INTRODUCTION
 Over 150 million peripheral intravenous catheter (PIVC) insertions occur in the United States annually, making it the most common invasive procedure performed in hospitals.1 Complications associated with PIVCs include nerve injury, vascular injury, and infiltration. Infiltration of a PIVC is the unintended administration of any medications or fluids into tissue surrounding the catheter.2,3 Infiltration occurs in approximately 13.7% of PIVC insertions and can have significant perioperative patient safety consequences.4,5 Risk factors for PIVC infiltration include both equipment and care-related factors.5-8 While most PIVC infiltration events can be managed conservatively, severe cases can result in tissue injury requiring surgical intervention, specialized wound care, persistent pain, or loss of limb function.
Over 150 million peripheral intravenous catheter (PIVC) insertions occur in the United States annually, making it the most common invasive procedure performed in hospitals.1 Complications associated with PIVCs include nerve injury, vascular injury, and infiltration. Infiltration of a PIVC is the unintended administration of any medications or fluids into tissue surrounding the catheter.2,3 Infiltration occurs in approximately 13.7% of PIVC insertions and can have significant perioperative patient safety consequences.4,5 Risk factors for PIVC infiltration include both equipment and care-related factors.5-8 While most PIVC infiltration events can be managed conservatively, severe cases can result in tissue injury requiring surgical intervention, specialized wound care, persistent pain, or loss of limb function.
In the acute perioperative setting, PIVC infiltration can introduce a unique set of complications leading to patient harm, including intraoperative awareness, failed resuscitation, or compartment syndrome. Infiltration events involving neuromuscular blocking agents (NMBAs) may occur in the inpatient or outpatient surgery setting, complicate patient care significantly, and warrant additional considerations beyond tissue injury prevention and wound care. Specifically, the infiltration of a nondepolarizing NMBA risks subsequent reabsorption and recurarization, potentially resulting in muscle weakness, respiratory insufficiency, and postoperative pulmonary complications. Patients with compromised hepatic and renal function may be at higher risk of complications from NMBA infiltration. Unfortunately, few resources from anesthesiology societies or guidelines inform the management of this complication, whether it requires escalation of care, or if more conservative treatments can be prescribed. Anesthesiology professionals may be faced with a dilemma on how to proceed while prioritizing patient safety, especially when considering discharging same day surgery patients with higher risk comorbidities.
INFILTRATION OF NEUROMUSCULAR BLOCKING AGENTS
Relatively few studies and reports describe the clinical effects of infiltrated NMBAs. Thirty years ago, Korean researchers studied the clinical effects of subcutaneously administered succinylcholine.9 They found that patients receiving equal doses of subcutaneous succinylcholine had incomplete maximum depressed twitch height and prolonged paralysis onset time, but shorter paralysis recovery time compared to intravenous (IV) administration. In contrast, inadvertent subcutaneous administration of a non-depolarizing NMBA can prolong the onset and duration of neuromuscular blockade (NMB) with significant variability, making it difficult to predict neuromuscular recovery and complicating subsequent management.10-13 The prolonged onset and duration of NMB is due to the unpredictable shifting of NMBAs from subcutaneous tissues to the central circulation. While recurarization of intravenously administered rocuronium is possible after administration of NMB reversal agents, recurarization risk is increased when rocuronium has infiltrated into the subcutaneous tissue, even in patients with normal hepatic and renal function.14,15 In published cases, this “secondary recurarization” occurred most commonly when patients were administered additional “intubating doses” of rocuronium (0.6–1.2 mg/kg of ideal body weight [IBW])) after an initial infiltrated administration (subcutaneous injection), along with suboptimal dosing of NMB reversal agents.16,17
In cases involving infiltrated rocuronium, sugammadex has been successfully utilized to reverse NMB in patients with and without renal and hepatic dysfunction.18-21 Despite these case reports, the short two-hour half-life of sugammadex and its molar 1:1 binding ratio may not always result in a reliable and sustained reversal of recurarization from infiltrated rocuronium.19 In the context of renal impairment, where the half-life of sugammadex is prolonged up to 4 hours in mild renal insufficiency and 19 hours in severe renal insufficiency, sugammadex may confer a theoretical benefit in the management of infiltrated aminosteroidal NMBAs when its binding capacity is not saturated.
MANAGEMENT OF NEUROMUSCULAR BLOCKING AGENT INFILTRATION
While no guidelines for the management of infiltrated paralytic exist, several strategies may help reduce patient harm from this complication (Figure 1). Even if its effectiveness is limited, the PIVC should be left in place and medication aspiration should be attempted. If the infiltration is recognized after anesthesia induction drugs have been administered and a non-depolarizing NMBA was used, the subsequent induction attempt through the new PIVC should consider using a reduced dose of a non-depolarizing NMBA, avoiding redosing non-depolarizing NMBA altogether, or switching to succinylcholine. Intraoperatively, the anesthesia team should elevate the extremity with the infiltration, apply warm compresses (dry heat) to facilitate systemic uptake of drugs, demarcate the area of infiltration, and consider administration of hyaluronidase through the infiltrated PIVC and intradermally around the leading edge of infiltration site.22 Serial exams should be conducted along with surgical consultation if there remains concern for tissue injury or compartment syndrome.
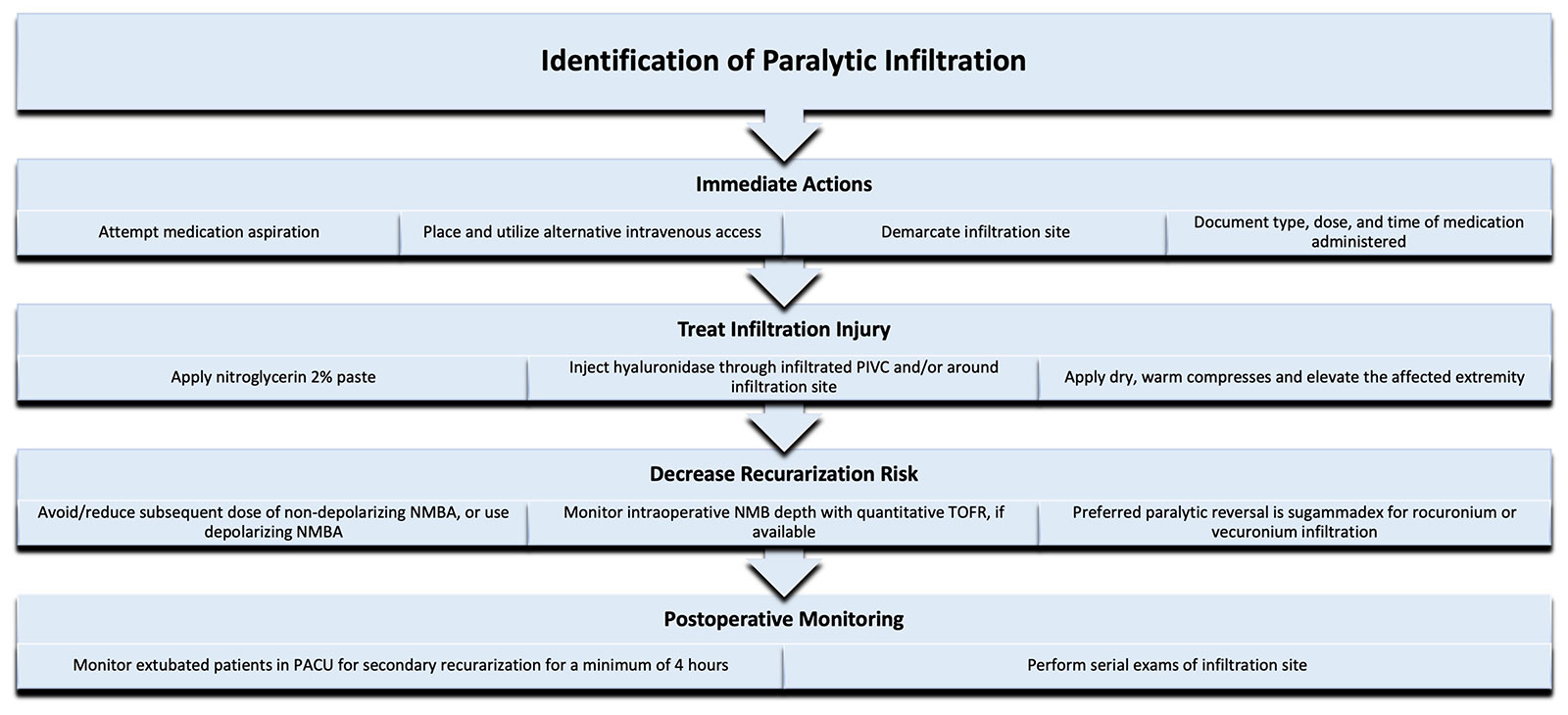
Figure 1: Authors’ proposed algorithm to manage paralytic extravasation.
Neuromuscular blocking agent (NMBA); Neuromuscular blockade (NMB); Post-anesthesia care unit (PACU); Train-of-four ratio (TOFR).
Local circulation can significantly alter the predictability of onset and duration of infiltrated rocuronium.20 Techniques to improve the systemic absorption of NMBAs may facilitate optimal NMB reversal in the immediate intraoperative period. Hyaluronidase and nitroglycerine paste have been utilized to accelerate the systemic absorption of many infiltrated medications and vesicants.23 Hyaluronidase is an enzyme that hydrolyzes hyaluronic acid to aid in the absorption and dispersal of injected agents. It is commonly used for the treatment of severe infiltration events involving pH-related and hyperosmolar vesicants. Hyaluronidase is commonly available in a 1 mL vial containing 150 units, and can be administered using a tuberculin syringe and 25-gauge (or smaller) needle. One recommended administration method is to dilute hyaluronidase to 15 units/mL and perform five 0.2 mL injections (1 mL total) around the leading edge of the infiltration site.22 Prior to the removal of the infiltrated PIVC, 15 units may be administered through the catheter and repeated every 30–60 minutes until the infiltration site resolves.22,24 The administration of hyaluronidase should occur optimally within 1 hour of the infiltration event; improvements in swelling may be observed within 15–30 minutes of enzyme delivery along the tissue plane.25 Similarly, the vasodilating effects of nitroglycerin 2% paste can improve systemic drug absorption when applied to one square inch areas of infiltration, avoiding any areas of skin breakdown.25,26
NMB reversal needs to be carefully considered. Studies on the pharmacokinetics and pharmacodynamics of subcutaneously administered steroidal NMBAs to support evidence-based NMB reversal treatments are sparse and have not included benzylisoquinoline alkaloids. Only twelve case reports/case series and one prospective study address the pharmacokinetics and pharmacodynamics of subcutaneously administered steroidal NMBAs.10-19,21,27-29 The cohort of cases reviewed included 30 patients and the NMBAs involved were pancuronium, vecuronium, and rocuronium. It is possible that the spontaneous degradation of benzylisoquinoline alkaloids at tissue pH may protect against severe complications from their reabsorption, hence the lack of infiltration reports involving this class of NMBAs. Due to the paucity of data, approaches to NMB reversal recommended in the literature are based on the availability of qualitative and quantitative monitors of NMB depth and on general pharmacokinetic and pharmacodynamic considerations, including the hepatic and renal function of patients.
After initiating treatment for infiltrated NMBA, every attempt should be made to reverse NMB, with sugammadex being the preferred agent for rocuronium and vecuronium.30 Intraoperatively, should the patient continue to have deep levels of NMB or if sugammadex is unavailable, the anesthesia professional may also elect to keep the patient intubated postoperatively. If only qualitative twitch monitoring is available or the concern for residual NMBA at the infiltration site remains, and NMB depth is mild-moderate, the anesthesia professional should use standard reversal doses and monitor the patient closely for clinical signs of recurarization in the postanesthesia care unit (PACU). If quantitative train-of-four ratio (TOFR) monitoring capabilities are available and the infiltration site looks visibly better at the end of the operation, patients may still be monitored clinically but with the added benefit of quantitative TOFR data to guide reversal redosing. Previous studies have used stimulation currents of 50 milliamperes to detect residual paralysis in patients in the PACU, but reducing the stimulation current amplitude to below 40 milliamperes using a newer commercially available electromyography-based quantitative TOFR monitor can significantly reduce discomfort in non-sedated patients without compromising TOFR accuracy.31 Due to the lack of predictability of subcutaneously injected paralytic absorption, extubated patients without hepatic or renal dysfunction should be monitored for at least four hours in the PACU.12,13,19,20 Both the patient and nursing teams should receive counseling on the signs and symptoms of residual NMB with parameters to guide care escalation.
CONCLUSION
Infiltration events can cause significant patient harm and complicate patient care in the perioperative period. Should NMBA infiltration occur, the anesthesia professional is presented with the challenge of not only managing potential patient injuries but also preventing secondary recurarization from the unpredictable reabsorption of NMBA from the subcutaneous depot. Anesthesiology professionals should remain aware of management options to reduce adverse sequelae from this complication.
Govind Rangrass, MD, FASA, is an associate professor of anesthesiology and critical care at SSM Health Saint Louis University Hospital, Saint Louis, MO.
Karolina Brook, MD, FASA, CPPS, is an anesthesiologist in the Department of Anesthesiology at Boston Medical Center, Boston, MA, and an assistant professor in the Department of Anesthesiology, Boston University Chobanian and Avedisian School of Medicine, Boston, MA.
Rachel C. Wolfe, PharmD, MHA, BCCCP, FCCP, is a perioperative clinical pharmacy specialist at Barnes-Jewish Hospital, Saint Louis, MO.
Fenghua Li, MD, FASA, is a professor of anesthesiology at the State University of New York Upstate Medical University, Syracuse, NY.
Andrea Vannucci, MD, FASA, is a clinical professor of anesthesiology at the University of Iowa Hospitals and Clinics, Iowa City, IA.
The authors have no conflicts of interest.
REFERENCES
- Zingg W, Pittet D. Peripheral venous catheters: an under-evaluated problem. Int J Antimicrob Agents. 2009;34 Suppl 4:S38–42. PMID: 19931816.
- Gorski LA, Stranz M, Cook LS, et al. Development of an evidence-based list of noncytotoxic vesicant medications and solutions. J Infus Nurs. 2017;40:26–40. PMID: 28030480.
- Hadaway L. Infiltration and extravasation. Am J Nurs. 2007;107:64–72. PMID: 17667395.
- Barton A. Extravasation and infiltration: under-recognised complications of intravenous therapy. Br J Nurs. 2024;33:S18–S26. PMID: 38578942.
- Marsh N, Webster J, Ullman AJ, et al. Peripheral intravenous catheter non-infectious complications in adults: a systematic review and meta-analysis. J Adv Nurs. 2020;76:3346–3362. PMID: 33016412.
- Nickel B. Peripheral intravenous access: applying infusion therapy standards of practice to improve patient safety. Crit Care Nurse. 2019;39:61–71. PMID: 33016412.
- Palefski SS, Stoddard GJ. The infusion nurse and patient complication rates of peripheral-short catheters. a prospective evaluation. J Intraven Nurs. 2001;24:113–123. PMID: 11836836.
- Qin KR, Ensor N, Barnes R, et al. Standard versus long peripheral catheters for multiday IV therapy: a randomized controlled trial. Pediatrics. 2021;147:e2020000877. PMID: 33446506.
- Cho MH, Kim SI, Kim YC, et al. The neuromuscular blocking effect of subcutaneous administration of succinylcholine. Korean J Anesthesiol. 1994;27:35–39. doi:10.4097/kjae.1994.27.1.35.
- Awad N, Zalut S, Deutsch E. Successful management of subcutaneous infiltration of an intubating dose of rocuronium in a morbidly obese patient: a case report. Journal of Anaesthesia and Critical Care Reports. 2018;4:21–23. doi:10.13107/jaccr.2018.v04i02.094
- Iwasaki H, Namiki A, Omote T, Omote K. Neuromuscular effects of subcutaneous administration of pancuronium. Anesthesiology. 1992;76:1049–1051. PMID: 1599090.
- Takagi S, Kijima M, Iwasaki H, et al. Extravascular leakage of induction doses of rocuronium: four cases in which both depth of neuromuscular block and plasma concentration of rocuronium were assessed. J Clin Monit Comp. 2022;36:587–592. PMID: 33745069.
- Timmermann TN, Mongan PD, Hoefnagel AL, Braunecker S. Management of subcutaneous infiltration of rocuronium: a case report. J Clin Anesth. 2021;71:110203. PMID: 33745069.
- Nakamura T, Nagasaka H, Kazama T, et al. Postoperative recurrence of paralysis following extravascular injection of rocuronium bromide in an elderly patient with normal renal and hepatic function. Anaesthesiol Intensive Ther. 2022;54:94–96. PMID: 35266377.
- Carollo DS, White WM. Postoperative recurarization in a pediatric patient after sugammadex reversal of rocuronium-induced neuromuscular blockade: a case report. A A Pract. 2019;13:204–205. PMID: 30985317.
- Wirz Y, Bergmann I, Marti F. Secondary recurarization after accidental subcutaneous application of rocuronium: case report, review of the current literature and suggestion for clinical practice. Annals of Case Reports. 2023;8. doi:10.29011/2574-7754.101316.
- Breckenridge FLGM O, Harten J. Delayed recurarization following an accidental subcutaneous injection of rocuronium despite sugammadex reversal. Anaesthesia. 2021;76 Suppl 2:16–165. PMID: 36780926.
- Doshu-Kajiura A, Suzuki J, Suzuki T. Prolonged onset and duration of action of rocuronium after accidental subcutaneous injection in a patient with chronic renal failure—a case report. JA Clin Rep. 2021;7:18. PMID: 33638714.
- Navare SR, Garcia Medina O, Prielipp RC, Weinkauf JL. Sugammadex reversal of a large subcutaneous depot of rocuronium in a dialysis patient: a case report. A A Pract. 2019;12:375–377. PMID: 30575607.
- Nietvelt F, Van Herreweghe I, Godschalx V, Soetens F. Extravascular injection of neuromuscular blocking drugs: a systematic review of current evidence and management. Eur J Anaesthesiol. 2024;41:367–373. PMID: 38410855.
- Yi J, Zimmerman P, Chow J, et al. Abstract 812: Prolonged neuromuscular blockade in the ICU from inadvertent subcutaneous rocuronium depot. Crit Care Med. 2023;51:397. doi:10.1097/01.ccm.0000908976.31856.5d.
- Stefanos SS, Kiser TH, MacLaren R, et al. Management of noncytotoxic extravasation injuries: a focused update on medications, treatment strategies, and peripheral administration of vasopressors and hypertonic saline. Pharmacotherapy. 2023;43:321–337. PMID: 36938775.
- Ong J, Van Gerpen R. Recommendations for management of noncytotoxic vesicant extravasations. J Infus Nurs. 2020;43:319–343. PMID: 33141794.
- Perez Fidalgo JA, Garcia Fabregat L, Cervantes A, et al. Management of chemotherapy extravasation: ESMO-EONS Clinical Practice Guidelines. Ann Oncol. 2012;Suppl 7:vii167-73. PMID: 22997449.
- Reynolds PM, MacLaren R, Mueller SW, et al. Management of extravasation injuries: a focused evaluation of noncytotoxic medications. Pharmacotherapy. 2014;34:617–632. PMID: 24420913.
- Maly C, Fan KL, Rogers GF, et al. A primer on the acute management of intravenous extravasation injuries for the plastic surgeon. Plast Reconstr Surg Glob Open. 2018;6:e1743. PMID: 29876181.
- Devi UR, Balasubramanyam M, Omkarappa S, et al. Accidental subcutaneous injection of vecuronium bromide in a patient with burns. Journal of Evolution of Medical and Dental Sciences. 2014;3:11903–11906.
- Kim D-H, Kim SM, Kim J, Jeong S. Sugammadex reversal of large subcutaneous injection of rocuronium in an obese patient. Med Biol Sci Eng. 2020;3:16–19. doi:10.30579/mbse.2020.3.1.16.
- Tarmey NT, Edward AM, Eynon CA. Prolonged neuromuscular block following accidental subcutaneous injection of vecuronium. Anaesthesia. 2011;66:956–957. PMID: 21916878.
- Thilen SR, Weigel WA, Todd MM, et al. 2023 American Society of Anesthesiologists practice guidelines for monitoring and antagonism of neuromuscular blockade: a report by the American Society of Anesthesiologists Task Force on Neuromuscular Blockade. Anesthesiology. 2023;138:13–41. PMID: 36520073.
- Ozbey NB, Abdullah T, Deligoz O. Residual neuromuscular block in the postanesthesia care unit: incidence, risk factors, and effect of neuromuscular monitoring and reversal agents. Turk J Med Sci. 2022;52:1656–1664. PMID: 36422506.
