 Language barriers in health care are not benign, and they contribute to disparities in care and outcomes for patients who do not speak English well as compared to English-speaking patients. Individuals with “limited English proficiency” (LEP) are defined by the U.S. Department of Health and Human Services as those “who do not speak English as their primary language and who have a limited ability to read, write, speak, or understand English.”1 The Agency for Healthcare Research and Quality identified five high-risk scenarios for LEP patients: medication reconciliation, patient discharge, informed consent, emergency department care, and surgical care. Anesthesia professionals may be involved in every one of these high-risk scenarios.2 LEP patients are at greater risk for surgical delays, surgical infections, falls, pressure ulcers, and readmissions.3
Language barriers in health care are not benign, and they contribute to disparities in care and outcomes for patients who do not speak English well as compared to English-speaking patients. Individuals with “limited English proficiency” (LEP) are defined by the U.S. Department of Health and Human Services as those “who do not speak English as their primary language and who have a limited ability to read, write, speak, or understand English.”1 The Agency for Healthcare Research and Quality identified five high-risk scenarios for LEP patients: medication reconciliation, patient discharge, informed consent, emergency department care, and surgical care. Anesthesia professionals may be involved in every one of these high-risk scenarios.2 LEP patients are at greater risk for surgical delays, surgical infections, falls, pressure ulcers, and readmissions.3
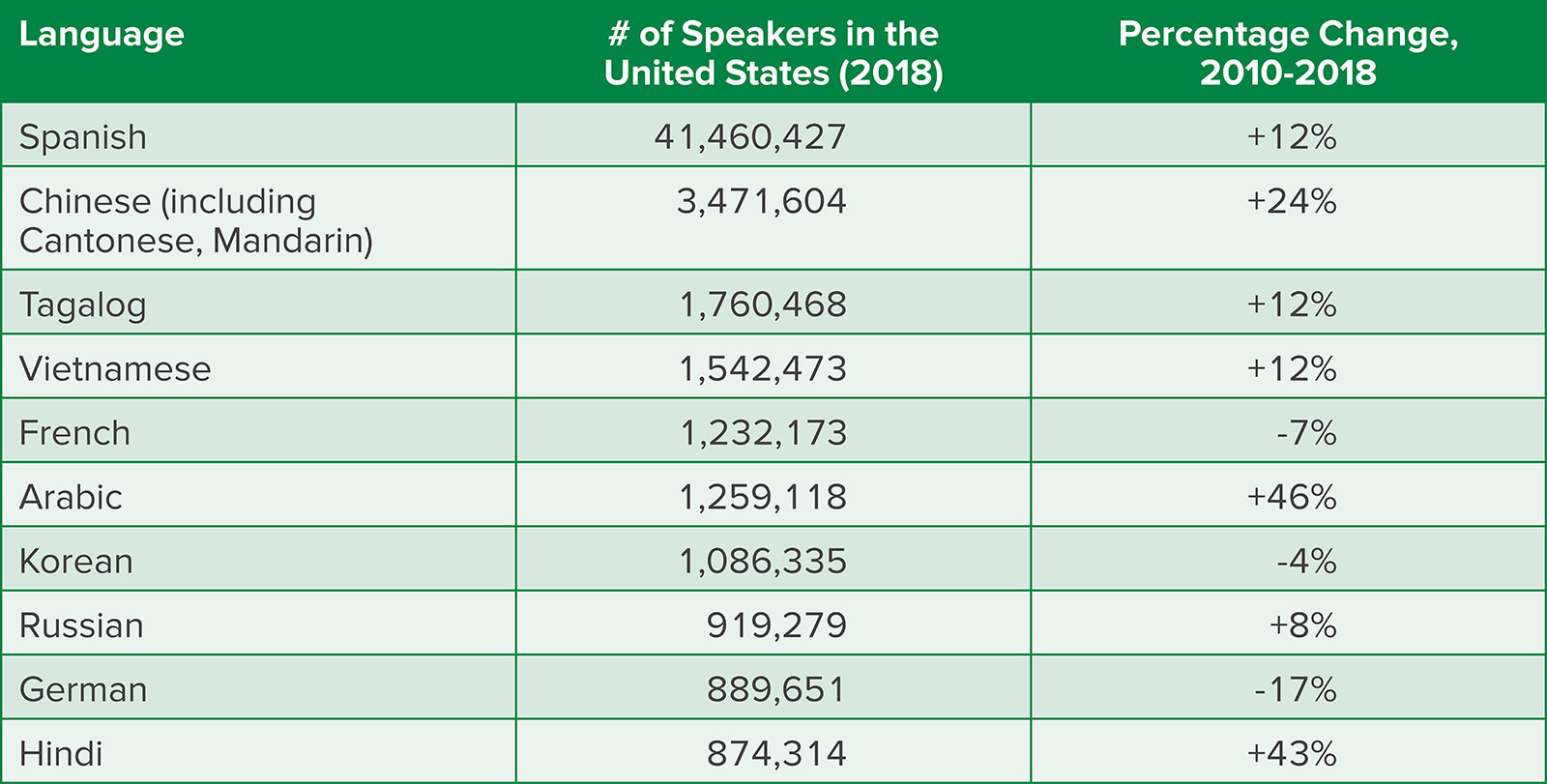
Linguists recognize more than 7,000 languages, and 1,333 of these are catalogued by the United States Census Bureau.4 Although precise counts are elusive, the U.S. Census Bureau reports speakers from forty-two different language groups;4 ten of the most common non-English languages spoken at home in the United States are shown in Table 1. As patients speaking these languages present for health care, it is important to recognize the unique needs of patients who do not speak the most common language(s) in any given setting. In the United States, English is the de facto language of government, health care, and commerce. In 2019, 21.5% of the U.S. population reported speaking a language other than English at home, and 8.2% of the US population were reported to have limited English proficiency.5 Title VI of the U.S. Civil Rights Act of 1964 requires that recipients of federal financial assistance take reasonable steps to make their programs, services, and activities accessible by eligible persons with LEP.6 Federal financial assistance programs include health care providers and hospitals who participate in CHIP, Medicaid, and Medicare. To make themselves accessible to LEP patients, hospitals must therefore provide translation of written word and interpretation of spoken word.
Table 1: Languages Spoken by Those Who Speak Languages Other Than English at Home, United States.11
The United States Department of Health and Human Services (HHS) offers a free online educational program to assist organizations and individual providers in assessing their readiness to provide care for LEP patients and teaching the HHS Office of Minority Health Standards for Culturally and Linguistically Appropriate Services in Health and Health Care.7 Below, we provide some important highlights of care for LEP patients.
When providing care to LEP patients, clinicians must assess when interpretation services are needed. The Joint Commission states, “Because communication is a cornerstone of patient safety and quality care, every patient has the right to receive information in a manner he or she understands.”8 For optimal care, interpretation services should be involved any time there is a need for two-way communication with the patient. Interpretation can be provided in person by a trained clinician, trained clinical staff member, or dedicated interpreter. Additionally, there are many companies that provide either audiovisual or audio-only interpretation. Providers familiarize themselves with the specific resources available in their health care system.
Trained interpreters are part of the health care team and receive between 40 and 120 hours of training prior to their first day on the job. Untrained interpreters have been shown to make twice as many errors as trained interpreters.9 To be eligible as a trained interpreter, an individual must speak English and the desired non-English language, as well as be versed in medical terminology in both languages. When interpretation services are being utilized, the health care professional should start the conversation by letting the interpreter know what to expect from the encounter prior to beginning a conversation. The conversation should be directly with the patient, not the interpreter. After the conversation, the interpreter’s name or ID number should be documented in the chart for that patient encounter.
Sometimes, providers use suboptimal interpretation options including the patient’s family members, staff members with limited fluency or medical language, Google Translate, or “just winging it.” It can be especially tempting to use family members as interpreters given their familiarity with the patient, availability in the moment, and lack of cost. However, most family members lack the training of official interpreters, including knowledge about and sensitivity to confidentiality concerns.2 Well-meaning family members may censor or change the information that the provider is sharing, which degrades the patient’s individual autonomy. Family members may also participate in the discussion between provider and patient rather than acting solely as interpreter. Minor children are especially problematic interpreters given family power dynamics and their limited understanding of medicine or the overall situation; children should not be used as interpreters except in emergencies.10 Some organizations allow patients to request a family member as an interpreter; this can be appropriate, but clinicians may have to make a judgment about the patient’s level of autonomy when such a request is made. In keeping with patient autonomy, patients may reject the offer for professional interpretation services, but these services should still be offered in each interaction.
When caring for LEP patients, three foundational principles apply. First, these patients are limited in their English proficiency, which does not mean a complete lack of English understanding. Patients who are conversant in simple English (e.g., they can greet the health care team in English) may still need interpretation services for adequate understanding of their health care. Second, a patient’s ability to speak English bears no relationship to their intelligence or medical sophistication. To reinforce this point, it can be helpful to imagine oneself as an anesthesia or perioperative professional seeking emergency care and not being able to communicate directly with the health care team. Third, every patient has the right to communicate directly with their health care team. To appropriately provide care to these patients, it is best to allot extra time while minimizing distractions. If possible, keeping the device for accessing remote interpretation services at the bedside can remove a barrier in use. Knowing the appropriate policies regarding interpretation can avoid awkward conversations with family members. Prescheduling in-person interpretation can streamline the entire process, especially for family meetings or other preplanned conversations. Partnerships with patients and between members of the care team can streamline care for LEP patients, enabling both efficient care and care that meets the needs of this vulnerable group.
As the United States continues to have a growing LEP population, clinicians will see increasing numbers of LEP patients. Having a plan in place for effectively communicating with LEP patients can help reduce strain on a provider while also maintaining a strong relationship with the patient. Trained interpretation staff are an important part of the health care team and allow patients to be truly informed throughout their medical journey. Providing interpretation services for patients should be considered an aspect of providing the compassionate patient-centered care to which clinicians aspire.
Harrison Charwat, MD, is a PGY-1 Anesthesiology resident at the Hospital of the University of Pennsylvania.
Meghan Lane-Fall, MD, MSHP, FCCM, is vice chair of Inclusion, Diversity, and Equity and the David E. Longnecker Associate Professor of Anesthesiology and Critical Care at the Perelman School of Medicine of the University of Pennsylvania. and vice president of the Anesthesia Patient Safety Foundation.
The authors have no conflicts of interest.
References
- U.S. Department of Health and Human Services. Office for Civil Rights. Guidance to federal financial assistance recipients regarding Title VI and the prohibition against national origin discrimination affecting limited English proficient persons – summary. Updated 7/26/2013. Accessed April 7, 2022, https://www.hhs.gov/civil-rights/for-providers/laws-regulations-guidance/guidance-federal-financial-assistance-title-vi/index.html.
- Betancourt JR, Renfrew MR, Green AR, Lopez L, Wasserman M. Improving patient safety systems for patients with limited English proficency: a guide for hospitals. 2012. 12-0041. Accessed December 8, 2022. https://www.nmhe.org/case-specific-resources/2020/5/21/improving-patient-safety-systems-for-patients-with-limited-english-proficiency-a-guide-for-hospitals-2014.
- Betancourt JR, Tan-McGrory A. Creating a safe, high-quality healthcare system for all: meeting the needs of limited english proficient populations; comment on “Patient safety and healthcare quality: the case for language access.” Int J Health Policy Manag. 2014;2:91–94. PMID: 24639984.
- United States Census Bureau. About language use in the U.S. population. Updated 12/3/2021. Accessed April 7, 2022, https://www.census.gov/topics/population/language-use/about.html.
- United States Census Bureau. Why we ask questions about…language spoken at home. Accessed April 7, 2022, https://www.census.gov/acs/www/about/why-we-ask-each-question/language/.
- United States Department of Justice. Title VI of the Civil Rights Act of 1964. Accessed April 7, 2022, https://www.justice.gov/crt/fcs/TitleVI.
- U.S. Department of Health and Human Services. The guide to providing effective communication and language assistance services. Accessed April 7, 2022, https://thinkculturalhealth.hhs.gov/education/communication-guide.
- Joint Commission Division of Health Care Improvement. Overcoming the challenges of providing care to limited English proficient patients. Quick Safety: An advisory on safety & quality issues. 2021;13:1–3. Accessed April 7, 2022. https://www.jointcommission.org/-/media/tjc/newsletters/quick-safety-issue-13-lep-update-10-5-21.pdf.
- Nápoles AM, Santoyo-Olsson J, Karliner LS, et al. Inaccurate language interpretation and its clinical significance in the medical encounters of Spanish-speaking Latinos. Med Care. 2015;53:940–947. PMID: 26465121.
- Juckett G, Unger K. Appropriate use of medical interpreters. Am Fam Physician. 2014;90:476–480. PMID: 25369625.
- Zeigler K, Camarota SA. 67.3 Million in the United States Spoke a Foreign Language at Home in 2018. Center for Immigration Studies; 2019. Accessed April 7, 2022. https://cis.org/sites/default/files/2019-10/camarota-language-19_0.pdf.
