INTRODUCTION
The International Organization for Standardization (ISO) was established in 1947 as a nongovernmental organization (NGO) in the United Nations with the aim of revitalizing the global economy post-World War II. ISO has primarily focused on standardizing industrial products and manufacturing processes to facilitate international trade. Participation and voting rights are on a country-by-country basis, but implementation is worldwide and the way each country aggregates opinions varies.
The ISO standards are formulated primarily by manufacturers, but diverse input from health care professionals is essential in sectors like medical devices. Manufacturers often lead the development of standards due to their expertise in manufacturing processes and regulatory compliance. However, without sufficient input from clinical experts, there is a risk of standards not fully addressing the clinical needs and safety concerns of medical professionals.
Unlike general industrial equipment, many clinical medical devices place greater emphasis on how they are used rather than their technical specifications. It is important to recognize that the ultimate responsibility for the use of medical devices rests with the clinician, who must take full responsibility for the lives of their patients.
Despite efforts to integrate the opinions of medical experts through Technical Committees, clinician involvement remains limited in some areas, with manufacturers often driving discussions.
ISO 80369
Growing international awareness of medical safety spurred the ISO to address medical accidents caused by misconnections and misadministration by developing unique connector design standards for enteral, respiratory, urinary, blood pressure, neuraxial, and intravenous patient care systems.1,2 ISO started releasing the ISO 80369 series of standards in 2016.2 Participating countries have been encouraged to adopt these international standards without delay (Table 1, Figure 1).
Table 1: ISO 80369:
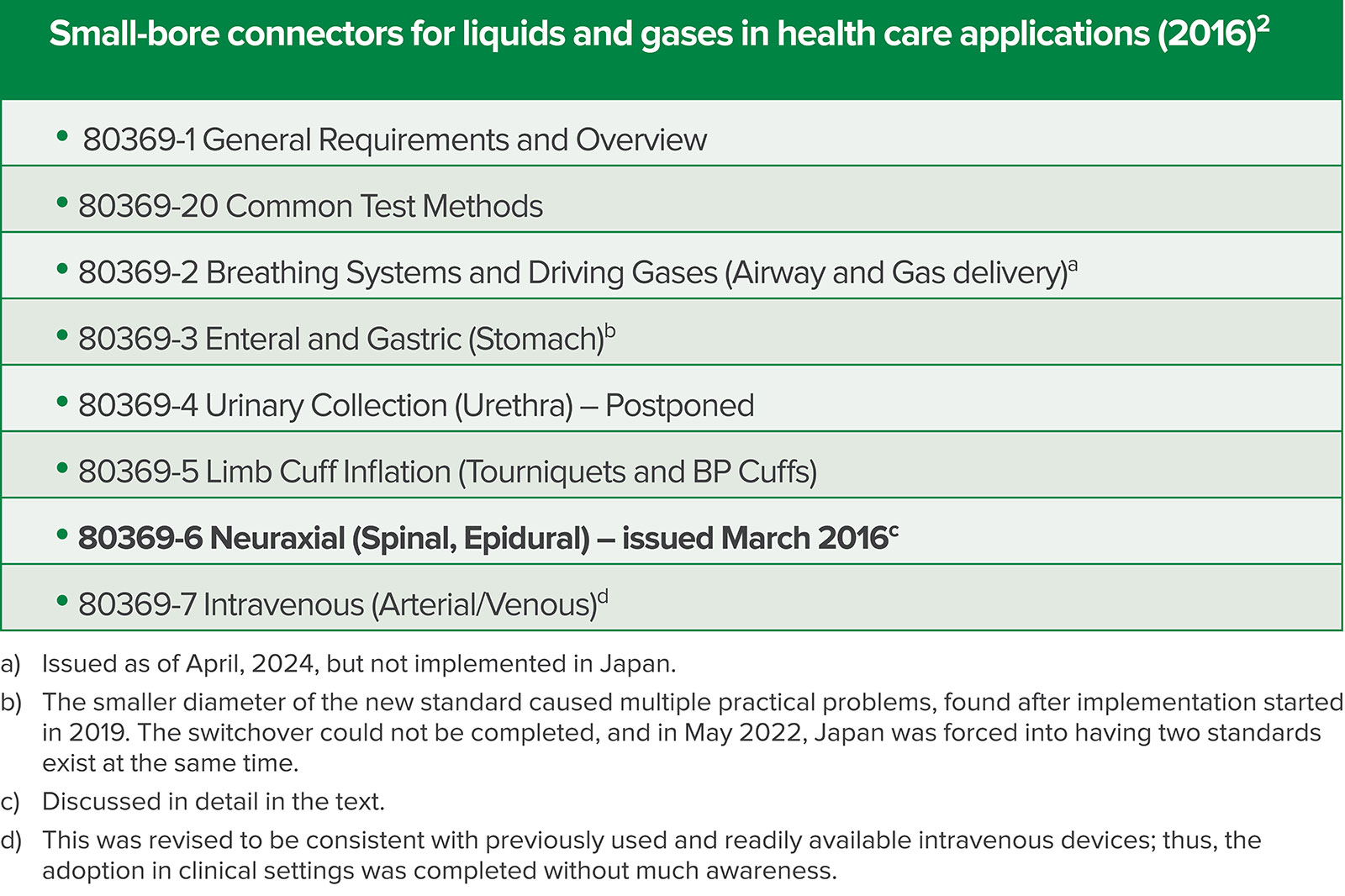
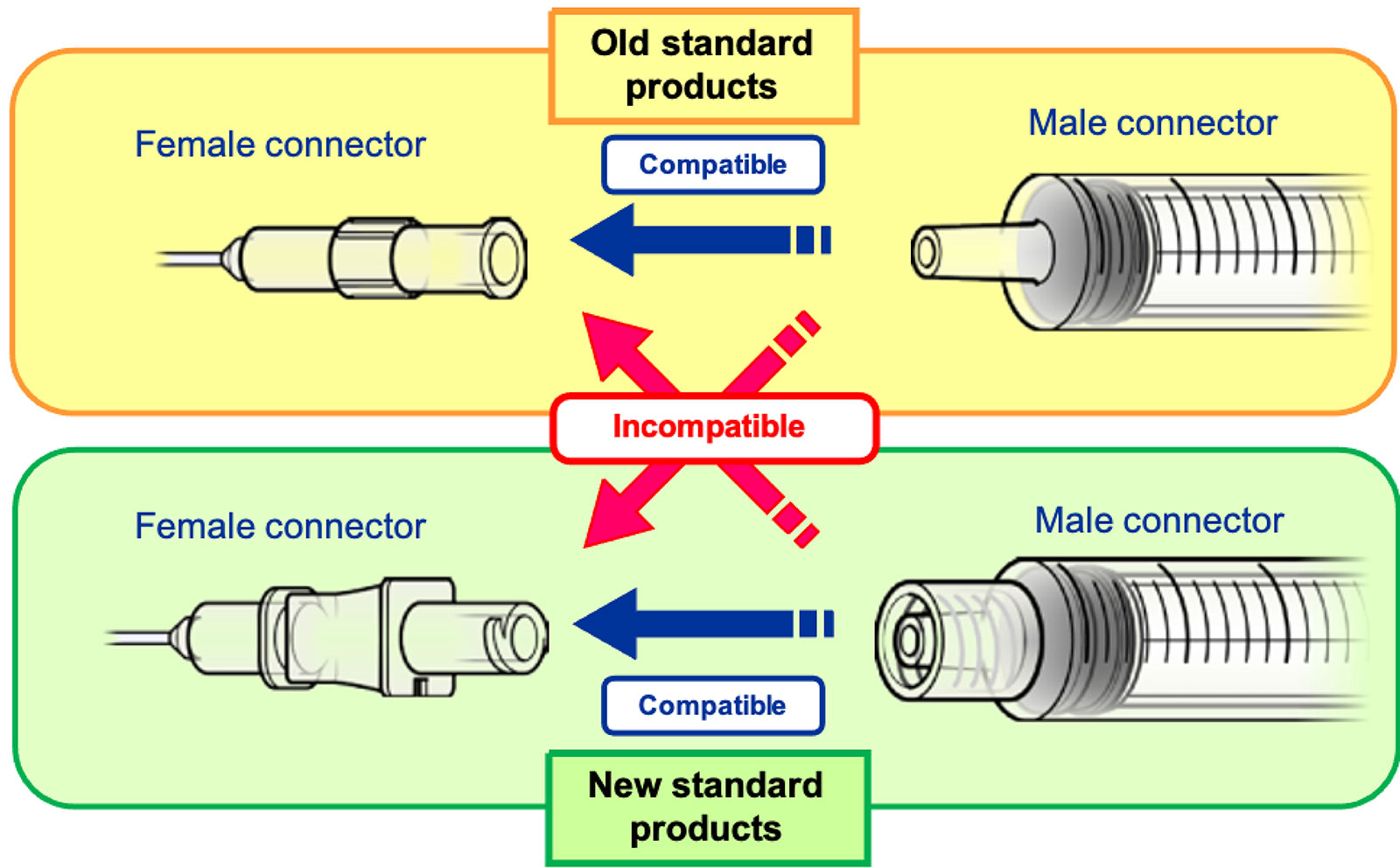
Figure 1: Old standard (Luer) connector and New standard (ISO 80369-6) connector.
PMDA Medical Safety Information, No.55 August 2018, Connections of new and old standard products http://www.pmda.go.jp/english/safety/info-services/safety-information/0001.html
Japan implemented a nationwide introduction of ISO 80369-6 (neuraxial applications) under governmental leadership upon receiving information (source unknown) that the introduction of ISO 80369-6 had begun globally, including parts of the United States. The transition is now almost complete, and while no major accidents involving loss of life have been reported during the transition process, numerous serious issues were experienced. As far as we know, no other country has yet fully switched over to this new standard, so Japan’s experience can contribute to patient safety worldwide by raising awareness of the associated problems that can occur.
NEED FOR NEW STANDARD FOR NEURAXIAL APPLICATIONS (ISO 80369-6)
 For many years in clinical practice, the Luer connection (ISO-594) was standard for injections and connecting small-diameter tubing. Health care providers benefited from the convenience provided by its universal connectivity. However, preventing accidental injections due to misconnecting Luer connections depends solely on the vigilance and responsibility of the medical personnel involved.
For many years in clinical practice, the Luer connection (ISO-594) was standard for injections and connecting small-diameter tubing. Health care providers benefited from the convenience provided by its universal connectivity. However, preventing accidental injections due to misconnecting Luer connections depends solely on the vigilance and responsibility of the medical personnel involved.
Human error, an unavoidable cause of patient injury, has therefore led to misconnecting many types of medical devices.1 Discussions on the ISO 80369 series began around 2005 with the goal of developing purpose-specific connections utilizing physical noninterfacing mechanisms specific to each application to ensure that misconnections are simply not possible.
Discussions on a purpose-specific compatibility standard for preventing misconnections (ISO 80369 series) were undertaken by ISO in Technical Committee 210 (TC 210, quality management), liaising with TC 121 via Joint Working Group 4. TC 210 covers a broader range of topics and is not necessarily an anesthesia-focused TC, especially compared to TC 121 where many prominent anesthesia professionals participate. A joint working group was formed under TC 210 to convey the voices of TC 121 on this matter, but, unfortunately it was ineffective.
Anesthesia professionals have actively participated since the early stages, making significant contributions to the field of anesthesia and intensive care. TC 121 has SC-3 (Subcommittee) that deals with products directly handled by anesthesia professionals, such as ventilators, oxygen concentrators, and related patient monitors.
THE DECISION-MAKING PROCESS FOR THE IMPLEMENTATION OF ISO 80369-6 IN JAPAN
In Japan, the implementation system essentially remains the same as it was when ISO was first established. The main supervisory body for medical devices that affect human lives is the Ministry of Health, Labour, and Welfare (MHLW), which also holds licensing authority. However, the Ministry of Economy, Trade and Industry (METI), which oversees general industries, liaises with ISO. In practice, information flows from METI to MHLW. As a result, there is a lack of supervision and a lack of proactive participation by clinicians on a domestic and international level.
When the implementation of ISO 80369 was first discussed at the Safety Division of MHLW in 2015 with some health care representatives, the switchover to ISO 80369-6 was already assumed. Concerns were raised at the time by anesthesia professionals regarding potential confusion from the switchover, but in practice, there were no meetings that included clinical physicians or the Japanese Society of Anesthesiologists (JSA). The procedures and deadlines for the introduction were determined between MHLW and an industrial organization, MTJAPAN. The Ministry explained that Japan, as a member of the World Trade Organization, has a fundamental obligation to comply or harmonize with ISO standards.3 Although exceptions do exist, Japan is required to adopt the ISO standard as the national standard without delay after a new standard is issued, and changes that would create international trade barriers are not permitted.
While it is essential to carefully consider the risk-benefit balance in clinical settings before implementing ISO standards, there are no organizations or opportunities to deliberate on these considerations in Japan.
The MHLW issued a notification in December 29, 2017, stating that the sale of old products affected by ISO 80369-6 must cease by the end of February 2020. The deadline for product supply was set at the convenience of the company, so anesthesia professionals had no choice but to comply.
At the strong request of anesthesia professionals onsite, an interchangeable adapter was not introduced for safety reasons. Awareness activities were conducted by the industry association for manufacturers and suppliers (MTJAPAN), targeting relevant academic societies. The Pharmaceuticals and Medical Devices Agency (PMDA) provided specific details on the implementation procedures. Despite these measures, awareness of the need for and possibility of switching was not well known to anesthesia professionals.
MHLW SURVEY ON THE SWITCHOVER TO ISO 80369-6 IN JAPAN
The transition was carried out and the switchover was completed in approximately two years. In June 2024, MHLW released a report on the transition to ISO 80369-6, which began in 2021.4 The report includes the results of a postal survey of limited scope, of anesthesia professionals and MTJAPAN. The survey was mainly targeted at facilities accredited by the Japan Society of Anesthesiologists (JSA), with 1447 facilities contacted, and 329 valid responses.
The MHLW survey was not intended to ascertain patient-related contingencies, but rather to investigate product-related issues; thus, there was a possibility for under-reporting untoward events handled by anesthesia professionals.
MHLW SURVEY RESULTS AND ISSUES
The main survey results are summarized in Table 2. We were shocked by the number of initial troubles experienced.
Table 2: Issues Encountered With the Change to ISO 80369-6.
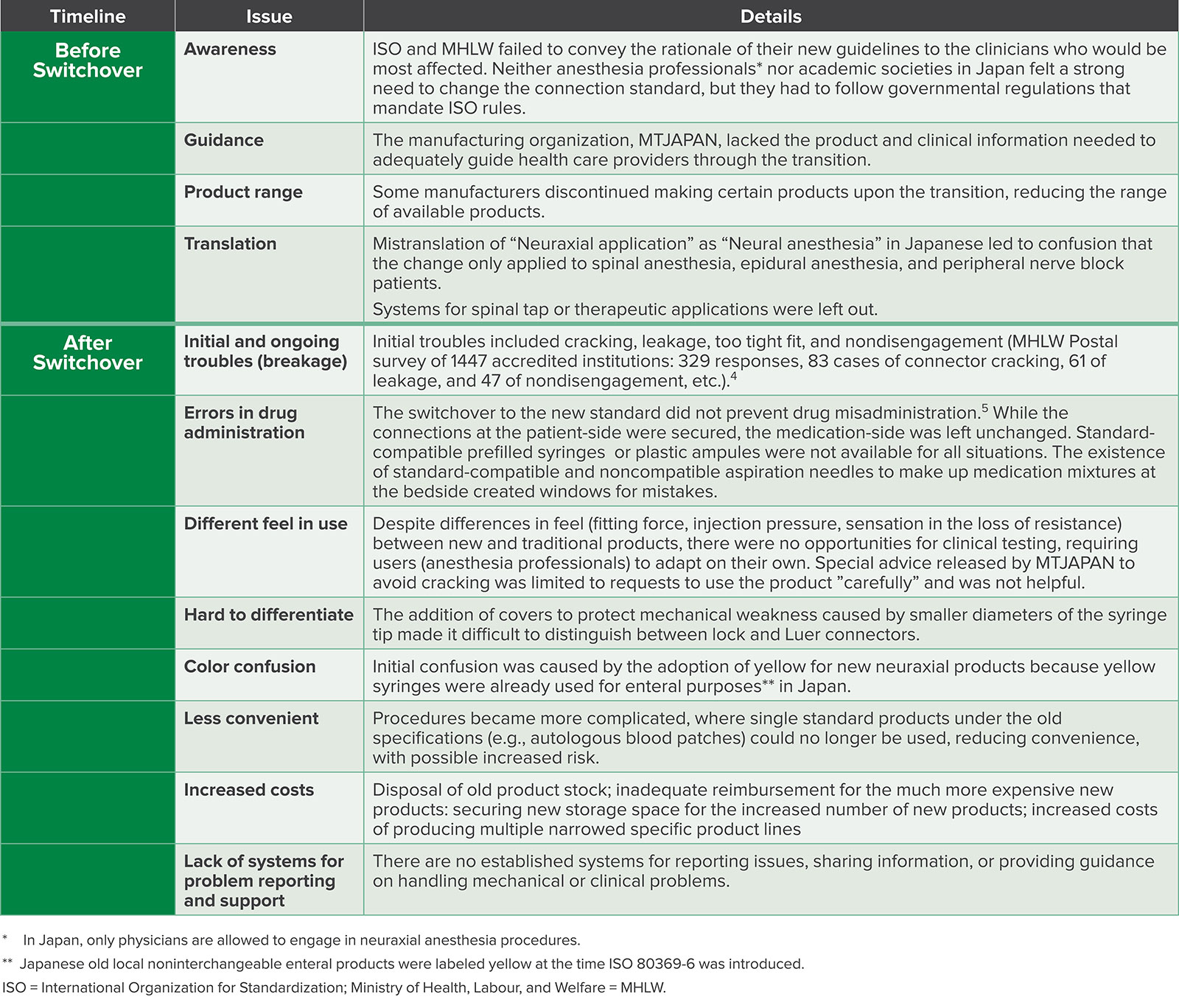
Inadequate advisories before the switchover put clinicians at a disadvantage, as they were not prepared for the changes. Numerous cases of breakage and leakage during patient care were reported. No patients were harmed due to quick thinking on the part of anesthesia professionals.
Drug misadministration was a constant worry as connector sets with connectors and pre-filled syringes were not fully available.5 Errors due to incorrect connection to medication were avoided only due to professional diligence.6
Incomplete switchovers, due to the nonavailability of all syringes and connectors, created confusion at the bedside, as old and new connectors were placed side by side. Other unnecessary confusion resulted from poor translation, overlap in connector colors, inadequate product availability, and wasted resources. Above all, there were no processes available to clinicians, before or after the switchover, to convey or report problems.
Several issues were raised, as follows:
1. Insufficient clinical involvement
Both the ISO 80369-6 standard formulation process and the Japanese domestic implementation process by the government and manufacturers suffered from lack of practical clinical information.
Once ISO 80369 standards were set, there was little discussion of whether to implement or accommodate the domestic clinical situation by governmental agencies in Japan.
2. Imbalanced perspectives (clinicians, manufacturers, and regulatory agencies)
Manufacturers assumed it was acceptable, indeed unavoidable, to produce fittings that, while compliant with the standard, were hard to use, especially by uninformed users. Clinicians, had they been aware of this, would have refused to use products as patient safety was at risk.
The transition to smaller diameters without clinical trials led to confusion in usage related to changes in liquid flow and increased push-in and rotational forces. Problems included difficulty of use and snap breakage of connectors. This forced clinicians to deal with issues like extra-strong fittings and liquid leaks from cracked connectors while working in the field.
3. Lack of clinical feasibility trials
It was absolutely necessary to do clinical feasibility studies across products (between products of various companies) before domestic implementation to avoid patient harm and physician’s liability. However, clinical feasibility trials before full-scale introduction were actively denied based on a false and biased perception among regulatory agencies and manufacturers saying this would violate competition laws. Most of the problems Japan experienced during implementation could have been avoided with proper information and preparation. It is regrettable that clinicians were effectively eliminated from this discussion, with their only option being to accept the administrative decision.
4. Lack of transparency
Regulatory agencies were under the mistaken belief that clinical feasibility trials were unnecessary as the newly introduced products already complied to the new authoritative ISO standard. Manufacturers did not see the need to inform clinicians of “small” changes in how the new products fit together. Clinicians were not aware of this situation in Japan and had no place to address these concerns.
The consensus-building process in ISO is not available to those outside the group, but compliance with the standards produced is mandatory and strongly promoted by local administrative agencies in Japan. At present, users (clinicians), who are required to follow the standards, are only able to learn about them after purchasing ISO’s official publications.
This process needs to be improved as it not only impedes the timely dissemination of information, but also is too technical for ordinary health care workers to understand. Unaware that the new standards resulted in products that differed significantly from before, clinicians experienced such dire clinical consequences as liquid leaks and cracked connections due to extra-strong fittings. They had to deal with such problems while patients were undergoing procedures.
ROLE OF CLINICIANS IN DOMESTIC IMPLEMENTATION OF ISO STANDARDS
Domestically, challenges arise in ensuring standards meet local health care requirements, usability, and patient safety. These include consideration of product availability, changes in functionality from preexisting standards, education level, and scope of professional responsibility.
Feasibility studies by clinicians before introduction are crucial to protect patients and validate the efficacy of the standards in specific national contexts, but were denied under the pretext of competition law. Effective integration of ISO standards requires balancing manufacturer efficiency with comprehensive clinician involvement and responsive domestic adoption processes. From a clinician’s perspective, the lack of clinical usability tests before the implementation was truly regrettable.
A similar issue is happening with ISO 80369-3 (enteral applications). Pediatricians experienced practical problems, such as the inability to administer blended diets or to aspirate stomach contents because of the much smaller diameter of the new standard. The switchover, which started in 2019 and was to be completed by 2021, was delayed. MHLW already had introduced its own noninterchangeable connection in 2000 (MHLW No. 888) that was well-received, but was forced to switch to ISO 80369-3. Japan was forced into allowing both the old and new standards in May 2022.7 Confusion persists to this day.
Incredibly, such a basic error went unnoticed during the creation of the ISO standard. Japan introduced its own noninterchangeable enteral connection standard in 2000, and it is regrettable that the already-proven Japanese standard was not adopted by ISO.
SUMMARY
ISO issued a series of ISO 80369 standards to physically restrict connections between syringes, needles, and other small-diameter components to their intended purposes only. Japanese administrative authorities started a nationwide initiative to introduce ISO 80369-6 (neuraxial applications) in 2018 as part of the implementation of the new standards. To our knowledge, this is the first country level switchover in the world.
This decision was made without adequate consultation with clinicians or professional anesthesia organizations. New products were approved in Japan if they conformed to the new ISO standards, but were introduced into clinical practice without any preliminary feasibility trials. Anesthesia professionals in the field lacked sufficient information and encountered numerous unexpected problems, such as breakage and leaks.
No disastrous accidents involving human lives were reported during the switchover, but we experienced serious incidents that cannot be ignored.
Clinicians and medical societies, such as JSA and APSF, should become more involved to raise awareness in ISO, industry, and domestic regulatory agencies of the essential importance of clinical input. One of the reasons the government and industries have an overly strong voice in Japan is related to the extreme fragmentation of medical specialties making it harder for everyone to work together.
In a clinical setting, it is very important to consider how a product is used coupled with the quality of the product itself. The most important thing is to protect patients’ lives. Anesthesia professionals must not condone situations that threaten patient safety. We should be more involved in the decision-making process of perioperative devices approved by the ISO.
Sachiko Omi, MD, PhD, is visiting professor in anesthesiology, Tokyo Jikei Medical University, Tokyo, Japan.
Akito Ohmura, MD, PhD, is professor emeritus, Teikyo University Medical School, Tokyo, Japan, and chair, ISO TC 121 SC-3.
Katsuyuki Miyasaka, MD, PhD, is professor emeritus, St. Luke’s International University, Tokyo, Japan.
The authors have no conflict of interest.
REFERENCES
- Examples of Medical Device Misconnections. https://www.fda.gov/medical-devices/medical-device-connectors/examples-medical-device-misconnections. Accessed July 30, 2024.
- ISO 80369-6:2016 Small bore connectors for liquids and gases in healthcare applications, Part 6: Connectors for neuraxial applications, published (Edition 1, 2016). https://www.iso.org/standard/50734.html. Accessed July 30, 2024.
- Article 2.4 of the TBT Agreement: Agreement on technical barriers to trade, technical regulations and dtandards, Article 2: Preparation, adoption and application of technical regulations by central government bodies, 1995. https://www.wto.org/english/docs_e/legal_e/17-tbt_e.htm. Accessed July 30, 2024
- Miyajima A. Pharmaceuticals and medical devices regulatory science policy research project: research on post-market safety measures for the safer and more effective use of new types of medical devices, etc. FY 2023 Summary and Joint Research Report (21KC2007). 2023 (In Japanese)
- Lefebvre PA, Meyer P, Lindsey A, et al. Unraveling a recurrent wrong drug-wrong route error— tranexamic acid in place of bupivacaine: a multistakeholder approach to addressing this important patient safety issue. APSF Newsletter. 2024;39:37,39–41. https://www.apsf.org/article/unraveling-a-recurrent-wrong-drug-wrong-route-error-tranexamic-acid-in-place-of-bupivacaine/. Accessed July 30, 2024.
- Institute for Safe Medication Practices (ISMP). Implement strategies to prevent persistent medication errors and hazards. ISMP Medication Safety Alert! Acute Care. 2023;28 (6):1–4. https://psnet.ahrq.gov/issue/implement-strategies-prevent-persistent-medication-errors-and-hazards Accessed July 30 2024.
- The distribution of new standard products (ISO80369-3) has been phased in starting from December 2019. https://www.pmda.go.jp/files/000246586.pdf. Accessed July 30 2024.
