Pulmonary complications following major surgery are the most frequent type of postoperative complications.1 Preoperative identification of patients at higher risk for postoperative pulmonary complications is critical for minimizing risks and implementing monitoring techniques to ensure protective ventilation. The incidence of postoperative pulmonary complications has been reported to exceed 20% in patients with class III obesity (BMI ≥ 40 kg/m2) undergoing major abdominal surgery, and no standardized approach has proven effective in reducing their occurrence.2 The underlying pathophysiology of this susceptibility is linked to increased abdominal fat, which causes cephalic displacement of the diaphragm and a reduction in lung volumes, particularly functional residual capacity and expiratory reserve volume. The reduction in lung volumes is primarily responsible for the decreased respiratory system compliance observed in obesity. Moreover, supine position is associated with increased airway resistance in obese patients, likely due to breathing at low volumes, leading to flow limitation in the expiratory phase and, in some cases, intrinsic positive end expiratory pressure (PEEPi).3
According to the World Health Organization, the global prevalence of obesity is rising, with more than 40% of the U.S. population now affected.4 Mechanical ventilation for patients with obesity presents unique challenges that have become increasingly common in clinical practice. However, current ventilation strategies (Table 1) often fail to account for the specific respiratory physiology of these patients, who are frequently excluded from major randomized controlled trials.3 Obesity is associated with higher pleural pressure, reduced lung volumes, atelectasis, and increased risk of airway occlusion.5 Current intraoperative monitoring standards remain limited to basic ventilator settings (pressure, volume, and flow), which may not be sufficient in defining the best ventilation settings for these patients. These concerns become even more critical during laparoscopic and robotic-assisted procedures.
Table 1: Suggested Settings for Mechanically Ventilated Obese Patients3.
| Ventilation Mode | Volume control preferable during pneumoperitoneum and Trendelenburg Pressure control requires close monitoring of tidal volume |
| Tidal Volume | Tidal volume 6 ml/kg IBW Inspiratory time 0.6–1 s |
| Ventilation Pressures | Plateau pressure ≤ 30 cm H2O Driving pressure ≤ 15 cm H2O Higher PEEP or titrate PEEP on advanced respiratory techniques If hypoxemia consider recruitment maneuver |
| Postoperative Phase | Consider noninvasive ventilation in the postoperative period |
| Positioning | Intubate and extubate with head elevated |
| IBW: Ideal body weight. PEEP: Positive end-expiratory pressure. Driving Pressure = Plateau Pressure – PEEP | |
RESPIRATORY SYSTEM MECHANICS AND LAPAROSCOPIC SURGERY
The rising use of robotic-assisted surgeries—requiring pneumoperitoneum and, often, steep Trendelenburg position—complicates the physiologic characteristics associated with obesity. A pneumoperitoneum increases chest wall elastance, which reduces respiratory lung compliance, resulting in formation of atelectasis. Counterbalancing the increase in pleural pressure by providing positive end expiratory pressure (PEEP) is essential to avoid negative transpulmonary pressure and lung collapse.6 Loss of lung volumes leads to ventilation-perfusion mismatch and hypoxemia. The use of carbon dioxide as an insufflation agent increases the required minute ventilation. This hyperventilation in the presence of reduced lung volumes and increased chest wall rigidity can lead to heterogenous ventilation and higher driving pressure, increasing the complexity of intraoperative ventilation management.
Patients with obesity frequently experience increased driving pressures during robotic-assisted procedures, often exceeding physiological accepted values (<15 cm H2O).6 However, no advanced monitoring tools are routinely used to guide adjustments in ventilatory support. This clinical gap needs to be addressed to improve patient safety and reduce respiratory intraoperative and postoperative complications.
ADVANCED RESPIRATORY MONITORING TECHNIQUES
Esophageal manometry (Pes) and electrical impedance tomography (EIT) are advanced respiratory monitoring techniques that can be used to guide safely personalized intraoperative ventilatory support. Studies utilizing postoperative computed tomography (CT) scans have demonstrated a reduction in lung atelectasis in patients treated with intraoperative individualized PEEP.7,8 However, further research is needed to evaluate the impact of these various techniques on postoperative pulmonary complications.
ESOPHAGEAL PRESSURE MANOMETRY
The respiratory system consists of two anatomical parts: the lung and the chest wall. Airway pressure can be considered as the sum of pleural pressure and transpulmonary pressure, where transpulmonary pressure represents the true distending force on the lungs. Negative transpulmonary pressure indicates a force pushing against the alveoli, resulting in lung collapse and reduced lung volumes.
Esophageal pressure is a user-friendly surrogate of continuous pleural pressure monitoring. This technique consists of a standard naso/oro-gastric tube equipped with a small plastic balloon at the end. The catheter is inserted to position the balloon in the lower third of the esophagus, which is in close proximity to the lungs, allowing for the measurement of the pleural pressure (Figure 1). Studies have shown that Pes reliably estimates pleural pressure in adjacent lung regions, though it may overestimate pleural pressure in more ventral lung regions.9 Pes monitoring can trace the whole respiratory phase and compute real-time continuous transpulmonary pressure. This technique has been proposed to set individualized PEEP equal to Pes measured at end-expiration.10,11 Because negative transpulmonary pressure values are associated with lung collapse, Pes can guide PEEP settings by maintaining a transpulmonary pressure equal to zero at the end of expiration, thus preventing atelectasis (Figure 2).
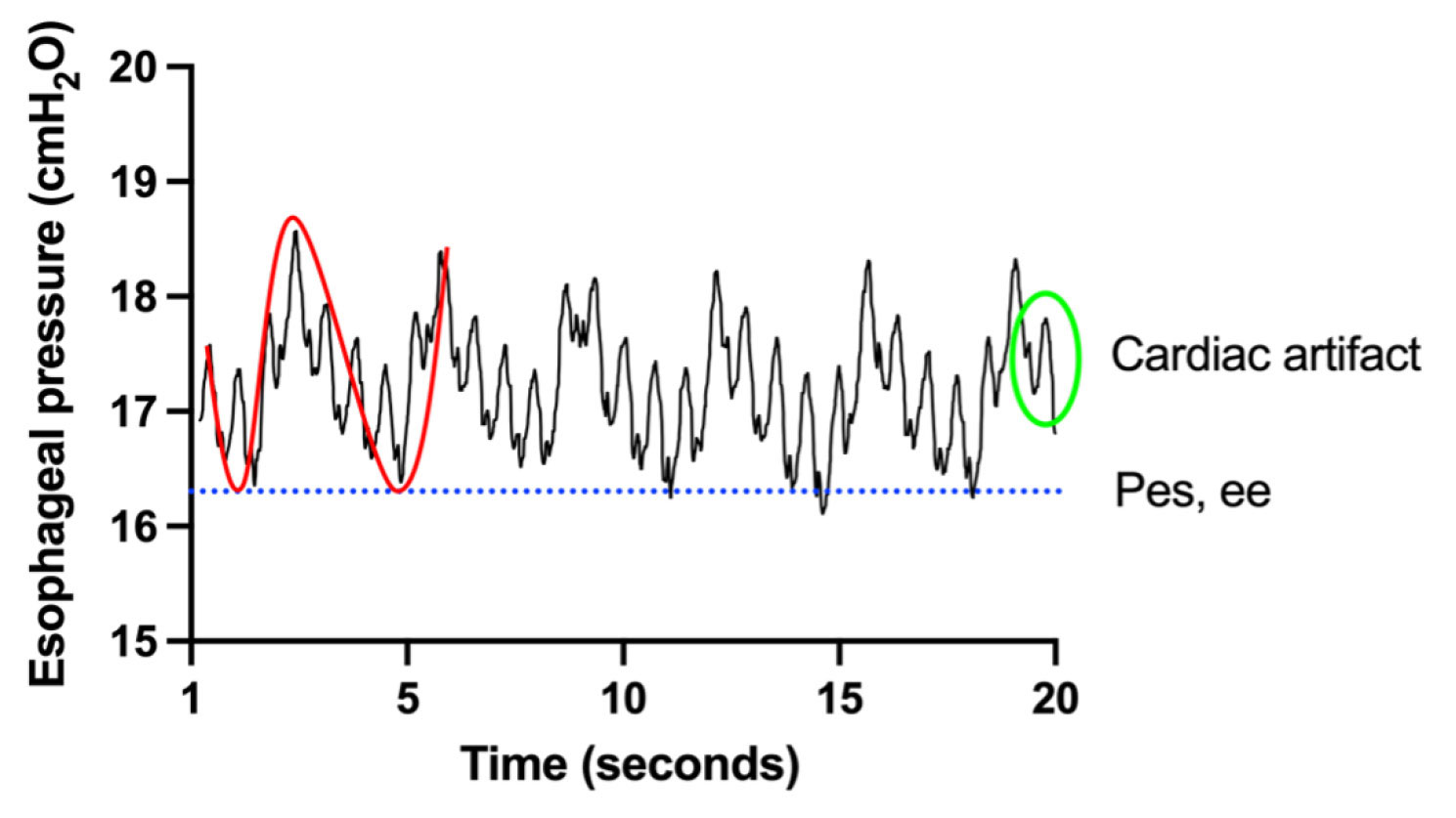
Figure 1: Esophageal pressure waveform recorded in a mechanically ventilated patient with a BMI of 67 kg/m². The red line represents the esophageal pressure trace, while the blue dotted line marks the end-expiratory esophageal pressure (Pes,ee). The green circle highlights cardiac artifacts. (Used with permission of the authors.)
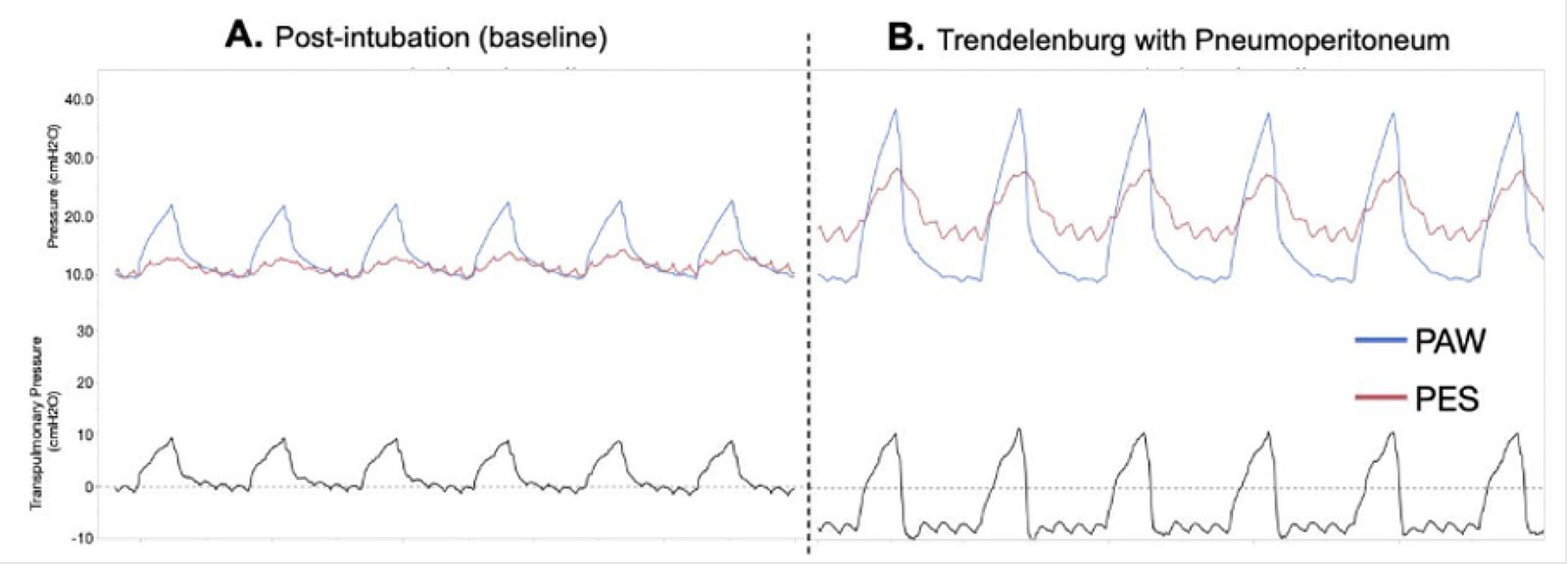
Figure 2: Esophageal pressure manometry curves recorded in a mechanically ventilated patient during a laparoscopic procedure. Panel A shows the traces for airway pressure (Paw, blue line), esophageal pressure (Pes, red line), and transpulmonary pressure (PL, grey line) after intubation in the supine position at PEEP 10 cmH₂O. Panel B shows the traces for Paw (blue line), Pes (red line), and PL (grey line) for the same patient after pneumoperitoneum and Trendelenburg positioning at PEEP 10 cmH₂O. In Panel A, Paw and Pes are similar at end-expiration, and PL equals zero at end-expiration (dotted line). After insufflation and Trendelenburg positioning, Pes exceeds Paw at end-expiration, resulting in a negative PL during expiration (dotted line), a condition associated with lung collapse. (Used with permission of the authors.)
Individuals with class III obesity and healthy lungs have been shown to have higher pleural pressure.5 Under general anesthesia, with sedation and paralysis and in absence of PEEP and lung recruitment, this tendency towards lower lung volumes and airway collapse is further exacerbated, leading to atelectasis and ventilation/perfusion mismatch if not prevented by adequate PEEP.12
Esophageal pressure monitoring has been used for decades in intensive care units (ICU) with studies demonstrating improvement in oxygenation in acute respiratory failure.13 A recent observational trial found that a transpulmonary pressure >0 was associated with a lower 60 days mortality in patients with BMI > 30kg/m2.14 Additionally, our group studied the implementation of a dedicated team consisting of experts in advanced respiratory techniques (Lung Rescue Team) at the Massachusetts General Hospital to individualize ventilation settings in patients with obesity admitted to the ICU. This study showed that individualized ventilation in patients with obesity was associated with better oxygenation, respiratory mechanics, and improved survival at 28 days, 3 months, and 1 year.15
ELECTRIC IMPEDANCE TOMOGRAPHY
Electrical impedance tomography (EIT) is an FDA-approved, radiation-free, noninvasive lung imaging technique that provides real-time visualization of regional ventilation, lung volumes, and perfusion. It measures the electrical impedance of tissues, which changes as the lungs fill with air. Electrodes positioned on a belt around the chest produce low electrical currents, and the resulting voltage differences are analyzed to be visualized in a color-coded image of air distribution across different lung regions during each breath (Figure 3).16 An important feature is the ability to evaluate regional (right versus left, anterior versus posterior) ventilation, and determine regional differences in compliance.17 EIT can also guide PEEP adjustments based on the amount of lung collapse and overdistension at different pressures, optimizing lung recruitment while minimizing the risk of overinflation and atelectasis (Figure 4). This technique has been validated in ICU patients during a decremental PEEP trial, in which EIT displays impedance changes associated with each PEEP step.18 The best PEEP is identified as the crossing point between minimum overdistension and collapse and correlates to a positive transpulmonary pressure. The use of EIT for individualized ventilation has been proposed across the entire spectrum of severity of respiratory failure, from noninvasive ventilation to intubated patients and during extracorporeal membrane oxygenation.19 The use of EIT for PEEP titration during abdominal surgery (laparoscopic or open) has been shown to reduce postoperative atelectasis, as assessed by computer tomography after extubation.8 Moreover, individualized PEEP was associated with better oxygenation and lower driving pressure during surgery, without hemodynamic complications.8
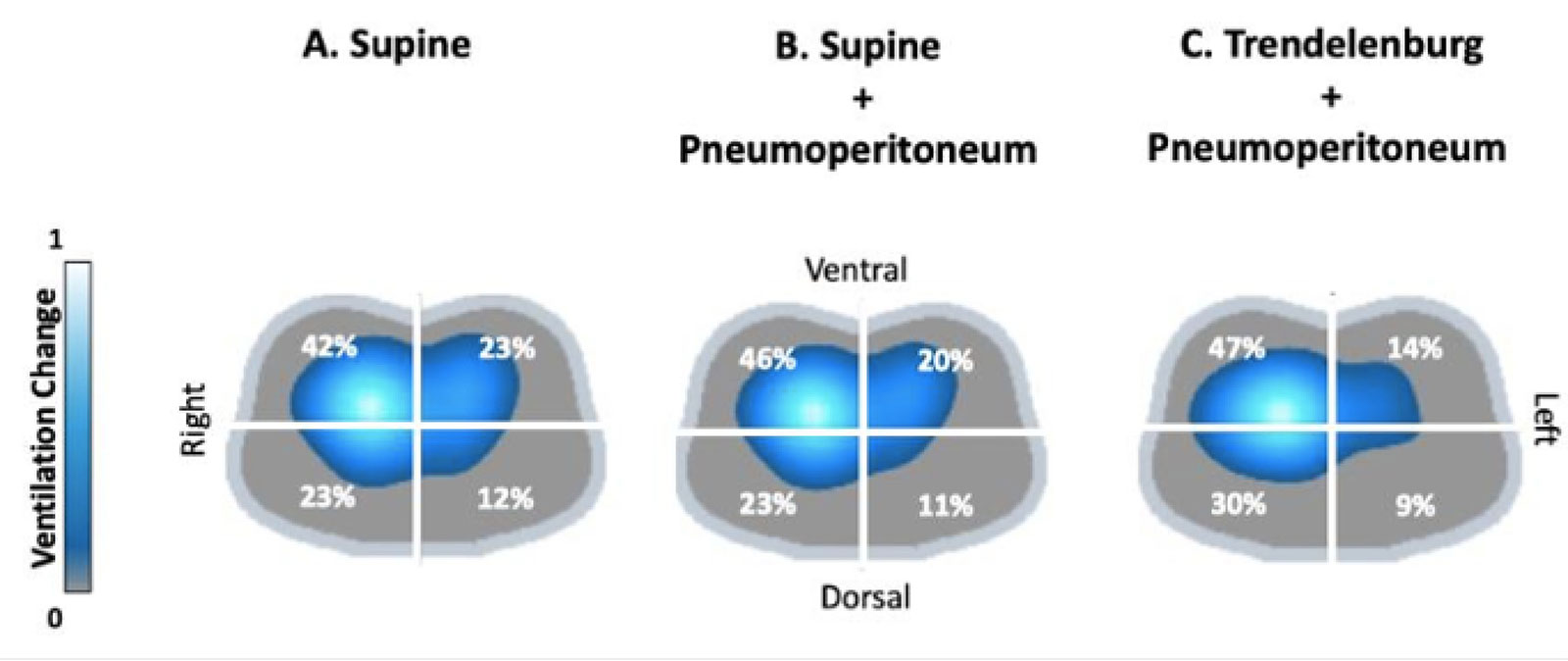
Figure 3: EIT images of ventilation distribution in the four quadrants during a robotic-assisted procedure. Panels show the changes in ventilation at the same PEEP level during three different phases of the procedure; Panel A: after intubation in supine position, Panel B during pneumoperitoneum in supine position; Panel C: during pneumoperitoneum and Trendelenburg position. (Used with permission of the authors.)
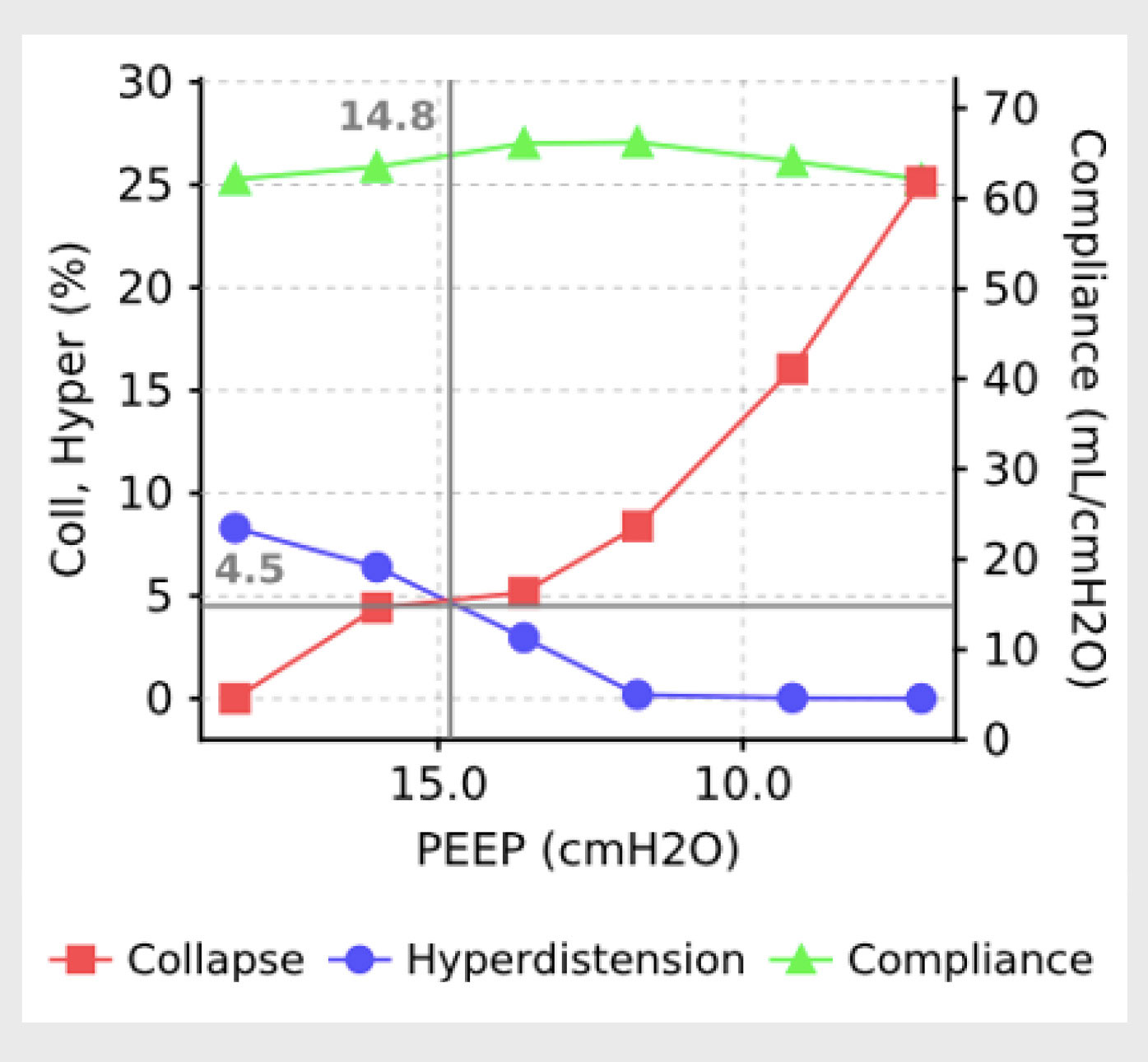
Figure 4: EIT analysis of consolidation versus overdistention curves during a decremental PEEP trial. The crossing point of the red (collapse) and blue (overdistension) lines defines the PEEP level with the lowest percentage of lung collapse and overdistension.18 (Used with permission of the authors.)
Additionally, EIT can provide dynamic lung perfusion images by detecting changes in impedance related to blood flow in the chest. This offers the potential to monitor both ventilation and perfusion in real time at the bedside, enabling a more comprehensive assessment of lung function and helping clinicians optimize ventilation/perfusion matching.
CLINICAL IMPLEMENTATION
Raising awareness of the importance of ventilator optimization and advanced respiratory monitoring during mechanical ventilation in the operating room is critical to minimize lung injury and improve respiratory outcomes in patients with obesity. Clinical, educational, and technological gaps prevent clinicians from providing safe and personalized ventilation for complex patients. A number of barriers have been identified in the process of clinical implementation of advanced respiratory techniques.20 Common barriers are lack of device availability, limited clinician education, and organizational challenges. To overcome these barriers, our Lung Rescue Team at Massachusetts General Hospital is available in the operating room.21 This multidisciplinary team with expertise in Pes and EIT can be consulted for those complex patients in whom advanced respiratory monitoring may be beneficial. The project is accompanied by the development of an educational curriculum to teach residents and clinicians in providing such techniques.
CONCLUSIONS
Providing mechanical ventilation for obese patients undergoing operating room procedures is often challenging. Advanced monitoring techniques such as Pes and EIT can provide important data to individualize the mechanical ventilation support, minimizing lung injury, and prevent postoperative atelectasis. Consequently, the traditional “one-size-fits-all” approach should be replaced by strategies tailored to adapt respiratory management for individual differences, which can improve patient outcomes. Addressing the clinical and educational gaps surrounding personalized ventilation is critical to reduce respiratory complications in this vulnerable population. By overcoming implementation barriers, we can promote the widespread adoption of advanced respiratory therapies in anesthesia practice.
Cristina Mietto, MD, Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital. Harvard Medical School, Boston, MA.
Roberta Santiago, RRT, MD, PhD, Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital. Harvard Medical School, Boston, MA. Respiratory Care Services, Massachusetts General Hospital, Boston, MA.
Lorenzo Berra, MD, Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital. Reginald Jenney associate professor, Harvard Medical School, Boston, MA; Respiratory Care Services, Massachusetts General Hospital, Boston, MA.
The authors have no conflicts of interest.
REFERENCES
- Shander A, Fleisher LA, Barie PS, et al. Clinical and economic burden of postoperative pulmonary complications: patient safety summit on definition, risk-reducing interventions, and preventive strategies. Crit Care Med. 2011;39:2163–2172. PMID: 21572323.
- Bluth T, Neto AS, et al. Effect of intraoperative high positive end-expiratory pressure (PEEP) with recruitment maneuvers vs. low PEEP on postoperative pulmonary complications in obese patients. JAMA. 2019;321:2292–2305. PMID: 31157366.
- Grassi L, Kacmarek R, Berra L. Ventilatory mechanics in the patient with obesity. Anesthesiology. 2020;132:1246–1256. PMID: 32011342.
- Adult Obesity Prevalence Maps. U.S. Dept of Health and Human Services. [Internet]. 2023; Available from: https://www.cdc.gov/obesity/data-and-statistics/adult-obesity-prevalence-maps.html. Accessed March 30, 2025.
- Florio G, Santiago RRDS, Fumagalli J, et al. Pleural pressure targeted positive airway pressure improves cardiopulmonary function in spontaneously breathing patients with obesity. Chest. 2021;159:2373–2383. PMID: 34099131.
- Tharp WG, Murphy S, Breidenstein MW, et al. Body habitus and dynamic surgical conditions independently impair pulmonary mechanics during robotic-assisted laparoscopic surgery. Anesthesiology. 2020;133:750–763. PMID: 32675698.
- Ma X, Fu Y, Piao X, et al. Individualised positive end-expiratory pressure titrated intra-operatively by electrical impedance tomography optimises pulmonary mechanics and reduces postoperative atelectasis. Eur J Anaesthesiol. 2023;40:805–816. PMID: 37789753.
- Pereira SM, Tucci MR, Morais CCA, et al. Individual positive end-expiratory pressure settings optimize intraoperative mechanical ventilation and reduce postoperative atelectasis. Anesthesiology. 2018;129:1070–1081. PMID: 30260897.
- Yoshida T, Amato MBP, Grieco DL, et al. Esophageal manometry and regional transpulmonary pressure in lung injury. Am J Respir Crit Care Med. 2018;197:1018–1026. PMID: 29323931.
- Mauri T, Yoshida T, Bellani G, et al. Esophageal and transpulmonary pressure in the clinical setting: meaning, usefulness and perspectives. Intensiv Care Med. 2016;42:1360–1973. PMID: 27334266.
- Daniel T, Todd S, Atul M, et al. Mechanical ventilation guided by esophageal pressure in acute lung injury. N Engl J Med. 2008;359:2095–2104. PMID: 19001507.
- Sprung J, Whalley DG, Falcone T, et al. The impact of morbid obesity, pneumoperitoneum, and posture on respiratory system mechanics and oxygenation during laparoscopy. Anesth Analg. 2002;94:1345–1350. PMID: 11973218.
- Ball L, Talmor D, Pelosi P. Transpulmonary pressure monitoring in critically ill patients: pros and cons. Crit Care. 2024;28:177. PMID: 38796447.
- Chen L, Grieco DL, Beloncle F, et al. Partition of respiratory mechanics in patients with acute respiratory distress syndrome and association with outcome: a multicentre clinical study. Intensiv Care Med. 2022;48:888–898. PMID: 35670818.
- Florio G, Ferrari M, Bittner EA, et al. A lung rescue team improves survival in obesity with acute respiratory distress syndrome. Crit Care. 2020;24:4. PMID: 31937345.
- Santiago RRDS, Xin Y, Gaulton TG, et al. Lung imaging acquisition with electrical impedance tomography: tackling common pitfalls. Anesthesiology. 2023;139:329–341. PMID: 37402247.
- Roldán R, Rodriguez S, Barriga F, et al. Sequential lateral positioning as a new lung recruitment maneuver: an exploratory study in early mechanically ventilated Covid-19 ARDS patients. Ann Intensiv Care. 2022;12:13. PMID: 35150355.
- Costa ELV, Borges JB, Melo A, et al. Bedside estimation of recruitable alveolar collapse and hyperdistension by electrical impedance tomography. Intensiv Care Med. 2009;35:1132–1137. PMID: 19255741.
- Franchineau G, Bréchot N, Lebreton G, et al. Bedside contribution of electrical impedance tomography to setting positive end-expiratory pressure for extracorporeal membrane oxygenation–treated patients with severe acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;196:447–457. PMID: 28103448.
- Wisse JJ, Scaramuzzo G, Pellegrini M, et al. Clinical implementation of advanced respiratory monitoring with esophageal pressure and electrical impedance tomography: results from an international survey and focus group discussion. Intensiv Care Med Exp. 2024;12:93. PMID: 39432136.
- Spina S, Capriles M, Santiago RDS, et al. Development of a lung rescue team to improve care of subjects with refractory acute respiratory failure. Respir Care. 2020;65:420–426. PMID: 32019849.
