
Robert K. Stoelting, MD
Any startup organization has a critical test of sustainability when it makes its first leadership transition. The APSF had the experience in 1997 when our beloved founder and leader, Dr. Jeep Pierce, passed on the reins of his Presidency to the first successor. Jeep had the proverbial big shoes to fill. Who could take on that role and not only sustain, but grow our vital yet still adolescent band of anesthesia patient safety advocates? It was our exceptional good fortune that Dr. Bob Stoelting was willing to take the challenge. Nineteen years later, Dr. Stoelting, too, has passed on the reins to a successor. We all owe so much to Bob for the continued, steady effort to not just keep anesthesia relatively safe, but to also make it even safer. He has been a remarkable leader, colleague, and passionate crusader for our common goal: that no patient shall be harmed by anesthesia.
Dr. Stoelting came to the position of President of the APSF (POTAPSF) as one of anesthesiology’s most esteemed academic leaders. This is what was written about him when he assumed the APSF Presidency in 1997:
Dr. Stoelting, most recently ASA Vice-President for Scientific Affairs until this year, is a native of Indianapolis, Indiana, who received his undergraduate and medical educations at Indiana University before anesthesiology residency at the University of California, San Francisco. After two years at the NIH, Dr. Stoelting joined the faculty (Anesthesia and Pharmacology) at Indiana University in 1970, rising rapidly to become Professor and Chairman of Anesthesia in 1977. Also extensively involved in ASA committees and administration for many years, Dr. Stoelting was a District Director before becoming Vice-President for Scientific Affairs. Possibly best known as an educator for his prodigious and prestigious authorship of important and very widely used textbooks (Basics of Anesthesia, Pharmacology and Physiology in Anesthetic Practice, and Anesthesia and Co-Existing Disease as well as co-editing Clinical Anesthesia with Drs. Barash and Cullen and editing periodicals such as the Yearbook of Anesthesiology and Advances in Anesthesia), Dr. Stoelting has been a Director and the President of the American Board of Anesthesiology. He has been Chairman of the ACGME Anesthesiology Residency Review Committee, and is a Director of the Foundation for Anesthesia Education and Research. This Spring, he will deliver the T.H. Seldon Memorial Lecture to be entitled “Anesthesiology—a medical specialty with unique challenges and opportunities” at the Annual Meeting of the International Anesthesia Research Society (for which he has also served as Chair of the Board of Trustees). Dr. Stoelting brings this truly remarkable background to his new role as the leader of the APSF, which will benefit greatly as it moves forward into the next century from the vision and wisdom. Dr. Stoelting has gained from the extraordinary breadth and depth of his career.1

Dr. Stoelting led the development of the widely downloaded “Fire Safety Video” for prevention of on-patient fires in the operating room.
APSF was incredibly fortunate that Bob Stoelting was ready and eager for even more national service, leadership, challenge, and impact. While that might have been via the ASA, he chose to dedicate the next phase of his career to patient safety via APSF. Despite his vast knowledge and experience in anesthesiology, Bob hadn’t yet focused on patient safety alone. However, through his participation and leadership in APSF, he adroitly directed his energies forward. Like everything he has done in his life, he undertook this responsibility with total dedication, passion for learning, wisdom, and effective leadership. His prior experience in clinical anesthesia, research, and academic and organizational leadership in the field prepared him better than anyone to take on this prestigious role.

Dr. Stoelting provided decisive leadership for developing numerous patient safety initiatives by convening relevant stakeholders at targeted conferences and workshops.
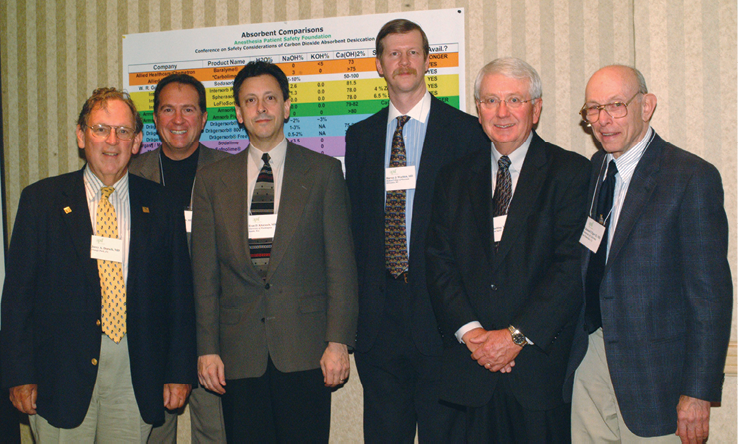
Left to right, Drs. Dorsch, Olympio, Kharasch, Woehlck, Stoelting,and Eger speak at the APSF Conference on Safety Considerations of Carbon Dioxide Absorbents on July 27, 2005, in Chicago, IL. (APSF Newsletter. 2005;20:25.)
There are so many wonderful, effective qualities about Bob Stoelting that have enabled APSF’s continued influence. Most important is his leadership style. The 19-member multidisciplinary Executive Committee is the main working instrument of APSF, and we are not a shy bunch. The discussions at meetings are always collegial and respectful, but sometimes intense. We have a lot of opinions and are not always good at self-policing. Bob was fantastic at keeping us on track, yet allowing creativity to emerge. He always guided the group to seek consensus, which we almost always could achieve. Yet, when consensus was not initially present, he diplomatically steered us to a place where we could agree on a direction or decision that led to positive changes for patient safety. APSF was fortunate that this was one of many of Bob’s leadership attributes.

Drs. Stoelting and Pierce pose at the APSF ASA booth.
For the 31 years since the founding of APSF, I’ve experienced a substantial turnover of the Executive Committee membership as members retired. What is so remarkable is how the original culture of dedication, trust, and mutual respect has endured. That is in no small measure a result of how Bob Stoelting models and enables the behaviors that are essential to the continuity of that culture, which I believe have been essential to our ongoing effectiveness. I have never experienced such an extended level of collegiality and mutual respect in any organization. It’s what has kept me going at the same level of interest and commitment all these years. Like Jeep before him, Bob has made that possible by how he helps shape the composition of the team and how he leads it, with a light, but highly leveraged touch. Bob (similar to his predecessor) perpetuated the axiom that anesthesia patient safety is a multidisciplinary, collaborative process. He has always embraced ideas from a variety of providers, business leaders, and national organizations to further the quest to improve patient safety. In all that he does, he conveys his respect for all of us (on the executive committee and beyond!), that he holds and lives with the highest ethical standards, that he listens and is entirely open to dissent, and can change his mind based on what he learns from others. Most notable is that he does all of this with humility and grace.

Dr. Stoelting initiated the annual APSF conference in Phoenix, AZ, where relevant stakeholders are invited to participate in the development of consensus statements for specific patient safety issues. The APSF has recently named this annual meeting the “Stoelting Conference” in honor of Dr. Stoelting’s tireless dedication to patient safety.
I haven’t heard Bob Stoelting espouse a specific philosophy or strategy for how patient safety in anesthesia should be maintained and continuously improved. Instead, it is my interpretation that he has guided APSF and its patient safety strategy through continuous, steady progress. Rather than big leaps forward or forced changes in behavior, patient safety is a continual series of small steps that make everyday work and processes safe. It’s not a big bang or a revolution, but rather a continuous evolution. As individual providers and their organizations change their practices to be safer, the culture changes. It’s not just the changing of practices; it’s the growing commitment and enlightened attitudes to continuously make anesthesia safer, project by project. He understands that culture change is the sum total of what we do as individuals, not a magical force or prescribed, demanded actions. He has instantiated this philosophy through the steady stream of projects and concepts that are the product of what APSF does. That product has been disseminated primarily via the APSF Newsletter, which is now distributed widely to about 122,000 people around the world, and available free of charge to anyone on our website. The message of APSF is further disseminated via the workshops and consensus conferences that Bob either has led himself or guided us on the Executive Committee to develop and lead every year.
The following observations don’t provide a complete history of the 19 years that Bob has been at the helm of APSF. However, they are examples of specific projects and programs he has championed to illustrate how this philosophy of issue-by-issue safety improvements has affected change:
APSF Consensus Conferences (now known as the annual Stoelting Conference)
Bob promoted these events, which have become one of the important mechanisms by which we identify solutions to current patient safety issues and, from those, choose which initiatives to promote vigorously. Each year, the Executive Committee, under Bob’s guidance, chose a topic and leader to run the conference. Through his skillful management of APSF talent and creativity, almost entirely from volunteers, we’ve shared the workload and had a diversity of topics and speakers.
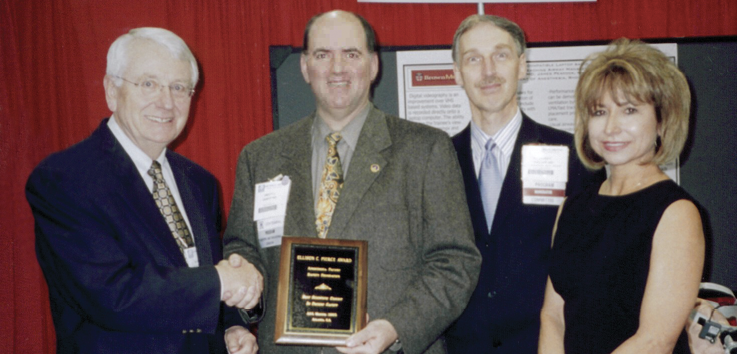
Dr. Stoelting presents the Ellison C. “Jeep” Pierce, Jr., MD, Best Scientific Exhibit in Patient Safety Award at the 2005 ASA meeting. This annual award encourages development of patient safety projects from all anesthesia professionals. The award in 2005 was for the project “Macintosh- and IBM-compatible Laptop-based Videography of Airway Management for Teaching Airway Management and Record Keeping” from Brett L. Arron, MD, Richard Gillerman, MD, and James E. Peacock, RN
Setting Audible Critical Alarms
Bob overcame controversy to steer APSF to make a strong statement about the need to set critical audible alarms, rather than disabling them to avoid possible false positive signals that subsequently could lead to unsafe situations or adverse events (https://www.apsf.org/newsletters/html/2004/winter/01workshop.htm).
CO2 Absorbent Interactions with Volatile Anesthetics
This was the topic of the first APSF consensus conference (2005), which was convened because of the concern for the potentially dangerous by-products and flammable reactions that could occur with exposure of volatile anesthetics to CO2 absorbent. This meeting led to solid recommendations promulgated through the APSF Newsletter (https://www.apsf.org/newsletters/html/2005/summer/01co2.htm).
Monitoring to Prevent Postoperative Respiratory Depression or Opioid-Induced Ventilatory Impairment (OIVI)
Through Bob’s leadership and advocacy, APSF has taken a strong stand to promote postoperative monitoring for early detection of respiratory depression related to residual opioids. APSF has hosted multiple consensus conferences and workshops on this topic as well as produced an educational video for prevention of this high acuity patient safety issue (https://www.apsf.org/newsletters/html/2007/winter/01_opioids.htm; https://www.apsf.org/resources/oivi/).
Beach Chair Position
The hazards of positioning with inadequate cerebral perfusion were identified, and research into this important issue was funded. Potential preventive measures, such as maintenance of adequate cerebral perfusion using correction for height differences between the brain and the site of blood pressure measurement, were recommended. As a result, awareness of this patient safety issue has been heightened among anesthesia professionals today (https://www.apsf.org/newsletters/html/2009/spring/01_cerebral.htm; https://www.apsf.org/newsletters/html/2010/winter/01_workshop.htm).
Medication Safety
This has been one of Bob’s great interests. The APSF has convened several workshops and consensus conferences on this topic, produced an educational video, and published numerous reports and articles on it in the APSF Newsletter. While awareness of this issue surely is higher, deep solutions that stick are still elusive. The APSF has advocated for the “Standardization, Technology, Pharmacy/Pre-filled/Pre-Mixed, Culture (STPC)” paradigm for optimal management of medications (https://www.apsf.org/newsletters/html/2010/spring/01_conference.htm; https://www.apsf.org/resources/med-safety/).
Postoperative Visual Loss
Bob worked alongside multiple organizations and stakeholder groups to educate providers about this topic and promoted research and preventive efforts. The APSF convened a consensus conference and produced an educational video on this debilitating patient safety issue (https://www.apsf.org/newsletters/html/2013/winter/06_conference.htm; https://www.apsf.org/resources/povl/).
Emergency Manuals/Checklists
Bob spearheaded and co-chaired the 2015 Annual APSF Consensus Conference on Implementing Emergency Manuals/Checklists. The conference attendees and faculty concluded that the APSF could play a lead role in advocating, educating, and researching the implementation of the highest quality manuals/checklists in the operating room to make patients safer (https://www.apsf.org/newsletters/html/2016/February/08_EmerManuals.htm).
Videos Dissemination of APSF Initiatives
Approximately 10,000 copies of videos related to specific patient safety problems such as on-patient fires in the operating room, medication safety, opioid-induced ventilatory impairment, and postoperative visual loss have been distributed from APSF either via download or DVDs from the apsf.org website. The fire safety video alone has been distributed or accessed 8,000 times and is used to raise awareness and teach health care professionals how to prevent and respond to operating room fires (https://www.apsf.org/resources/fire-safety/).
Given Bob’s larger-than-life, well-deserved reputation in our specialty, those who don’t know him may think he’s very serious and formal. They would be mistaken. He has a remarkable sense of humor. It may not be immediately evident to those who don’t know him well and who respect him so much as a senior statesman for our specialty, but he’s a master of one-liners and self-deprecating stories. It’s these attributes that make him so good at leading meetings; they enable his team to discuss intense issues in a productive and even enjoyable environment. He is a prodigious worker. Most importantly, his love of his wife, Natalie, and family is inspiring. He genuinely cares for people and has a warmth and charm that shine when he sees mentees succeed.
All of us on the Executive Committee are happy for Bob that he has chosen to move on to the next phase of his life. He’s still full of vigor and will surely explore new and stimulating things. He also successfully steered us through the process of selecting his successor, Mark A. Warner, MD, fulfilling his responsibilities, as always, to APSF and the anesthesia community. He will be missed at the head of our EC table for all that he has brought these many years. We wish him the best and thank him for all that he has given to the APSF and to anesthesia patient safety. All patients having the experience of anesthesia are better off for his having been our selfless, dedicated, and effective leader.
Jeffrey Cooper currently serves as Executive Vice President of the APSF and he has been an active member of the APSF Executive Committee from 1985 to the present. He is also Professor of Anaesthesia at Harvard Medical School in the Department of Anesthesia, Critical Care & Pain Medicine, Massachusetts General Hospital, Boston, MA.
Reference
- APSF Newsletter. Winter 1997. https://www.apsf.org/newsletters/html/1997/winter/leadership.html. Last accessed 1/2/2017.
