DEFINITION AND RATES
A medication error is “a failure in the treatment process that leads to, or has the potential to lead to, harm to the patient.”1 In general, perioperative medication errors are under-reported. Rates of medication errors are difficult to accurately quantify as few studies have observed anesthesia professionals going through the process of medication ordering and administration. In one large, institutional study of adult patients, the self-reported incidence of medication errors was 0.004% (10/280,488) whereas the direct observation incidence was 5.3% (193/3671), suggesting that only severe medication errors with sequelae may be reported.2 In pediatric anesthesia, the estimated incidence of medication errors using self-reports is between 0.01% (276/2,316,635) to 1.92% (37/1,925).3-4,7 Pediatric patients have large variations in body weight resulting in high variability in dosing calculations. This makes children both at higher risk of medication errors as well as higher risk for harm from these errors compared to adult patients.6
COMMON CAUSES THAT LEAD TO MEDICATION ERROR
Anesthesia professionals work under high intensity conditions where multiple doses and classes of drugs are given during fast-paced clinical scenarios. This environment predisposes anesthesia professionals to medication errors. Moreover, anesthesia professionals routinely take ownership of the entire drug administration process, including prescribing, preparation, and administration. Hazards exist throughout this process (Figure 1).
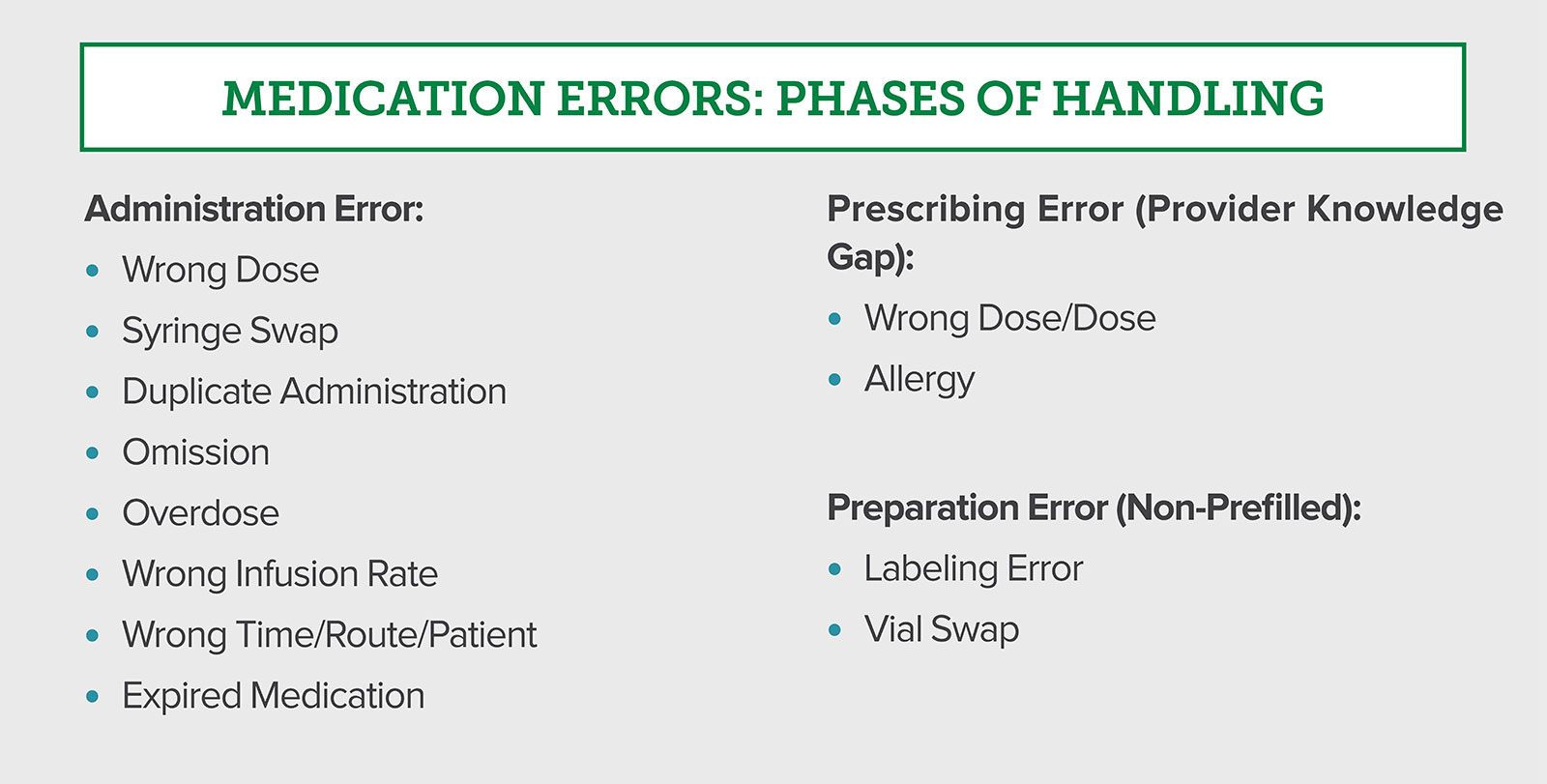
Figure 1: Primary pediatric medication errors in the perioperative setting during different phases of handling: preparation, prescribing, or administration. Adapted and modified with permission from Lobaugh LMY et al. Anesth Analg. 2017; 125:936–942.7
Wake Up Safe, a national pediatric anesthesiology quality collaborative, found that sedatives and hypnotics/opioids are the most common medications resulting in an error.
It also found that the highest incidence of medication errors was during administration (N = 179), followed by prescribing (incorrect knowledge of dose, N = 67), then preparation (N = 30) (Figure 2), next page. The most common error type during administration was the wrong dose (N = 84), followed by syringe swap (accidental administration of the wrong syringe, N = 49). Fifty-seven incidents (21%) of reported medication errors involved medication infusions as opposed to bolus administrations. Of note, nearly all (97%) of the medication errors were deemed to be preventable.7
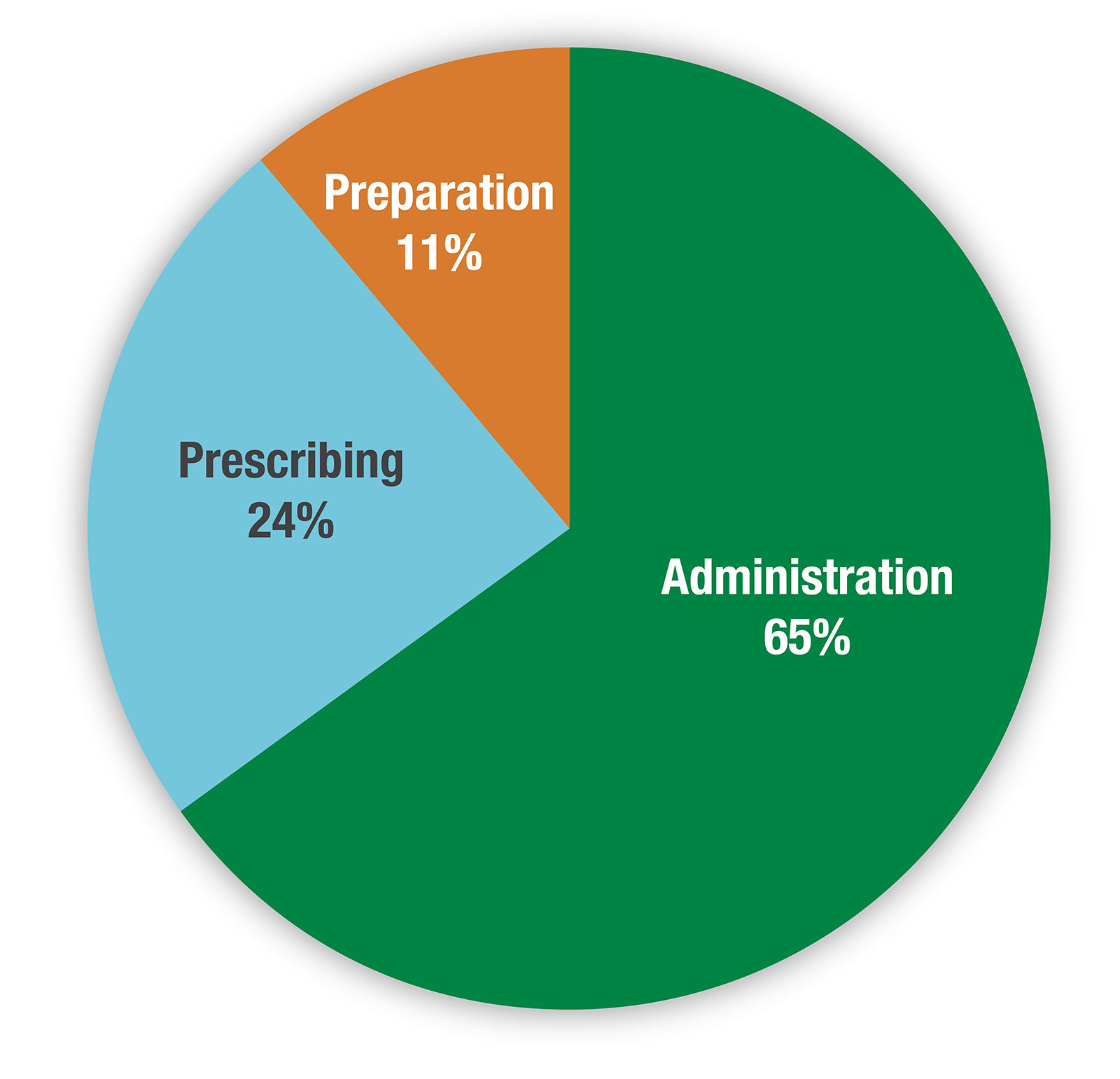
Figure 2: Phase of handling and incidence of perioperative medication errors in pediatric patients: administration, prescribing, and preparation.
Adapted and modified with permission from Lobaugh LMY et al. Anesth Analg. 2017; 125:936–942.7
HOW DO WE CONTROL THE RISK DURING MEDICATION ADMINISTRATION?
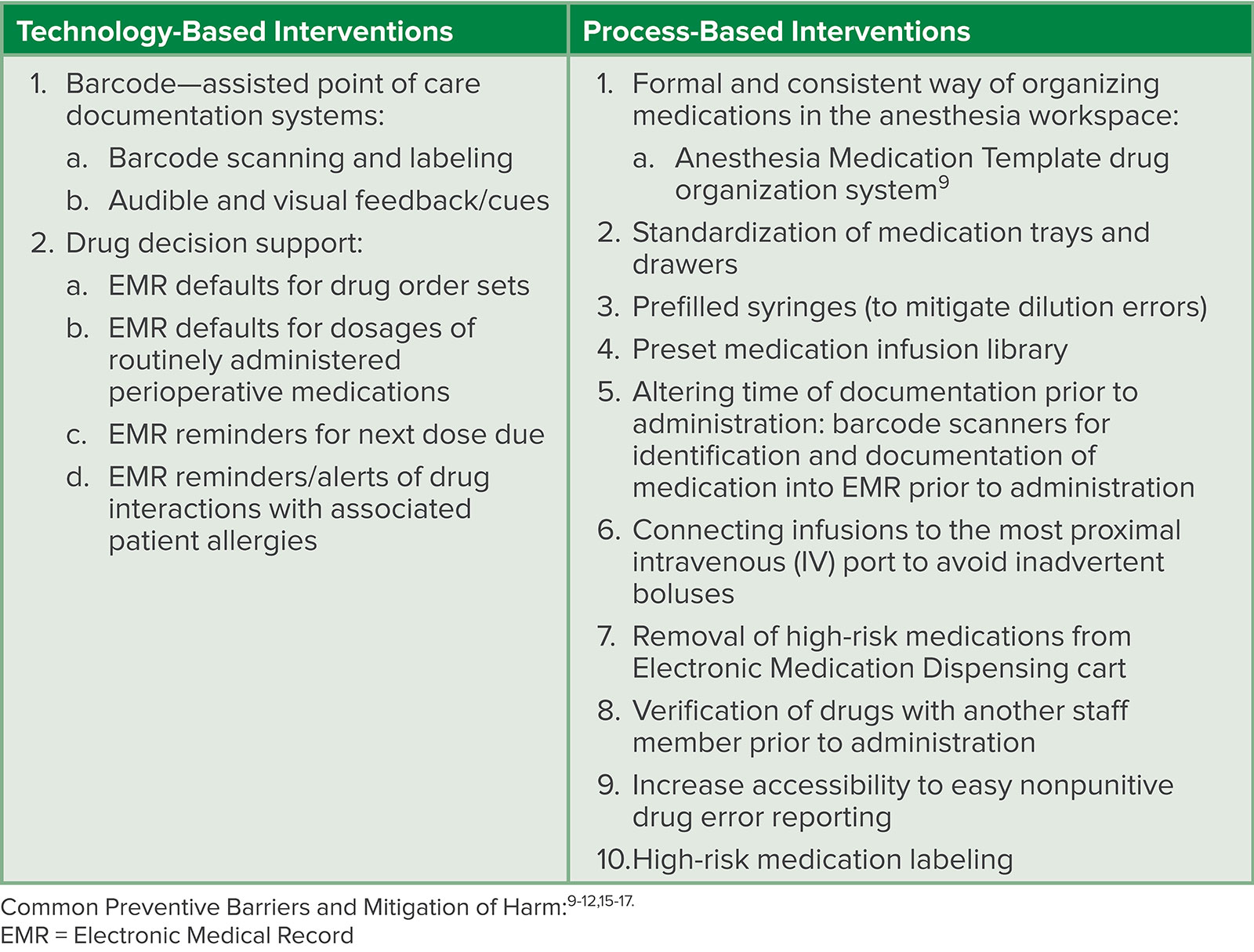
The critical step in medication administration occurs once the syringe is pushed or infusion started.8 Once the drug reaches the patient, there is potential for an immediate and irreversible change to their condition. This administration process comes with inherent possibility for error and harm. Some technological and process-based interventions can help mitigate or even eliminate harm potentially caused by the error (Table 1).
Table 1: Technological and Process-Based Interventions Reduce Medication Errors.
A FOCUS ON PEDIATRIC MEDICATION ERRORS:
For the pediatric population, specific evidence-based mitigation techniques should be considered (Figure 3).
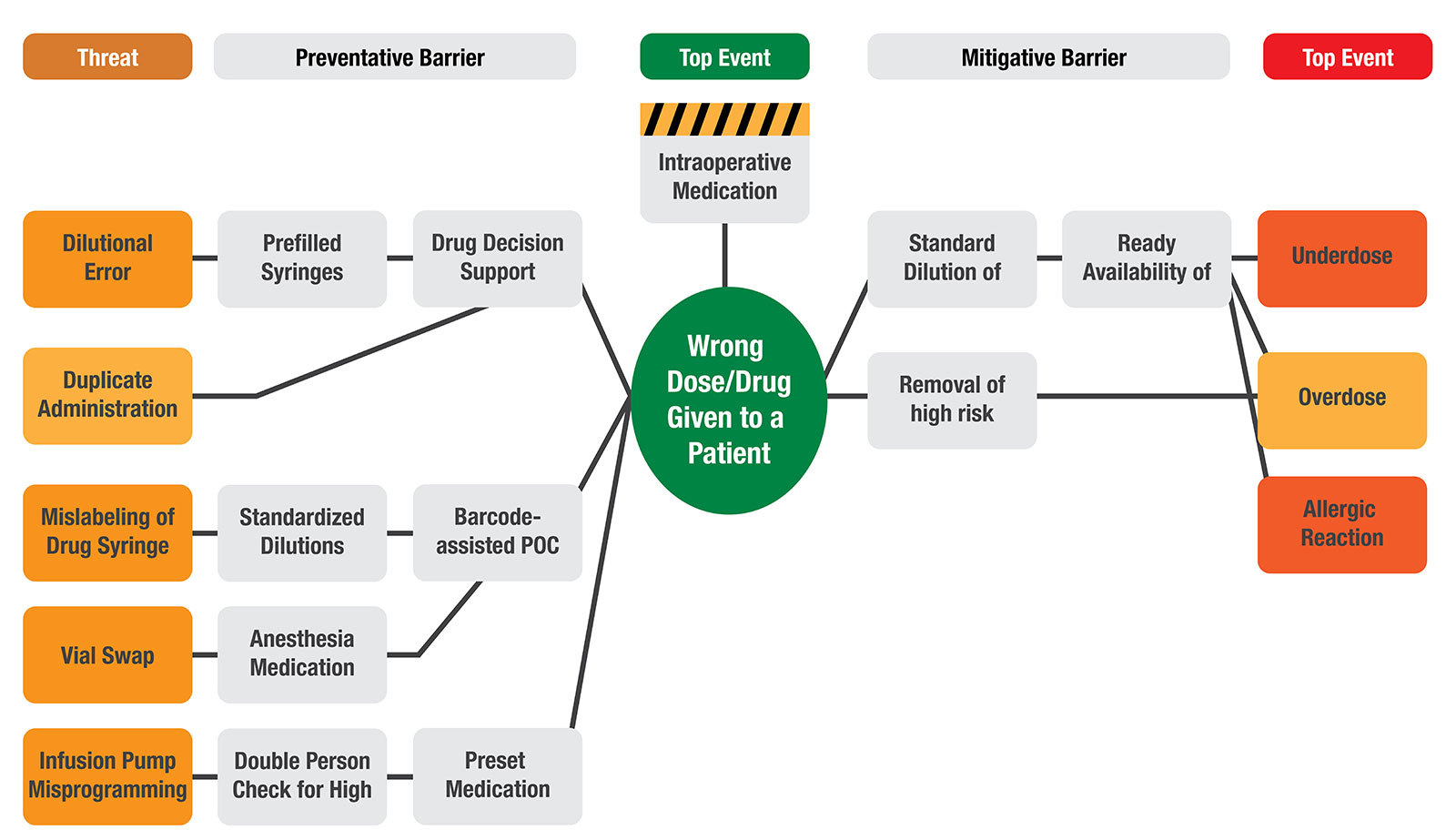
Figure 3: Bow-tie Analysis of Intraoperative Medication Errors.
POC = Point-Of-Care
The Anesthesia Medication Template (AMT) drug organization system is a formal and standardized method of organizing medications in the anesthesia workplace. This tool lessens cognitive burden and has been shown to facilitate the selection of correct syringes from the anesthesia workspace as well as correct drug dose administration.9 During simulation at a freestanding pediatric academic hospital, use of an AMT reduced incidence of overall drug dosing errors from 10.4 to 2.4 per 100 medication administrations. During phase 2 implementation, use of the AMT decreased the mean monthly error rate that reached pediatric patients from 1.24 to 0.65 errors per 1000 anesthetics. Of the errors that reached the patient, the AMT helped reduce the rate of medication swaps, miscalculation, and timing errors from 0.80 to 0.26 per 1000 anesthetics.9
Another mitigating technique is using prefilled syringes. Multiple patient safety groups including the APSF and Wake Up Safe advocate for prefilled syringes, which can provide standardized and enhanced labeling, along with ready-to-use medication doses.10-12 This practice can mitigate ampule/vial swap errors and may also decrease the risk of syringe swap.11 In a 2016 qualitative research study, System Vulnerabilities (SVs) compared provider-filled and prefilled syringe systems. SV is defined as an “activity or event that has the potential to reduce safety, efficiency of provider workflow, or increase drug costs and waste.”12 More SVs were identified in the provider-filled system compared to the prefilled syringe system, including errors due to illegible handwriting and errors due to similar medication packaging.12 Despite its safety profile, reports of medication errors related to look-alike prefilled syringes have been published involving select manufacturers. These reports emphasize the importance of selecting prefilled pharmaceuticals that meet standards set by the American Society for Testing and Materials as well as being visually distinguishable once assembled for use.13-14
A third modality is the use of point-of-care barcode scanning systems.15-17 An observational study investigating the efficacy of barcode medication-verification technology implementation in an inpatient adult populationsuggested a 41% reduction in dose, route, documentation, and administration errors and a 51% reduction in potential adverse drug events.15 In a 2022 study out of a quaternary academic children’s hospital, implementation of an electronic labeling system demonstrated a 3.6% reduction in the average daily medication discrepancy rate. Pre-implementation, the average daily medication discrepancy rate was 9.7%, decreasing to a statistically significant 6.1% (X21 = 43.9; P < .0001) post-implementation.16 Limitations to these technologies include user feasibility, compliance, cost, and availability.15-17 Technology, while it can be incredibly useful, needs to be used in the manner for which it was intended to function in a way to mitigate medication errors. When functioning outside of intended purposes, technology can pose a risk. For example, barcode scanning only works well provided that the systems link with the EMR and that the barcode provided registers appropriately. In addition, utilization of point of care barcoding technology requires partnership with pharmacy for system updates, label changes, and medication shortage management.
CONCLUSION
Direct observation via published studies of adult and pediatric anesthesia providers in the operating room estimates a medication error rate of up to 5%.2 The harm caused by medication errors is reported to be as high as three times more in pediatric patients than adults. The adverse event drug rate is highest among neonates. Potential medication error mitigation strategies include utilizing prefilled syringes, EMR decision support, medication organization aides, and barcode scanning systems.
Ying Eva Lu-Boettcher, MD, is an assistant professor in the Department of Anesthesiology at the University of Wisconsin School of Medicine and Public Health, Madison, WI.
Rahul Koka, MD, is an assistant professor of anesthesiology and critical care medicine at the Johns Hopkins University School of Medicine, Baltimore, MD.
The authors have no conflict of interest.
REFERENCES
- Aronson JK. Medication errors: definitions and classification. Br J Clin Pharmacol. 2009;67:599–604. PMID: 19594526.
- Nanji KC, Patel A, Shaikh S, et al. Evaluation of perioperative medication errors and adverse drug events. Anesthesiology. 2016;124:25–34. PMID: 26501385
- Gariel C, Cogniat B, Desgranges FP, et al. Incidence, characteristics, and predictive factors for medication errors in paediatric anaesthesia: a prospective incident monitoring study. Br J Anaesth. 2018;120:563–570. PMID: 29452813
- Feinstein MM, Pannunzio AE, Castro P. Frequency of medication error in pediatric anesthesia: a systematic review and meta-analytic estimate. Paediatr Anaesth. 2018;28:1071–1077. PMID: 30375106
- Leahy IC, Lavoie M, Zurakowski D, et al. Medication errors in a pediatric anesthesia setting: Incidence, etiologies, and error reduction strategies. J Clin Anesth. 2018;49:107–111. PMID: 29913393
- Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285:2114–2120. PMID: 11311101
- Lobaugh LMY, Martin LD, Schleelein LE, et al. Medication errors in pediatric anesthesia: a report from the Wake Up Safe Quality Improvement Initiative. Anesth Analg. 2017; 125:936–942. PMID: 28742772. PMID: 28742772
- Muschara T, Farris R, Marinus J. Critical steps: managing what must go right in high-risk operations. 1st edition, CRC Press, 2021.
- Grigg EB, Martin LD, Ross FJ, et al. Assessing the impact of the anesthesia medication template on medication errors during anesthesia: a prospective study. Anesth Analg. 2017;24:1617–1625. PMID: 28079581
- Wahr JA, Abernathy JH 3rd, Lazarra EH, et al. Medication safety in the operating room: literature and expert-based recommendations. Br J Anaesth. 2017;118:32–43. PMID: 28039240
- Eichhorn JH. APSF hosts medication safety conference: consensus group defines challenges and opportunities for improved practice. APSF Newsletter. 2010;25:1–8. https://www.apsf.org/article/apsf-hosts-medication-safety-conference/ Accessed August 13, 2024.
- Yang Y, Rivera AJ, Fortier CR, Abernathy JH 3rd. A human factors engineering study of the medication delivery process during an anesthetic: self-filled syringes versus prefilled syringes. Anesthesiology. 2016;124:795–803. PMID: 26845139
- Parr G, Desvarieux T, Fisher D. Medication error related to look-alike prefilled syringes. APSF Newsletter. 2019; 34:2. https://www.apsf.org/article/medication-error-related-to-look-alike-prefilled-syringes/ Accessed August 13, 2024.
- Hand W, Cancellaro V. “No read” error related to prefilled syringes. APSF Newsletter. 2018;33:1. https://www.apsf.org/article/no-read-errors-related-to-prefilled-syringes/ Accessed August 13, 2024.
- Poon EG, Keohane CA, Yoon CS, et al. Effect of bar-code technology on the safety of medication administration. N Engl J Med. 2010;362:1698–1707. PMID: 20445181
- Thomas JJ, Bashqoy F, Brinton JT, et al. Integration of the Codonics Safe Label System® and the Omnicell XT® Anesthesia Workstation into pediatric anesthesia practice: utilizing technology to increase medication labeling compliance and decrease medication discrepancies while maintaining user acceptability. Hosp Pharm. 2022;57 PMID: 35521011
- Jelacic S, Bowdle A, Nair BG, et al. A system for anesthesia drug administration using barcode technology: the Codonics Safe Label System and Smart Anesthesia Manager. Anesth Analg. 2015;121:410–421. PMID: 24859078
