| Table of Contents |
DEAR RAPID RESPONSE:
Nihon Kohden provides miniaturized carbon dioxide (CO2) sensors for mainstream CO2 analysis in both intubated and nonintubated patients. They offer two distinct models for this purpose: the cap-ONE TG 980-P (quantitative) and the cap-ONE TG 920-P (semiquantitative), both of which feature a waveform display that is compatible with all of their monitoring systems. These sensors have been primarily designed for monitoring respiration in non-operating room settings.1
In this report, we present two clinical cases in which our ill-informed use of the semi-quantitative CO2 sensor (cap-ONE TG 920-P) during general anesthesia resulted in significant unrecognized CO2 rebreathing and subsequent respiratory acidosis. These cases highlight the importance of understanding the nuanced limitations of any monitor one uses and the need for anesthesia providers to stay informed about innovative technologies in the operating room setting.
Case 1: A 34-year-old ASA 1 patient was scheduled for an anterior cervical discectomy under general anesthesia. The Datex Ohmeda 9100c NXT workstation and a Nihon Kohden Life Scope 3562 monitor, with a cap-ONE TG920P CO2 analyzer, were used. After an ueventful intravenous induction and intubation, 5% desflurane was administered in oxygen: air mixture (1:1) with a total fresh gas flow (FGF) of 4 L/min for the first 15 minutes. Subsequently, the FGF was lowered to 0.8 L/min. The displayed CO2 level on the monitor was 34 mmHg. An hour later, the displayed CO2 value during expiration had fallen to 8 mmHg. Hemodynamic parameters remained stable. The ventilator parameters, airway pressure, and lung compliance were also normal. Upon increasing the FGF to approximately 8 L/min, the displayed CO2 value on the monitor immediately increased to approximately 33 mmHg. The displayed expired CO2 seemed to vary with the FGF, increasing with higher FGF and decreasing with low FGF (Figure 1). An arterial blood gas analysis revealed respiratory acidosis (pH 7.18; PaCO2 60 mmHg). While troubleshooting the cause of the arterial blood gas identified hypercapnia, we found that the CO2 absorbent appeared exhausted and replaced it. This normalized the displayed CO2 values and eliminated the FGF related fluctuations with alteration in FGF (Figure 2). The reason for this was not immediately evident.
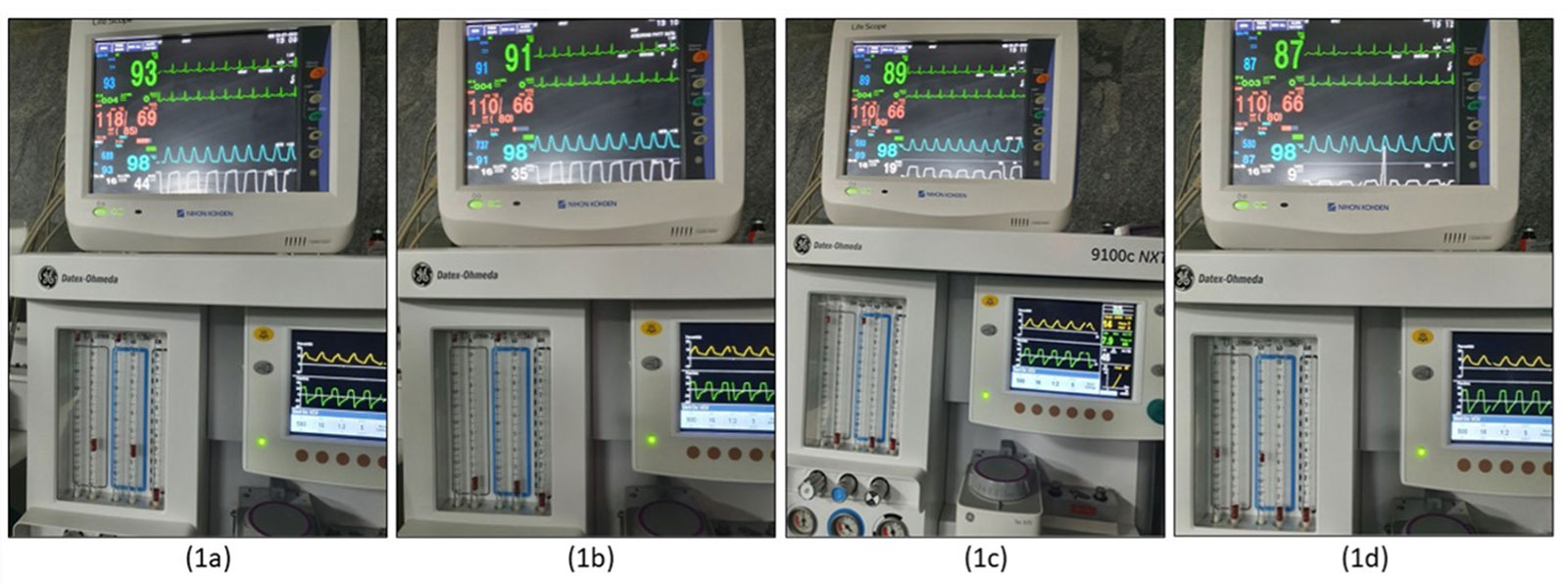
Figures 1(a) and (b) show higher expired CO2 (44 mHg and 35 mmHg) with higher fresh gas flows (8 L/min and 4 L/min, respectively). Figures 1(c) and (d) show low expired CO2 (19 mmHg and 8 mmHg) with reduced flows (1.8 L/min and 0.8 L/min, respectively).
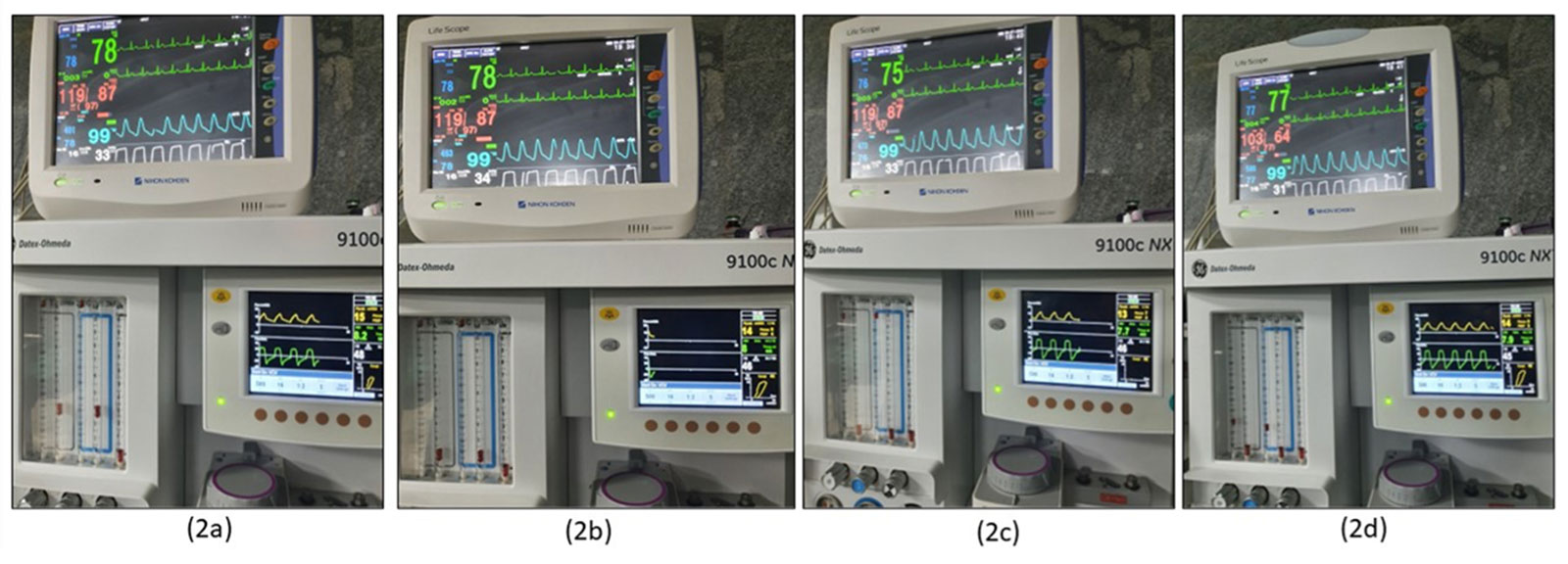
Figure 2: Figures 2(a) to 2(d) show that the variations, however, did not occur after changing the exhausted CO2 absorbent and correcting rebreathing. The images have been taken while using the same fresh gas flows as in Figure 1a.
Case 2: A 26-year-old ASA 1 patient was scheduled for septoplasty in the same operating room with the same workstation and monitor as Case 1. As with the preceding case, on initiation of low flows, the displayed expired CO2 value decreased and then on increasing the FGF, the reported ETCO2 value rose. Given our experience with the previous case, replacing the exhausted CO2 absorbent corrected this FGF related variation in the reported end tidal CO2.
Analysis of the preceding cases led us to consider the possibility of improper calibration of the CO2 analyzer, but the logic of increasing FGF increasing ETCO2 did not make sense. On further exploration, we learned that the cap-ONE Mainstream sensor (TG-920p) is fundamentally a semi-quantitative CO2 analyzer with no calibration chamber provided. It has a single CO2 sensor. It assumes that inspired air has no CO2, and irrespective of the CO2 in the inspired air, self-calibrates the inspired CO2 value to zero (Figure 1).2 These devices are designed for the intensive care unit and recovery room environments where there is no rebreathing through a semi-closed circle system as in an operating room (OR). It is also not intended for use in the setting of general anesthesia with a CO2 absorber where iCO2 monitoring is mandatory to detect rebreathing from either valve malfunction or absorbent depletion.
An institution may have several models of monitoring systems installed at various locations, and monitors may get shifted from one setting to another. Root cause analysis revealed that in our institute, the implicated CO2 sensor had been shifted from the ICU to the OR. This underscores the importance of anesthesia professional being involved in decisions regarding the suitability of monitors for each hospital location.
We encourage the manufacturer to ensure that these monitors are provided with safety tags, e.g., “Not suitable for use with rebreathing systems in the operating room during anesthesia.” Further, all safety tags supplied by the manufacturers should be tagged to the monitor. The admonition currently provided with the sensor—“With the TG-920P CO2 sensor kit (cap-ONE), measurements are based on the assumption of no CO2 gas being present on inspiration and uses zero mmHG during the calibration process. Therefore, when monitoring CO2 on a patient with an oxygen mask, CO2 gas may be present on inspiration and may result in the acquired data being lower than the actual value. It is therefore not recommended to use the cap-ONE on patients receiving oxygen by mask”3—does not make it obvious that it is not intended for use with anesthesia breathing circuits. This is aggravated by the fact that the waveform displays on a moving graph with an adjacent numerical value leading the observer to potentially mistakenly infer that the inspired CO2 value is zero.
Amrutha Bindu Nagella, MD, was an associate professor in anesthesiology, Sapthagiri Institute of Medical Sciences, Bangalore, India, when these cases were encountered. She works as a research scientist at the University at Buffalo at present.
Sripriya Ramalingam, DNB, IDRA, MANMS, is additional professor of anesthesiology at All India Institute of Medical Sciences, Mangalagiri, India.
Prabha Parthasarathy DA. MD, is professor and head of anesthesiology, Sapthagiri Institute of Medical Sciences, Bangalore, India.
Ravishankar Murugesan DA, MD, FRCP, is professor emeritus of anesthesiology, director e-learning, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidyapeeth, Pondicherry, India.
The authors have no conflicts of interest.
REFERENCES
- What is cap-ONE? [Internet]. Nihon Kohden Europe. 2017 [cited 2023 Jul 18]. Available from: https://eu.nihonkohden.com/en/innovativetechnologies/cap-one/what-is-cap-one.html. Accessed March 22, 2025.
- cap-ONE [Internet]. Nihon Kohden India. 2016 [cited 2023 Jul 18]. Available from: https://in.nihonkohden.com/en/products/patientmonitoring/capone.html. Accessed March 22, 2025.
- Capnography monitoring with the CapONE CO2 sensor. https://edutracker.com/trktrnr/Presentation/jh_newcastle_pa/N9CAPNOGRAPHY.pdf. Accessed March 22, 2025.
NIHON KOHDEN’s Response to RAPID Response Case Report on Semi-Quantitative Mainstream Carbon Dioxide Sensors in the Operating Room
DEAR RAPID RESPONSE:
Thank you for bringing your concern to our attention regarding the misuse of our TG-920P series product due to incorrect product selection in the operating room clinical setting.
Nihon Kohden’s CO2 sensor lineup includes the TG-920P, which was the subject of this report, and the TG-980P, which uses a different measurement method.
We would like to focus on the differences between the two sensors’ measurement methods, their intended uses, and the points to note.
The TG-920P series (which was the subject of this report) is a product that uses a semi-quantitative method. This does not require calibration so that in an emergent treatment and other situations, CO2 measurement can begin immediately. The measurement method is based on the premise that there is no CO2 in the inhaled air.
As there is no need for calibration, it is quick and easy to use, but, as has been reported, in cases where there is CO2 in the inhaled air, it will not be possible to measure the exact CO2 concentration. To be more specific, in respiratory circuits, like an anesthesia circuit with depleted CO2 absorption capability, or a facemask with insufficient fresh gas flow, where the inspired gas contains CO2, the displayed value will be lower than the actual CO2 concentration. A cautionary note and example of CO2 waveform with inspired CO2 is provided in the Operator’s Manual.
In contrast, the TG-980P series uses the quantitative measurement method for CO2 sensors. It can be used in settings where the inspired air may contain CO2 gas. It is designed for use in respiratory management during anesthesia, mechanical ventilation management in ICUs, and noninvasive (nonintubation) respiratory management. This measurement method uses a sensor that accurately measures CO2, including environments where inhaled air contains more CO2 gas than normally found in the atmosphere. Before use, it is necessary to perform a zero calibration of the CO2 measurement manually on the patient monitor interface. Five to six seconds is required for the calibration process before measurement can begin.
Each sensor series uses a different method to measure CO2 values. By using the most appropriate one for the situation and purpose of use in each clinical setting, one can get the most out of the performance of each product.
In addition to providing the optimal measurement method for each use situation, Nihon Kohden CO2 sensors incorporate unique technology that allows them to cope with condensation without a heater (condensation is a major factor of difficult CO2 measurement). Thus, they are also significantly smaller, lighter, and more robust than conventional mainstream sensors.
Following is a summary of use for each product series.
TG-920P SERIES
- Measurement: Employs the mainstream capnography using semi-quantitative method.
- Operation: Measures the CO2 partial pressure of expired air based on the assumption that the inspired air does not contain CO2.
- Advantage: This design eliminates the need for manual calibration, allowing for a prompt start in emergency treatment scenarios.
- Limitation: In respiratory circuits, like an anesthesia circuit with depleted CO2 absorption capability, or a facemask with insufficient fresh gas flow, where the inspired gas contains CO2, the displayed value will be lower than the actual CO2 concentrations. A cautionary note and an example of CO2 waveform are provided in the Operator’s Manual, as shown in Figure 1.
- Clinical conditions: Do not use the device when inspired air contains or may contain CO2 gas. Any inspired CO2 that might be present is not measured or reported. The device is applicable only for the inspired gas without CO2 gas.
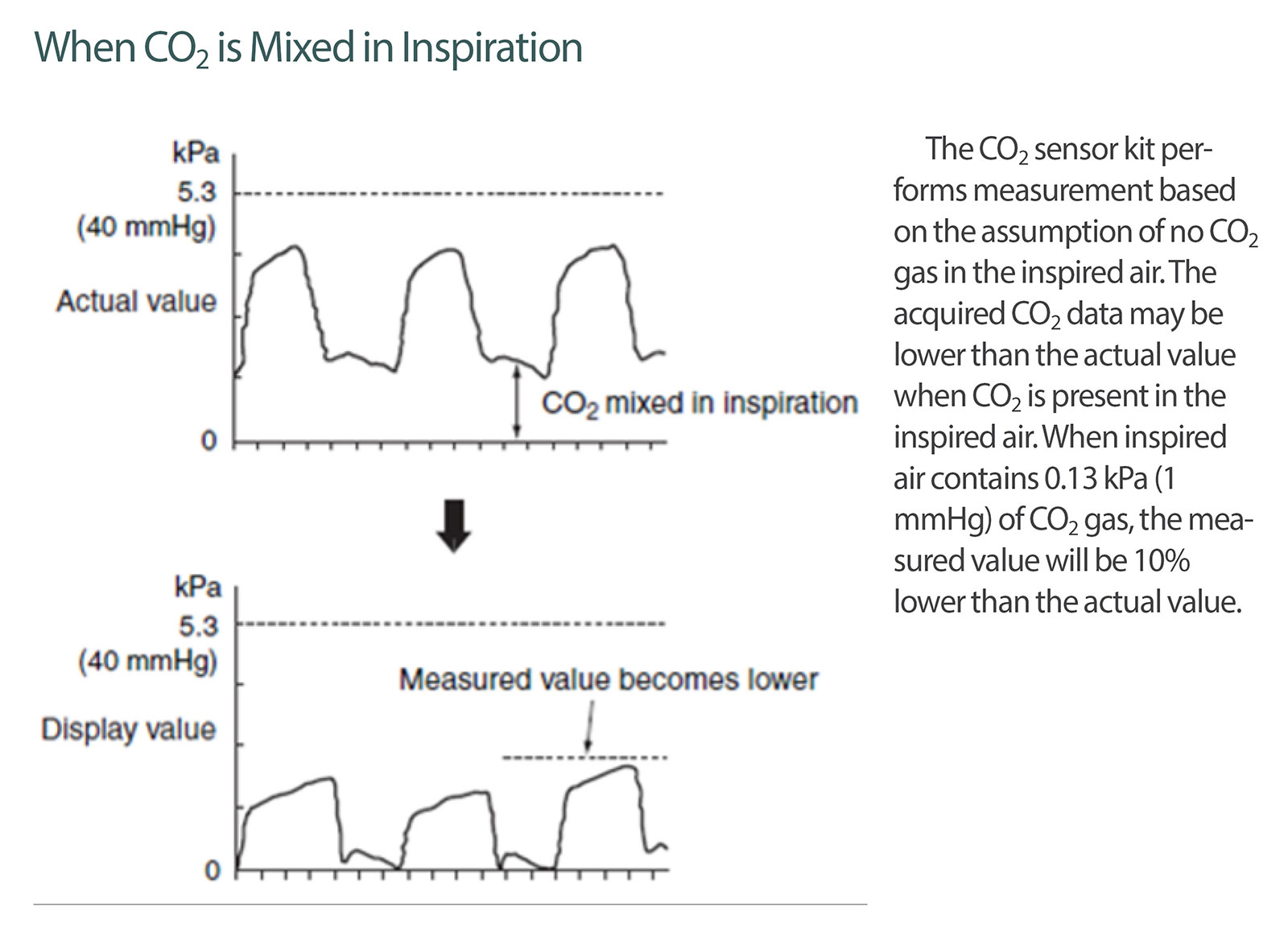
Figure 1: Note in the TG-920P Operator’s Manual: Description of the impact of CO2 gas mixing in inspired air.
Regarding the TG-920P, the reported issue is listed as a caution in the Operator’s Manual as outlined in Figure 2.
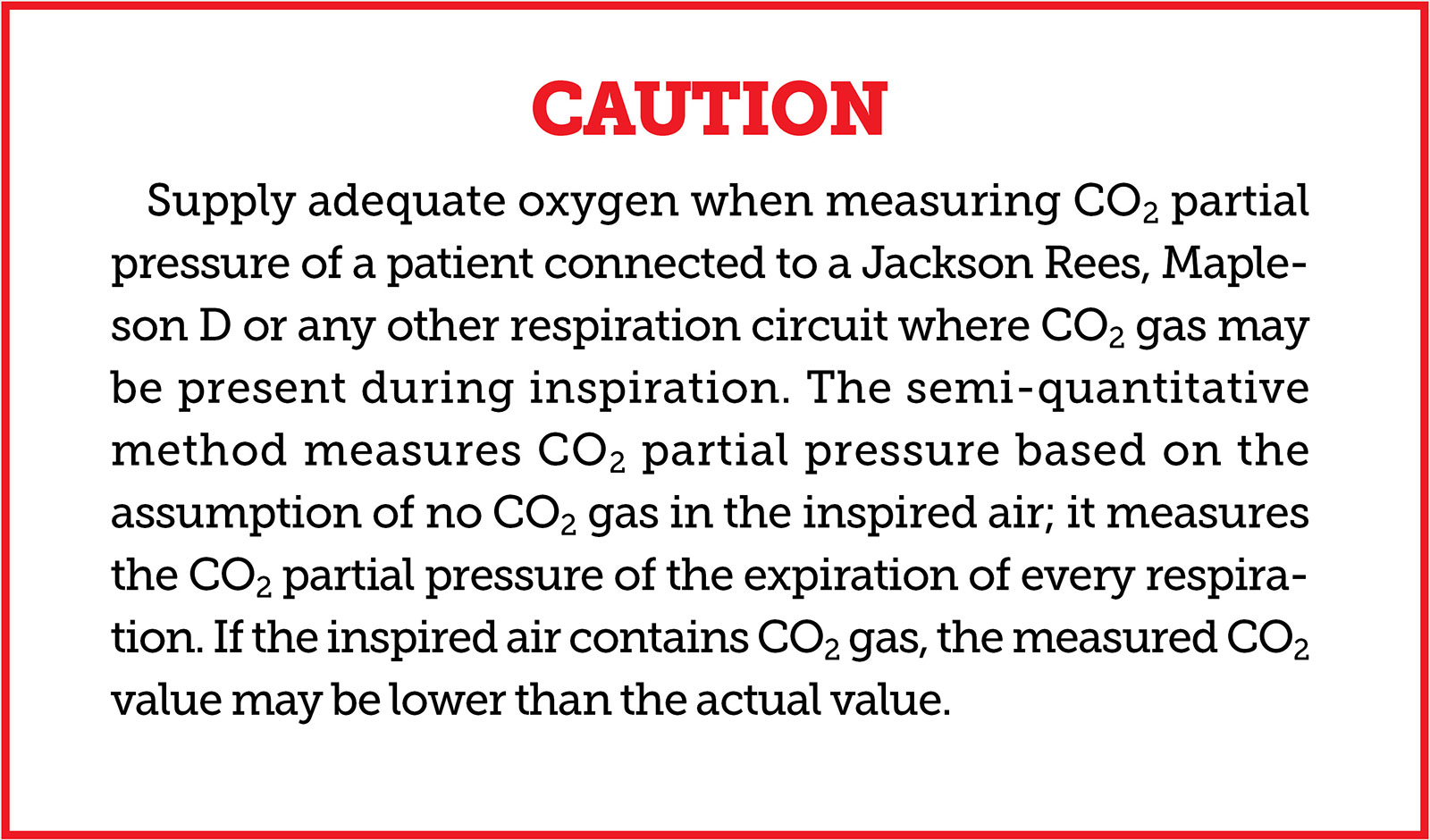
Figure 2: Caution in the TG-920P Operator’s Manual: Impact of CO2 gas mixing in inspired air to the measured CO2 value.
TG-980P SERIES
- Recommended use: Ideal for situations where the inspired air may contain CO2.
- Measurement: Employs the mainstream capnography using quantitative method with a single wave spectroscopic method, which requires manual zero calibration before use.
- Advantage: Provides a measurement of any CO2 partial pressure in the inspired air unlike the TG-920P series.
- Clinical condition: Can be used in settings where the inspired air may contain CO2 gas. The device is applicable for both inspired air with and without CO2 gas.
Nihon Kohden is dedicated to improving the labeling of our devices to more clearly indicate the appropriate product in the presence of inspired air containing CO2. As a medical device manufacturer, we will continue not only to improve our product technology on a day-to-day basis but also place a renewed emphasis on patient safety by working with anesthesia professionals on this matter in the future. Thank you for this valuable opportunity.
Sincerely,
Masao Togawa is senior manager, Safety Management Department, Quality Management System Division, Corporate Quality Management Operations, Nihon Kohden Corporation.
Maki Suezawa is senior manager, Product Quality Management Division, Corporate Quality Management Operations, Nihon Kohden Corporation.
Isao Matsubara is senior manager, Vital Sign SensorTechnology Department Division, Technology Development Operations, Nihon Kohden Corporation.
The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or group responses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intention of APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
