The 2015 Ellison C. Pierce, Jr., MD, ASA/APSF Patient Safety Memorial Lecture

Dr. Mark A Warner
Mark A. Warner, MD, presented the 2015 Pierce ASA/APSF Patient Safety Memorial Lecture. He started by reviewing the anesthesia patient safety imperative that anesthesiology has embraced since the creation of the APSF in 1985: “no patient shall be harmed by anesthesia.” The APSF used that visionary statement to create goals that still stand today. They specifically state that the foundation will:
- Foster investigations that will provide a better understanding of preventable anesthetic injuries
- Encourage programs that will reduce the number of anesthetic injuries
- Promote national and international communication of information and ideas about the causes and prevention of anesthetic injuries
The following summarizes Dr. Warner’s comments from the lecture.
Improvement in anesthetic mortality and several major morbidities was dramatic during the first decade of the APSF…and anesthesia care has continued to become safer. The specialty provides outstanding, very safe patient care intraoperatively.
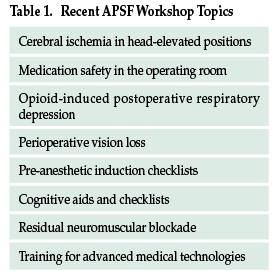
With all of that, the anesthesia community can and must continue to improve because patients are still harmed—every day—in the U.S. and elsewhere, during and by anesthesia care. There is still much to study, assess, and improve intraoperatively. Issues that have recently been discussed during workshops of the APSF are shown in Table 1.
Unfortunately, overall surgical and procedural safety lags. The incidences of a variety of major perioperative morbidities as well as death rates clearly remain unacceptably high. Within anesthesiology, and working with health care colleagues outside of our specialty, we should, can, and must improve both intraoperative and perioperative patient safety. This is where the Perioperative Surgical Home concept comes into play.
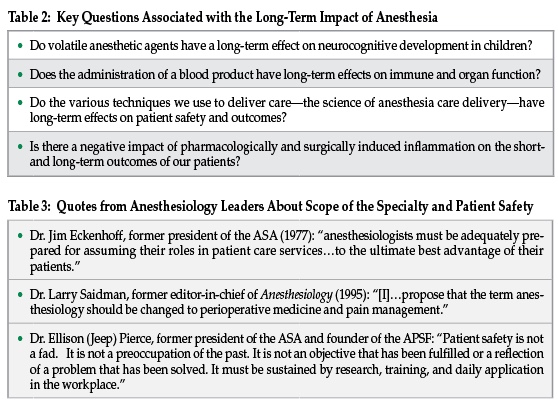
In general, we have not looked intensely into the long-term consequences of anesthesia care. That is changing—data are increasingly strong that there are prolonged physiologic and pathologic changes associated with intraoperative anesthesia care. Several key questions for 2015 are shown in Table 2. Anesthesiologists and members of the anesthesia care team are well positioned to design, assess, and improve perioperative care of patients who will be anesthetized for surgical, diagnostic and therapeutic procedures.
How can the anesthesia community expand its influence in the perioperative period and improve patient safety? Let’s look at several examples.
Penicillin Allergy: Nearly 90% of surgical patients in the U.S. who indicate that they have a penicillin allergy—do not have that allergy. Anesthesiologists and surgeons rarely check, instead ordering broad spectrum third and fourth generation antibiotics because it is expedient. Unfortunately, there is a cost to society and patient safety. Unfiltered, proliferate use of these high-end antibiotics is expensive and supports the evolution of resistant bacteria—and these resistant bacteria, of course, require more expensive antibiotics that have an increased proportion of adverse effects. Simple preoperative protocols can result in skin tests that document the presence or absence of true penicillin allergies. Anesthesiologists, surgeons, and infectious disease specialists or internists, can readily work together to develop facility-specific clinical protocols to check for penicillin allergies preoperatively.
Prehabilitation: Anesthesiologists and the teams with whom they work can develop preoperative evaluation processes that extend beyond the typical pre-anesthetic assessment—beyond the ubiquitous “OK for anesthesia.” Issues that have yet undefined contributions to perioperative morbidity and mortality such as weight control, correction of general or specific nutrition deficits, cessation of smoking, and improvement of poor physical conditioning all merit additional study and, when appropriate, implementation of clinical protocols that may “prehabilitate” patients before they proceed through the perioperative process.
Blood Product Transfusion: Extensive use of algorithms and clinical protocols for transfusion of blood products can have a significantly positive impact on patient safety during the perioperative period. In a wide variety of clinical settings, the use of predetermined transfusion protocols and mechanisms to proactively intervene when physicians transfuse blood products outside of agreed algorithms have reduced blood product use 40–60%. Blood transfusion has distinct and measurable detrimental impact on immune responses and susceptibility to infection in surgical patients, especially those undergoing procedures in body parts that have high concentrations of dwelling bacteria. Colorectal surgery is a good example.
Blood products contain much debris, including free hemoglobin and cellular stroma that can be toxic to organs such as kidneys. Processes that lead to reductions in blood transfusion are cost-effective, improve patient care in these settings, and help avoid prolonged disability, sepsis, and multi-organ failure. Approximately 40% of all blood products are transfused into surgical and procedural patients. The specialty is perfectly positioned to take lead roles in developing new algorithms or modifying existing algorithms for their specific practices and patient populations. In collaboration with transfusion medicine specialists, surgeons, and proceduralists, anesthesiologists and their care teams can work within health care settings to design and implement successful processes to reduce4,5 the use of blood products and decrease perioperative complications.
Human factors: Each step in a clinical pathway or process, whether it has been designed or occurred naturally, increases the opportunity for human error. Anesthesiologists, working closely with their health care colleagues and system engineers, can analyze, design, assess and continuously improve perioperative care pathways and processes by eliminating unnecessary steps. It is the right thing to do financially—reducing steps decreases expenses and increases efficiency. It is the right thing to do clinically—reducing steps decreases errors. It is the right thing to do for our patients—reducing steps decreases complications and increases patient safety.
Expansion of anesthesia care beyond intraoperative management and into an encompassing perioperative setting makes sense clinically because patients will benefit. It is another step forward in expanding the influence of the specialty in the safety of patients who are anesthetized for their surgical and procedural care.
Visionary leaders of the specialty during the past generation have noted that anesthesia care must evolve. Table 3 provides several of the quotes taken from selected ASA Rovenstine Lectures. These visionary colleagues had it right—expansion of the specialty to encompass perioperative care is necessary BECAUSE IT IS THE RIGHT THING TO DO FOR OUR PATIENTS.
I propose that the APSF reconsider its vision statement, “No patient shall be harmed by anesthesia.” It is now time that the statement should read, “No patient undergoing an anesthetic shall be harmed in the perioperative period.” This is the imperative you want to follow if you wish to expand the influence of the specialty into the future. This is the imperative you want to follow if you wish to have a greater influence on patient safety. This is the imperative you wish to have followed if you are the patient.”
Dr. Warner is Professor of Anesthesiology and Executive Dean at the Mayo Clinic College of Medicine in Rochester, Minnesota.
