“By failing to prepare, you are preparing to fail.”
Benjamin Franklin
Transcatheter Aortic Valve Replacement (TAVR) is quickly becoming an everyday procedure seen in operating rooms and cardiac catheterization suites throughout the country. With aortic stenosis being one of the most common valvular heart conditions in a continually aging population, these numbers are only expected to increase. To date, it is estimated over 200,000 TAVR procedures have been performed worldwide.1 It is imperative that anesthesia professionals have an understanding of this transformative procedure and the unique anesthetic challenges these patients present in order toprovide the safest level of care.
History of TAVR
TAVR was first performed as a proof-of-concept procedure by Cribier et al. in Paris, France, on April 16, 2002, on a patient with severe aortic stenosis and cardiogenic shock as a treatment of last resort.2 The patient experienced a dramatic improvement in his heart failure symptoms postoperatively, thus, demonstrating the feasibility of this remarkable new procedure. Since that moment 16 years ago, TAVR has seen a rapid evolution, and after being validated through several rigorous clinical trials,3-6 has now become a common, everyday procedure. TAVR has revolutionized the treatment of severe aortic stenosis since patients that were considered non-operable for traditional surgical aortic valve replacement (SAVR) due to significant comorbidities are now given this treatment option. Many of these patients go on to experience sustained quality of life with improved functional status for many years,3 whereas medically managed patients have a 1-year mortality of 51% and an average survival of only 1.8 years.6 TAVR has been accepted by the American Heart Association/American College of Cardiology (AHA/ACC) as a Class I indication and is considered the standard of care in these non-operable* patients and as a Class IIa indication in patients who are operative candidates but at high-risk† for mortality and complications after SAVR.7 Now, with data from the PARTNER-2A randomized clinical trial that have demonstrated lower stroke and mortality rates for TAVR,8 the Federal Drug Administration has recently approved TAVR for intermediate-risk‡ patients.9 There is also an interest in advancing efforts to include the recommended use of TAVR as an alternative to SAVR for even low-risk§ patients, with two large randomized trials underway in the US.10
Overview of the Procedure
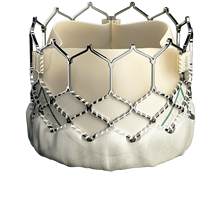
Figure 1. SAPIEN 3 Transcatheter valve. Courtesy of Edwards Lifesciences LLC, Irvine, CA. Edwards, Edwards Lifesciences, and SAPIEN 3 are trademarks of Edwards Lifesciences Corporation.
There are several commercially available TAVR systems approved for use in Europe and two in the United States. The two newest generation valve systems approved for use in the United States are the Sapien 3 (Edwards Lifescience, Irvine, CA, Figure 1) and the CoreValve Evolut-R (Medtronic, Minneapolis, MN, Figure 2). Both the Sapien and CoreValve systems are most commonly inserted via a retrograde transfemoral approach. For patients with ilio-femoral arterial access not amenable to this percutaneous technique due to severe peripheral vascular disease, tortuosity, or aortic disease, other options may include subclavian/axillary, transaortic, transapical, transcaval, and even a transcarotid approach. While both systems provide patients with similar outstanding outcomes,11,12 it is important to note that these two device systems differ in their deployment techniques that, in turn, have implications for the development of hemodynamic instability. The Sapien valve is a balloon-expandable device that requires rapid ventricular pacing (rate 160-220 beats/minute) at the time of deployment in order to minimize arterial pulse pressure and transaortic flow helping to reduce the risk of migration or ejection of the valve into the aorta. Conversely, the CoreValve is self-expanding and does not require pacing since it is gradually released into position. The CoreValve is a longer profile device that can also be partially recaptured in the sheath and repositioned if necessary. Balloon aortic valvuloplasty is occasionally performed to facilitate placement of either prosthetic valve. Rapid ventricular pacing is routinely employed during this step as well.
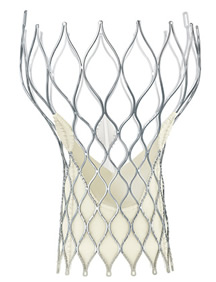
Figure 2. The Medtronic CoreValve® Evolut R Transcatheter Valve. Courtesy of Medtronic, Inc.,Minneapolis, MN.
While the vast majority of patients spontaneously recover from these brief pacing episodes, management of continued hemodynamic instability must be prompt. Patients with severe aortic stenosis and concomitant left ventricular hypertrophy do not tolerate hypotension for an extended period of time due to lack of coronary flow reserve and perfusion mismatch, even in the absence of coronary disease. Interventions can range from bolus vasopressor administration for transient hypotension to defibrillation for induced ventricular fibrillation and initiation of cardiopulmonary bypass for sustained hypotension, coronary occlusion, or annular rupture. Patients with pre-existing first-degree atrioventricular block, left anterior hemiblock, right bundle branch block, and those receiving a CoreValve are at higher risk of requiring pacing immediately after valve deployment as well as postoperatively.13 Since the CoreValve structure extends more deeply into the left ventricular outflow tract where the atrioventricular conduction system passes superficially, these patients are particularly at risk. A reliable mechanism for immediate pacing is required for all TAVR patients but a heightened sense of awareness is needed for patients with these preoperative electrocardiogram abnormalities and those receiving the CoreValve.
General versus Monitored Anesthesia Care (MAC):
Although the first TAVR was performed with local anesthesia and minimal sedation in a moribund patient, the early stage of TAVR development saw almost uniform use of general anesthesia. It is still the most common type of anesthesia used today in the United States.14 General anesthesia allows for more control of the procedural environment with a secure airway and completely immobile patient. Since ventilation is controlled, a period of apnea can be provided that may help avoid unnecessary movement of the heart during deployment of the valve. It also gives the cardiologist as much time as needed to perform the procedure. In addition, general anesthesia allows for the use of transesophageal echocardiography (TEE), in particular 3D TEE, to assist with positioning of the valve, the assessment of any paravalvular regurgitation, and immediate diagnosis of cardiac perforation if hypotension is persistent. TEE is also valuable in assessing under-filling of the left ventricle as an etiology of rapid or unfavorable hemodynamic changes. In the earlier stages of TAVR development, general anesthesia was warranted when there was a higher complication rate and the duration of the procedure was longer.
Presently, with recent technological advancements in the newer generation TAVR systems, along with better operator experience and implementing standardized protocols, there has been a much lower complication rate and a trend toward using MAC anesthesia. Some of the TAVR innovations that have permitted this transition to MAC anesthesia include significantly lower profile delivery systems, less paravalvular regurgitation from improved valve design, and enhanced device delivery systems.1 Although MAC anesthesia is now being used in many uncomplicated cases, general anesthesia is still required for most nontransfemoral approaches, in some high-risk patients, and when TEE guidance is used, such as in patients with chronic kidney disease to help minimize the use of x-ray contrast for procedure guidance.
Many high-volume centers now use almost exclusively MAC anesthesia as part of a streamlined process known as “minimalist” TAVR.15,16 When the vasculature of the patient is amenable to a percutaneous transfemoral approach, this method streamlines the entire perioperative process by using MAC anesthesia, intraoperative transthoracic echocardiography (TTE), reduction or elimination of pre-implantation balloon valvuloplasty, and well-defined postoperative care plans.1 The possible benefits of MAC over general anesthesia include less hemodynamic instability from anesthetic drugs, the avoidance of intubation and mechanical ventilation, faster postoperative recovery, and the ability to monitor for central nervous system embolic events. Since TTE, and not TEE, is used to evaluate the prosthetic valve after deployment, the ability to diagnose paravalvular regurgitation may be limited; however, with newer valve design modifications and more precise valve-sizing algorithms, the rate of paravalvular regurgitation has decreased significantly.1 In cases where aortography shows no paravalvular leak, patent coronary arteries, and good prosthetic position, there is no need for immediate post implant echo imaging. This latter point helps reduce procedure time and decreases the demands on the echocardiography staff and physicians.
Another potential benefit to a minimalist technique is reducing the incidence of postoperative delirium (PD). These patients are at unique risk for developing PD given their advanced age, frailty, and significant comorbidities. Abawi and colleagues recently published a retrospective observational study demonstrating PD was more frequent in nontransfemoral approaches (50% vs 10%, p<0.001) and in those that received general anesthesia (50% vs. 15%, p<0.001).17 Since all nontransfemoral procedures were performed under general anesthesia, it could not be determined whether there was an independent effect from the type of anesthesia (general vs. MAC). A more important factor in PD may be that patients with severe vascular disease, relegated to a nontransfemoral approach, are at higher risk for cerebral emboli and ischemia during the procedure. Moreover, nontransfemoral procedures involve a longer intensive care unit stay, more pain and opioid use, and more postoperative inflammation, which all may lead to PD. Further studies investigating whether the anesthetic type can lead to decreased postoperative delirium are forthcoming.
Although previous small studies did not reveal a difference in short or intermediate-term survival between general and MAC anesthesia,18-20 recent data are emerging that MAC anesthesia may be associated with improved outcomes. The largest observational TAVR study to date compared outcomes in patients who received general anesthesia or MAC anesthesia in all 10,997 patients who underwent TAVR in the United States from April 2014 through June 2015.14 The success of the procedure was comparable between the two techniques; however, MAC patients had significantly lower 30-day mortality (2.9% vs. 4.1%, p=0.029), a lower composite mortality and/or stroke rate (4.8% vs. 6.4%, p=0.019), and a shorter hospital length of stay (6 d vs. 6.7 d, p<0.0001). Even though these advantages remained after a propensity matched analysis, as a retrospective observational study, selection bias could have unintentionally been introduced into the data since non-transfemoral patients generally have more co-morbid conditions. For instance, outcomes may be better using MAC anesthesia solely because it is a much more common technique at high-volume centers than at emerging programs that employ general anesthesia and where operators encounter a steep learning curve. Although it is unknown whether anesthesia type is directly associated with improved outcomes without a prospective, randomized study, these data clearly signify a trend towards an increasing number of programs performing TAVR without general anesthesia. From April 2014 until June 2015, the percentage of programs employing moderate sedation or MAC increased from 10% to almost 30%.14 This transition from general to MAC anesthesia has largely already occurred internationally, where TAVR has been in general use for several more years than in the US.
There still are risks associated with TAVR performed under MAC anesthesia. The anesthesia provider must always be prepared for any contingency plan and be able to convert to a general anesthetic promptly. The rate of conversion to general anesthesia in most recent experience is under 2%, but has been reported as high as 5-6%.14 The most dramatic cases are when annular rupture or cardiac perforation occur. Embolization of the TAVR valve into the left ventricle may require rapid conversion to open surgery. In smaller patients, the delivery system can obstruct the arterial supply to a lower extremity causing ischemia and pain, let alone arterial dissection. Furthermore, many of these elderly patients also suffer from spinal stenosis and remaining motionless in the supine position after a period of time can be nearly impossible, necessitating conversion to a general anesthetic. Therefore, it may be prudent to have airway equipment (laryngoscopes, endotracheal tubes, laryngeal mask airway), vasopressors, and blood checked and ready for any critical life threatening situation that may arise. Moreover, open communication between all operating room team members, both before and during the procedure, is particularly important to avoid preventable complications. This “heart team” collaborative model has a Class I indication from the AHA/ACC as it seeks to optimize patient safety and clinical outcomes.7
Summary
TAVR has revolutionized the care of patients with severe aortic stenosis, proving in randomized comparisons with standard surgery to be a superior treatment alternative to SAVR in patients that are at prohibitive, high, and intermediate surgical risk. Recent data demonstrate MAC anesthesia provides a similar rate of procedural success when compared to general anesthesia; however, whether MAC anesthesia actually leads to improved patient safety and better outcomes in these patients remains to be elucidated. While technological advances and a low complication rate allowed for the introduction of the minimalist TAVR approach under MAC anesthesia, the anesthesia provider must always be prepared to address problems that may arise. A well-designed and thoughtful anesthetic plan should always be accompanied by an understanding of the sequence of steps involved in the TAVR procedure so that hemodynamic perturbations and procedural complications can be anticipated and addressed appropriately. As TAVR moves toward use in low risk patients, the importance of readiness to manage catastrophic complications becomes even more important. There should be contingency plans for anything from major hemodynamic changes and catastrophic complications to intolerance to MAC anesthesia.
* non-operable definition is challenging but agreed to be >50% mortality at 30 days or irreversible morbidity1
† Society of Thoracic Surgeons (STS) predicted risk of operative mortality score ≥10% or at a ≥15% risk of mortality at 30 days3
‡ STS predicted risk of operative mortality score ≥4% and ≤8%8
§ STS predicted risk of operative mortality score 2%10
Todd Novak is an attending anesthesiologist at NorthShore University HealthSystem and Clinical Assistant Professor at the University of Chicago Pritzker School of Medicine.
Suraj Parulkar is an attending anesthesiologist at Northwestern Memorial Hospital and Clinical Instructor of Anesthesia at the Northwestern Feinberg School of Medicine.
None of the authors have any disclosures pertinent to this manuscript.
We would like to acknowledge Ted Feldman, MD, Director of the Cardiac Catheterization Laboratory, NorthShore University HealthSystem and Michael Salinger, MD, Clinical Assistant Professor of Cardiology, NorthShore University HealthSystem for assistance in review of the manuscript. Dr. Feldman has received research grants and has served as a consultant for Abbott, Edwards, BSC and Gore. Dr. Salinger has served as proctor and consultant for Edwards Laboratories Sapien TAVR valve and Boston Scientific Lotus TAVR valve.
References
- Vahl TP, Kodali SK, Leon MB. Transcatheter aortic valve replacement 2016: a modern-day “through the looking-glass” adventure. J Am Coll Cardiol 2016;67:1472–1487.
- Cribier A, Eltchaninoff H, Bash A, et al. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description. Circulation 2002; 106:3006-8.
- Mack MJ, Leon MB, Smith CR, et al. PARTNER 1 trial investigators. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet 2015; 385: 2477–2484.
- Reardon MJ, Adams DH, Kleiman NS, et al. 2-Year outcomes in patients undergoing surgical or self-expanding transcatheter aortic valve replacement. J Am Coll Cardiol 2015;66:113–121.
- Thyregod HG, Steinbruchel DA, Ihlemann N, et al. Transcatheter versus surgical aortic valve replacement in patients with severe aortic valve stenosis: 1-year results from the all-comers NOTION randomized clinical trial. J Am Coll Cardiol 2015;65:2184–2194.
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med 2010; 363:1597-607.
- Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 63: e57-e185.
- Leon MB, Smith CR, Mack MJ, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med 2016; 374: 1609-20.
- FDA News Release. August 18, 2016. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm517281.htm
- The safety and effectiveness of the SAPIEN 3 Transcatheter Heart Valve in low risk patients with aortic stenosis (PARTNER 3). https://clinicaltrials.gov/ct2/show/NCT02675114
- Abdel-Wahab M, Neumann FJ, Mehilli J, et al. 1-Year outcomes after transcatheter aortic valve replacement with balloon-expandable versus self-expandable valves: results from the CHOICE randomized clinical trial. J Am Coll Cardiol 2015; 66: 791-800.
- Abdel-Wahab M, Mehilli J, Frerker C, et al. Comparison of balloon-expandable vs. self-expandable valves in patients undergoing transcatheter aortic valve replacement: the CHOICE randomized clinical trial. JAMA 2014; 311: 1503-1514.
- Siontis GCM, Jüni P, Pilgrim T, et al. Predictors of permanent pacemaker implantation in patients with severe aortic stenosis undergoing TAVR: a meta-analysis. J Am Coll Cardiol 2014; 64: 129-140.
- Giri, J. Moderate sedation vs. general anesthesia for transcatheter aortic valve replacement: An STS/ACC Transcatheter Valve Therapy Registry analysis. SCAI Annual Meeting, May 2016.
- Motloch LJ, Rottlaender D, Reda S, et al. Local versus general anesthesia for transfemoral aortic valve implantation. Clin Res Cardiol 2012; 101:45-53.
- Kasel AM, Shivaraju A, Schneider S, et al. Standardized methodology for transfemoral transcatheter aortic valve replacement with the Edwards Sapien XT valve under fluoroscopy guidance. J Invasive Cardiol 2014; 26: 451-461.
- Abawi M, Nijhoff F, Agostino P, et al. Incidence, predictive factors, and effect of delirium after trancatheter aortic valve replacement. JACC Cardiovasc Interv 2016; 25;9:160-8
- Gauthier C, Astarci P, Baele P, et al. Mid-term survival after transcatheter aortic valve implantation: results with respect to the anesthetic management and to the access route (transfemoral versus transapical). Ann Cardiac Anaesthesia 2015;18: 343-35.
- Oguri A, Yamamoto M, Mouillet G, et al. Clinical outcomes and safety of transfemoral aortic valve implantation under general versus local anesthesia. Circ Cardiovasc Interv 2014;7:602-610.
- Balanika M, Smyrli A, Samandis G, et al. Anesthetic management of patients undergoing transcatheter aortic valve implantation. J Cardiothoracic and Vasc Anesth 2014; 28:285-289.
