 Infants born at gestational age < 37 weeks are categorized as premature or preterm.1 Apnea of prematurity is defined as a respiratory pause for more than 15–20 seconds, or shorter respiratory pauses accompanied by oxygen desaturation or bradycardia (heart rate < 100 beats per minute) in premature or preterm infants.1-3 The incidence of apnea is inversely correlated with gestational age. In one study, almost all infants born at ≤ 28 weeks gestation were diagnosed with recurrent apnea; this incidence decreased to 85% for infants born at 30 weeks and 20% for infants at 34 weeks gestation.4
Infants born at gestational age < 37 weeks are categorized as premature or preterm.1 Apnea of prematurity is defined as a respiratory pause for more than 15–20 seconds, or shorter respiratory pauses accompanied by oxygen desaturation or bradycardia (heart rate < 100 beats per minute) in premature or preterm infants.1-3 The incidence of apnea is inversely correlated with gestational age. In one study, almost all infants born at ≤ 28 weeks gestation were diagnosed with recurrent apnea; this incidence decreased to 85% for infants born at 30 weeks and 20% for infants at 34 weeks gestation.4
Preterm and former preterm infants are known to be at increased risk for postoperative apnea following emergence from anesthesia.2-3 Inconsistent definitions of apnea, desaturation, and bradycardia in previous studies make it difficult to identify the true incidence of postoperative apnea, which has resulted in differences in monitoring protocols across institutions.
POSTOPERATIVE APNEA IN THE PRETERM POPULATION
Apnea of prematurity reflects an immature development of respiratory control centers. Premature infants have underdeveloped respiratory and chemoreceptor function and are less likely to adjust to postnatal environment changes.5 Premature infants experience hypoxic ventilatory depression in which the initial increase in respiratory rate and volume in the setting of hypoxia transitions to a decline in spontaneous breathing that is sustained. In response to hypercapnia, premature infants increase ventilation by prolonging the period of expiration, but do not increase breath frequency or overall tidal volume, leading to less minute ventilation than that seen in term infants.1,6
Apnea of prematurity and postoperative apnea have a similar combination of central and obstructive pathophysiology. Studies have shown that obstructive apnea episodes often begin with upper airway obstruction that occur with the central component of mixed apnea. Premature infants are more likely to respond to airway obstruction with apnea and periodic breathing, which decreases with increasing post menstrual age (gestational age plus postnatal age).2-4 Furthermore, general anesthesia decreases upper airway tone and increases airway obstruction, contributing to the development of apnea after anesthesia. This occurs even in infants without a history of apnea.1-4 The risk factors for postoperative apnea include cardiac shunts, anemia, decreasing gestational age, hypothermia, glucose and electrolyte disturbances, and a patent ductus arteriosus.1
Premature infants are at significantly higher risk than term infants for cardiopulmonary complications in the immediate postoperative period. Most anesthesiology studies use the term postconceptual age (PCA).5 Early prospective studies in the 1990s showed that postoperative apnea can affect as many as 20–32% of otherwise healthy former-preterm infants under 60 weeks PCA receiving general anesthesia.7-10 In 1995, Coté et al. compiled data from eight studies of former preterm infants undergoing inguinal hernia repair to better characterize the incidence and risk of postoperative apnea. The authors reported a combined apnea rate of ~25%.11 Rates from contributing studies varied from 5% to 49% depending on the technique of apnea detection. Most apneas were pneumogram-diagnosed, occurring in infants <44 weeks PCA, and anemia was shown to be an independent risk factor. Similar to apnea of prematurity, the incidence of postoperative apnea in the preterm population was inversely related to the infant’s gestational age and PCA at the time of anesthesia (Figure 1). Postoperative apnea probability decreased to less than 1% at 54 weeks PCA in infants whose gestational age was 35 weeks and at 56 weeks PCA in infants whose gestational age was 32 weeks.11
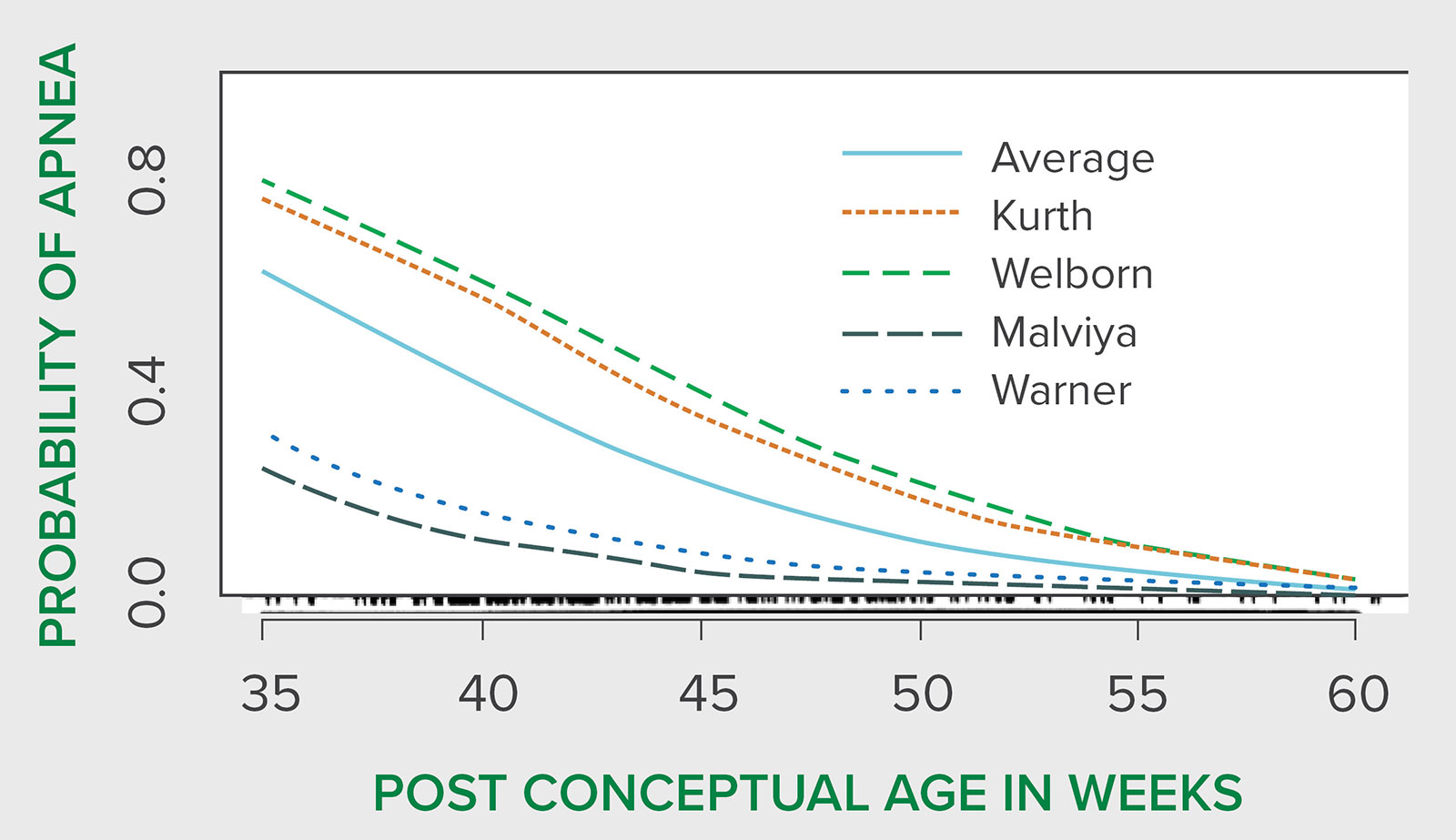
Figure 1: Predicted probability of apnea in recovery room and post-recovery room by weeks postconceptual age for all patients for each investigator. Bottom marks indicate the number of data points versus postconceptual age. The curves for the Kurth et al. and Welborn et al. studies are nearly identical in the upper range, and for the Malviya et al. and Warner et al. studies, in the lower range. There was significant institution-to-institution variability. The reasons for this are unclear but may represent differences in monitoring technology as well as patient populations, because the studies with the highest rate of apnea were also those that used continuous recording devices.
Figure from Postoperative apnea in the former preterm infants after inguinal herniorrhaphy. A combined analysis.Anesthesiology. 1995;82(4):809-822. PMID: 7717551.
Permission and rights to reuse figure without modification obtained from Wolters Kluwer.
These findings align with other reports, which showed that infants less than 45 weeks PCA were more likely to develop postoperative apnea, while in older infants with PCA between 46 and 60 weeks, comorbidities influenced their predisposition to apnea. The reported comorbidities included necrotizing enterocolitis, bronchopulmonary dysplasia, former apnea episodes, anemia, and lower birth weight.12 These findings led to a study that suggested infants between 46 and 60 weeks PCA be monitored for 12 hours postoperatively, and respiratory monitoring is recommended if the patient’s history reveals episodes of apnea, chronic lung disease, neurological disease, or anemia.13 In addition, a greater incidence of apnea within 30 minutes of surgery requiring significant interventions (maneuvers greater than tactile stimulation) was identified in infants who received general anesthesia, but no difference in the incidence of late apnea in infants who received regional versus general anesthesia.14
TIMING OF POSTOPERATIVE APNEA
Previous studies found that in the majority of infants who experienced postoperative apnea, the first event occurred within 2 hours of surgery. Yet, some authors have reported the first apneic event to occur as late as 12 hours after surgery.15-18 In a study that monitored children for 24 hours postoperatively for apnea, none of the 91 infants examined had their first apnea event after 12 hours.19 Thus, they recommended cardiorespiratory (respiratory impedance and electrocardiography) monitoring for former preterm infants for at least 12 hours after surgery. Rarely, infants have been reported to experience recurrent apneas up to 72 hours postoperatively, suggesting that even longer periods of postoperative monitoring may be required in certain cases.12,20
Most pediatric surgery centers have policies regarding postoperative admission and observation criteria for former preterm and term infants. Due to the variability in available data on gestational age, PCA, incidence, and timing of apnea events, there are nuanced differences in these policies (Table 1).6,12-14,24
Table 1: Postoperative Admission and Observation Recommendations6,13-15,24
| General Recommendations based on current available literature: Patients who are term or preterm/former preterm under 60 weeks PCA should be considered for postoperative monitoring and an observation period.13-15 Monitoring: Apnea and bradycardia monitoring, nursing observation, continuous pulse oximetry, and a respiratory monitor are recommended. |
|
| Preterm Recommendations: | Term Recommendations: |
|
|
The current available literature suggests that while there is variability across studies, a 12-hour apnea-free period currently appears to be a reasonably safe option in determining discharge in former preterm infants at risk for apnea after any anesthetic. However, a detailed analysis from a larger data set is warranted. Importantly, spinal or caudal anesthesia offers reduction in occurrence of early, but not late apnea. This is likely due to residual depressent effects of the general anesthetics.
Although most pediatric surgical centers have established policies regarding admission criteria after any anesthetic for young term and former preterm infants, policies vary from one institution to another. This variability can be partly attributed to small sample sizes and variable incidences of postoperative apnea among early studies. Data are currently being compiled and the results from a meta-analysis and micro-analysis are underway. We hope that new recommendations in the postoperative management of this vulnerable cohort will be forthcoming.
Ying Eva Lu-Boettcher, MD, FASA, is an assistant professor in the Department of Anesthesiology at the University of Wisconsin School of Medicine and Public Health, Madison, WI.
Rahul Koka, MD, MPH, is an assistant professor in the Department of Anesthesiology and Critical Care Medicine at the Johns Hopkins University School of Medicine, Baltimore, MD.
Priti G. Dalal, MD, is a professor at Penn State Health Children’s Hospital and Penn State College of Medicine
Charles J. Coté, MD, is a professor emeritus of anesthesia in the Division of Pediatric Anesthesia at the Harvard Medical School, Massachusetts General Hospital for Children.
Acknowledgements: We thank Megha Kanjia, Rahul Baijal, and Shobha Malviya for their valuable input in reviewing the manuscript.
The authors have no conflicts of interest.
REFERENCES
- Zhao J, Gonzalez F, Mu D. Apnea of prematurity: from cause to treatment. Eur J Pediatr. 2011;170:1097–1105. Epub 2011 Feb 8. PMID: 21301866.
- Eichenwald EC; Committee on Fetus and Newborn, American Academy of Pediatrics. Apnea of prematurity. Pediatrics. 2016;137(1). PMID: 26628729.
- Erickson G, Dobson NR, Hunt CE. Immature control of breathing and apnea of prematurity: the known and unknown. J Perinatol. 2021;41:2111–2123. PMID: 33712716.
- Henderson-Smart DJ. The effect of gestational age on the incidence and duration of recurrent apnoea in newborn babies. Aust Paediatr J. 1981;17:273–276. PMID: 33712716.
- Martin RJ, Miller MJ, Carlo WA. Pathogenesis of apnea in preterm infants. J Pediatr. 1986;109:733–741. PMID: 3095518.
- Engle WA. Age terminology during the perinatal period. Pediatrics. 2004;114:1362–1364. (In Eng). PMID: 15520122.
- Welborn HO, Hannallah RS, Luban NLC, et al. Anemia and postoperative apnea in former preterm infants. Anesthesiology. 1991;74:1003–1006. PMID: 2042754.
- Welborn LO, Rice LJ, Hannallah RS, et al. Postoperative apnea in former preterm infants: prospective comparison of spinal and general anesthesia. Anesthesiology. 1990; 72:838–842. PMID: 2187377.
- Kurth CD, LeBard SE. Association of postoperative apnea, airway obstruction, and hypoxaemia in former premature infants. Anesthesiology. 1991;75:22–26. PMID: 2064055.
- Sims C, Johnson CM. Postoperative apnoea in infants. Anaesth Intensive Care. 1994;22:40–45. PMID: 8160948.
- Coté CJ, Zaslavsky A, Downes JJ, et al. Postoperative apnea in former preterm infants after inguinal herniorrhaphy. A combined analysis. Anesthesiology. 1995;82:809–822. PMID: 7717551.
- Ozdemir T, Arıkan A. Postoperative apnea after inguinal hernia repair in formerly premature infants: impacts of gestational age, postconceptional age and comorbidities. Pediatr Surg Int. 2013;29:801–804. PMID: 23780479.
- Walther-Larsen S, Rasmussen LS. The former preterm infant and risk of post-operative apnoea: recommendations for management. Acta Anaesthesiol Scand. 2006;50:888–893. PMID: 16879474.
- Davidson AJ, Morton NS, Arnup SJ, et al. Apnea after awake regional and general anesthesia in infants: the general anesthesia compared to spinal anesthesia study—comparing apnea and neurodevelopmental outcomes, a randomized controlled trial. Anesthesiology. 2015;123:38–54. PMID: 26001033.
- Watcha MF, Thach BT, Gunter JB. Postoperative apnea after caudal anesthesia in an ex-premature infant. Anesthesiology. 1989;71:613–615. PMID: 2802223.
- Fellmann C, Gerber AC, Weiss M. Apnoea in a former preterm infant after caudal bupivacaine with clonidine for inguinal herniorrhaphy. Paediatr Anaesth. 2002;12:637–640. PMID: 12358663.
- Bell C, Dubose R, Seashore J, Touloukian R, et al. Infant apnea detection after herniorrhapy. Anesthesiology. 1991; 75:AI047. PMID: 7669312.
- Kurth CD, Spitzer AR, Broennle AM, et al. Postoperative apnea in preterm infants. Anesthesiology. 1987;66:483–488. PMID: 3565813.
- Malviya S, Swartz J, Lerman J. Are all preterm infants younger than 60 weeks postconceptual age at risk for postanesthetic apnea? Anesthesiology. 1993;78:1076–1081. PMID: 8512100.
- Murphy JJ, Swanson T, Ansermino M, Milner R. The frequency of apneas in premature infants after inguinal hernia repair: Do they need overnight monitoring in the Intensive Care Unit? J Pediatr Surg. 2008;43:865–868. PMID: 18485955.
- Taenzer A, Havidich J. The postanesthesia care unit and beyond. In: Cote CJ, Lerman J, Anderson B, eds. A practice of anesthesia for infants and children. Philadelphia, PA: Elsevier; 2019:1101–1102. https://www.sciencedirect.com/science/article/abs/pii/B9780323429740000471. Accessed March 30, 2025.
- Ghazal EA, Vadi MG, Mason LJ, et al. Preoperative evaluation, premedication, and induction of anesthesia. In: Cote CJ, Lerman J. and Anderson B. eds. A practice of anesthesia for infants and children. Philadelphia, PA: Elsevier; 2019:64–66. PMID: 22488124.
