered nurses Dionne Linton and Danielle Cammarata, who helped to create, develop and implement this protocol.
References
- Barrington, MJ, Uda, Y, Pattullo, SJ, et al. Wrong-site regional anesthesia: review and recommendations for prevention? Curr Opin Anaesthesiol 2015; 28: 670-684.
- The Joint Commission. The universal protocol for preventing wrong site, wrong procedure and wrong person surgery. Patient Safety Network; January 2003.
