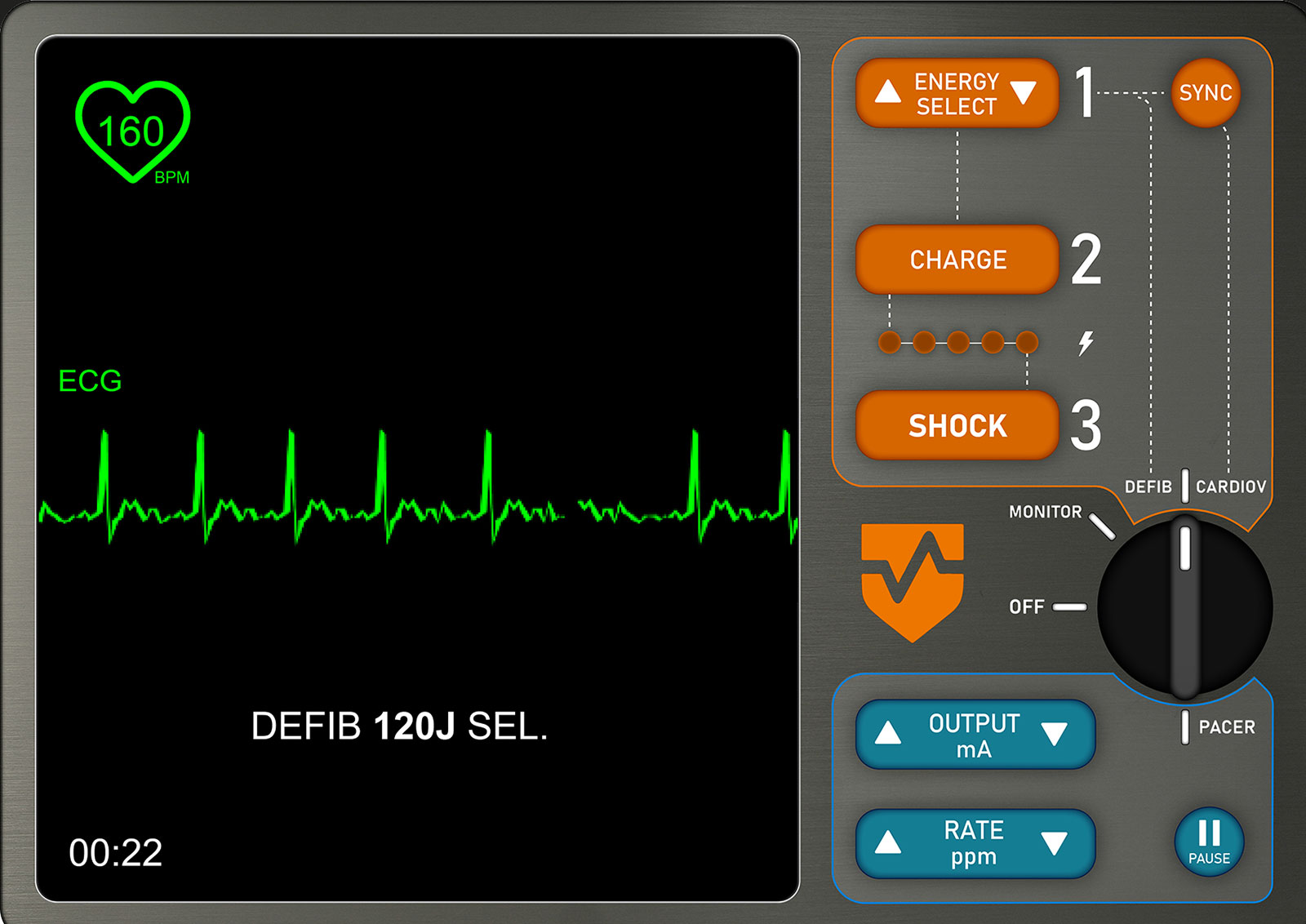
Figure 1: Interactive MED Simulation created for TEI 3.
You are taking care of a 64-year-old male undergoing an above-the-knee amputation under general anesthesia. Despite a stable intraoperative course, his heart rhythm suddenly changes to atrial fibrillation with a rapid ventricular response in the 170s. With the change in rhythm, his systolic blood pressure is in the 60s and oxygen saturation is decreasing. You call for help, notify the team, and the operating room nurse brings in the crash cart with the manual external defibrillator. You know that a cardioversion is indicated, and time is of the essence to prevent further decompensation. Do you know where to place the pads? Which setting do you select for mode and at what energy? How will you know you are synchronized for the cardioversion to prevent an R-on-T phenomenon?
Perioperative cardiac arrests are rare and anesthesia professionals play a critical role in timely diagnosis and providing life-saving treatment.1 An essential skill is the ability to promptly apply and manage the manual external defibrillator (MED). A MED is the device that in-hospital ACLS providers use to perform an indicated defibrillation, synchronized cardioversion, and/or transcutaneous pacing.2 Since the MED is rarely used, and there is considerable duress in the setting of a life-threatening cardiac event, human error, such as device mismanagement and delay to delivery of therapy, can lead to a failure to rescue.3-4
Many hospital systems have transitioned to online, E-Learning programs for Advanced Cardiovascular Life Support (ACLS) certification provided by the American Heart Association (AHA).5 ACLS providers must complete short, refresher sessions every three months instead of every two years.5 These online courses do not commonly include education on the use of a defibrillator so many providers no longer maintain or refresh their knowledge of this device. We need easily accessible learning opportunities to teach new providers how to use this device and to allow staff to maintain their knowledge so they are able to quickly and competently use the MED in a crisis.
To meet this educational need, the Anesthesia Patient Safety Foundation (APSF), in collaboration with the American Society of Anesthesiologists (ASA), is announcing the development of a third Technology Education Initiative (TEI) course entitled “Manual External Defibrillation, Cardioversion, and Pacing (MEDCP)”. Previous courses have been Low-Flow Anesthesia6 and Quantitative Neuromuscular Monitoring.7 These courses use guided interactive simulation to provide an active learning experience for the user to understand complex, technology-based concepts.
The MEDCP course will consist of seven different topics that cover the essentials of understanding and using a MED, each targeted to require about 15 minutes to complete. Like previous TEI courses, guided simulation is used to provide an interactive learning experience. While the topics are recommended to be done in sequence, they do not need to all be completed at the same time for a more convenient learning experience. Highlights of the course include:
Physics of Defibrillators: A brief explanation of the physics behind the device that will allow you to better understand the MED.
Defibrillator Waveforms: Visualize and practice delivering the different types of electricity waveforms emitted from commonly used defibrillators.
Defibrillator Pad (Electrode) Placement: Practice placing defibrillator pads on a simulated patient in the different anatomical locations, including anterior-posterior and anterior-lateral.
Defibrillation, Synchronized Cardioversion, and Transcutaneous Pacing: Use a simulated, generic MED (Figure 1) to practice performing the three main functions of the MED.
The course is projected to be completed in January 2025 and will be available online at the ASA website through the APSF web portal at https://www.apsf.org/TEI/. All the TEI courses are free and readily accessible. Any anesthesia professional or interested party can take any TEI course by creating a free guest account if not already an ASA member. Continuing medical education credits will be available for those that participate including patient safety and quality improvement.
We look forward to completing the course and hope it will be useful in better preparing you to manage a perioperative ACLS event.
Michael Kazior, MD is an assistant professor of anesthesiology at Virginia Commonwealth University Health and the Richmond Veterans Affairs Medical Center, Richmond, VA.
Christopher Samouce, PhD, is an assistant scientist at CSSALT at the University of Florida College of Medicine, Gainesville, FL.
Daniel Rosenkrans, MD, is an assistant professor of anesthesiology at the University of North Carolina at Chapel Hill, Chapel Hill, NC.
David Lizdas, BSME, is the lead engineer at CSSALT at the University of Florida College of Medicine, Gainesville, FL.
Jeffrey Feldman, MD, MSE, is an adjunct professor of clinical anesthesiology at the Perelman School of Medicine, Philadelphia, PA. He is also the chair of the APSF Committee on Technology.
Nikolaus Gravenstein, MD, is the Jerome H. Modell, MD, Professor of Anesthesiology at the University of Florida College of Medicine, Gainesville, FL.
Samsun Lampotang, PhD, FSSH, FAIMBE, is the Joachim S. Gravenstein Professor of Anesthesiology and the Director of CSSALT at the University of Florida College of Medicine, Gainesville, FL.
Dr. Feldman is a consultant for Medtronic, Becton-Dickinson, and Micropore. Dr. Gravenstein is a consultant for Teleflex Medical.
The other authors do not have any conflicts of interest.
REFERENCES
- Nunnally ME, O’Connor MF, Kordylewski H, et al. The incidence and risk factors for perioperative cardiac arrest observed in the national anesthesia clinical outcomes registry. Anesth Analg. 2015;120:364–370. PMID: 25390278
- Panchal AR, Bartos JA, Cabanas JG, et al. Part 3: Adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142:S366–S468. PMID: 33081529
- Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equipment failures in anesthesia management: considerations for prevention and detection. Anesthesiology. 1984;60:3–42. PMID: 6691595
- Olympio, MA. Formal training and assessment before using advanced medical devices in the operating room. APSF Newsletter. 2007;22:63–68. https://www.apsf.org/article/formal-training-and-assessment-before-using-advanced-medical-devices-in-the-operating-room/. Accessed June 28, 2024.
- American Heart Association. RQI: Resuscitation Quality Program overview. https://cpr.heart.org/-/media/CPR-Files/Courses-and-Kits/RQI/RQI-Program-Overview.pdf. Accessed July 28, 2024.
- Anesthesia Patient Safety Foundation. Low-flow anesthesia. https://www.apsf.org/apsf-technology-education-initiative/low-flow-anesthesia/. Accessed July 28, 2024.
- Anesthesia Patient Safety Foundation. Quantitative neuromuscular monitoring. https://www.apsf.org/apsf-technology-education-initiative/quantitative-neuromuscular-monitoring/. Accessed July 28, 2024.
