In March of this year, the U.S. Food and Drug Administration (FDA) approved naloxone hydrochloride nasal spray for over-the-counter, nonprescription use. This move was consistent with longstanding recommendations by the American Society of Anesthesiologists (ASA) and testimony given before several of its committees by ASA member Bonnie Milas, MD.1 The approval of naloxone for over-the-counter use by the Food and Drug Administration represents a nontraditional approach to managing opioid use, overuse or abuse, an approach referred to as “harm reduction.”
Whereas a “prevalence reduction” approach focuses on abstinence from behaviors that create risk, a harm reduction approach focuses on ameliorating the harmful consequences of the behavior.2,3 Although not without opposition from those who find the behavior morally objectionable, harm reduction presents a pragmatic approach to the mitigation of injury when behavior is difficult to modify.2 While harm reduction practices involving substance use are considered by some to be controversial, health care professionals routinely engage in other forms of harm reduction that are less contentious.3 A common example of this harm reduction approach is the prescription of cholesterol-lowering and antihyperglycemic medications to patients whose diet and exercise regimen are not optimal.
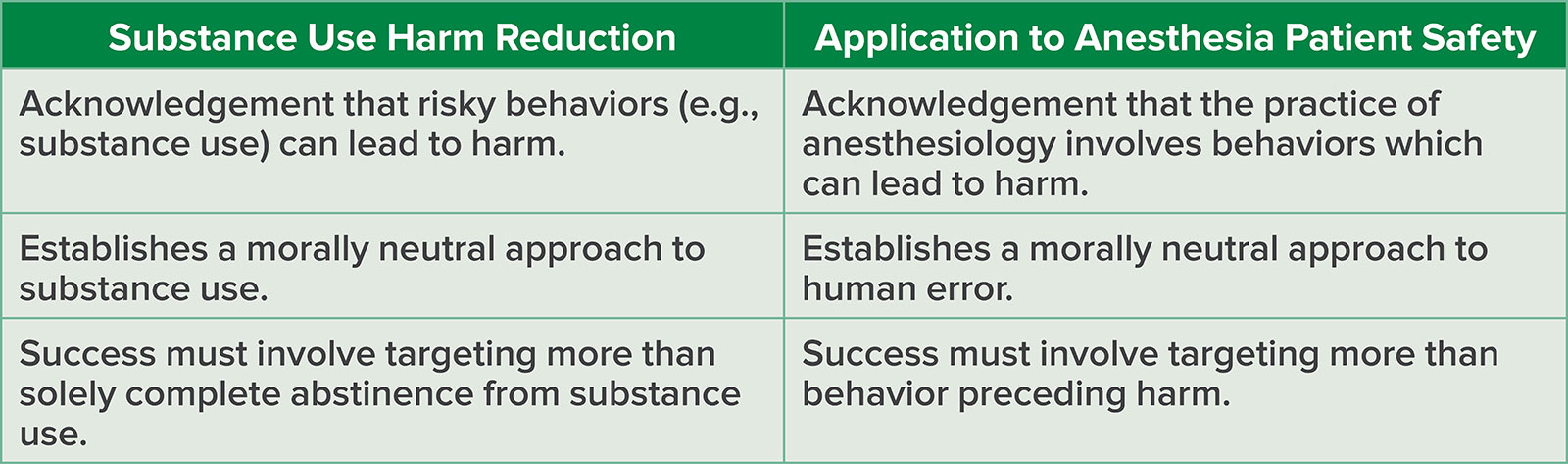
When we consider strategies to successfully address human error in anesthesiology, we can draw parallels to some of the core elements of a harm reduction approach (Table 1).4
Table 1: Analogy of Harm Reduction Approach with Substance Use and Anesthesia Patient Safety.
THE PRACTICE OF ANESTHESIOLOGY INVOLVES BEHAVIOR WHICH CAN LEAD TO HARM
The anesthesia work environment is complex, time-constrained, and stressful. Anesthesia professionals must negotiate the interactivity between the patient, equipment, medications, tasks, organization, and the surgical team. Simultaneously, they must remain vigilant, be able to multitask (or, more appropriately described, be able to rapidly switch between several tasks), and take actions with life-or-death consequences.5-7 The successful management of these multiple factors and how they affect each other is likely achieved the same way that pilots become adept at managing concurrent tasks, while simultaneously integrating unplanned tasks and rescheduling tasks. Such management requires substantial practice.8 In experienced pilots this strategy becomes largely automatic and does not require significant mental effort.8 Similarly, in studies involving anesthesia professionals, novices reported a higher degree of subjective workload than did experts for equivalent task loads.9 While great strides have been made over the years to improve the safety of patients undergoing anesthesia, the very nature of anesthesiology and the procedures for which patients require anesthesia will always have inherent risk, the elimination of which will never be completely possible. The harm which may occur as a result of anesthesia exists along a spectrum. Although the most severe degrees of harm are rare, it is nearly unavoidable for many anesthesia professionals during their career. It is also important to recognize that the harm which occurs to patients from error also extends to, and can have long-last effects upon, the anesthesia professional.10
MAKING ERRORS IS MORALLY NEUTRAL
The concept of human imperfection has been appreciated since biblical times.11 According to Shappell & Wiegmann, it is unreasonable to expect error-free performance from humans because, by their very nature, they make mistakes.12 Perrow estimated that human error accounted for 60–80% of accidents, an estimate similar to the work done by Cooper in the analysis of anesthesia-related incidents.13,14 In general, we make between 5 and 20 errors per hour depending on the type of work (manual vs. cognitive) and the circumstances in which the work is accomplished in (routine vs. urgent).15 The majority of these errors are prevented from causing harm by the systems in which we work, systems which include the very person making the error. The barriers, recoveries, and redundancies which prevent these errors from resulting in harm reflect the flexibility and resilience of the system. However, when certain circumstances involving the anesthesia professional such as fatigue, distraction, or the misinterpretation of clinical data or a warning alarm combine with certain patient factors, such as extensive comorbid disease and diminished physiologic reserve, the adaptive capacity of the system is no longer maintained, and harm can result.
Medical errors are often viewed as a moral failing, with a focus on blaming the individual for not being attentive enough or behaving in a way that is inconsistent with information which is only obvious to those viewing the situation with the benefit of hindsight.16,17 Health care professionals along the entire spectrum, from the most inexperienced, junior member of the team to the most senior are all prone to making errors.18 We’ve known for decades that the “blame approach” does not change the incidence of errors, rather it cloaks it in secrecy and makes the underlying causes difficult to address.19 Despite this knowledge, blame for making errors remains prevalent.20,21 It is important to consider that behavior can be seen as the cause of accidents even if the behavior itself is not attributed to impropriety or intentions of harm.22 The use of punitive language to describe this behavior is a symptom of a punitive safety culture.20 Creating a “Just Culture” is essential to the overall development of a robust safety culture in an anesthesia department.23 A Just Culture is not a system that is free of accountability, but rather one in which accountability is appropriately balanced between the individual and the system within which the individual practices.24 It is possible to hold individuals accountable without blame, and a similar model has been suggested for substance use.25,26
WE MUST RECOGNIZE THAT ONLY TARGETING BEHAVIOR PRECEDING HARM IS NOT PRACTICAL
Attempts to eliminate error-prone behavior continue to fail, and this approach is no longer accepted as a viable tactic by human factors experts.27 Resilience engineering and the Safety-II view reinforce this, as the processes underpinning human error are the same as those leading to acceptable outcomes, the difference being everyday performance adjustments.28,29 The Safety-II approach represents a fundamental change in the way that safety is viewed, shifting from examining what goes wrong (the traditional/Safety-I approach) to looking at what is necessary for acceptable outcomes to occur.29 The key to understanding how adverse outcomes occur is to have a thorough understanding of the human performance variability that is necessary for a satisfactory outcome.29 In this way, Safety-II is a proactive approach to safety management, as opposed to the reactive nature of the Safety-I approach. One of the essential components of Safety-II is attention to the system that shapes the variability in human performance. Harm reduction efforts that target modifications to the system are known to be more durable and effective than those that target modifying the behavior of individuals.30
INTEGRATING HARM REDUCTION PRACTICES IN ANESTHESIOLOGY SAFETY PROGRAMS
In summary, decreasing the harm from substance use and human error are problems that are intractable and resistant to solutions.31 This doesn’t mean that hope is lost, but rather that we need to approach these problems with different strategies than what we have employed in the past (Table 2). The behavior involved in the delivery of anesthesia can lead to harm, not just to patients, but also to ourselves. Errors are ubiquitous and anesthesia professionals of all experience levels will make them. When human behavior falls short of perfection, as it inevitably will, blame needs to be withheld as it will not prevent recurrence; making errors needs to be treated as morally neutral. A Just Culture approach of balancing accountability between the individual and the system provides a framework for reviewing harm events as well as designing systems that are more resilient. Since the same behaviors that lead to successful outcomes also can lead to harm, we must focus the majority of our efforts on designing systems that prevent harm rather than human error. Finally, we must train anesthesia professionals in safety as we would in any other field of science, and partner with safety professionals to better understand our complex systems.32
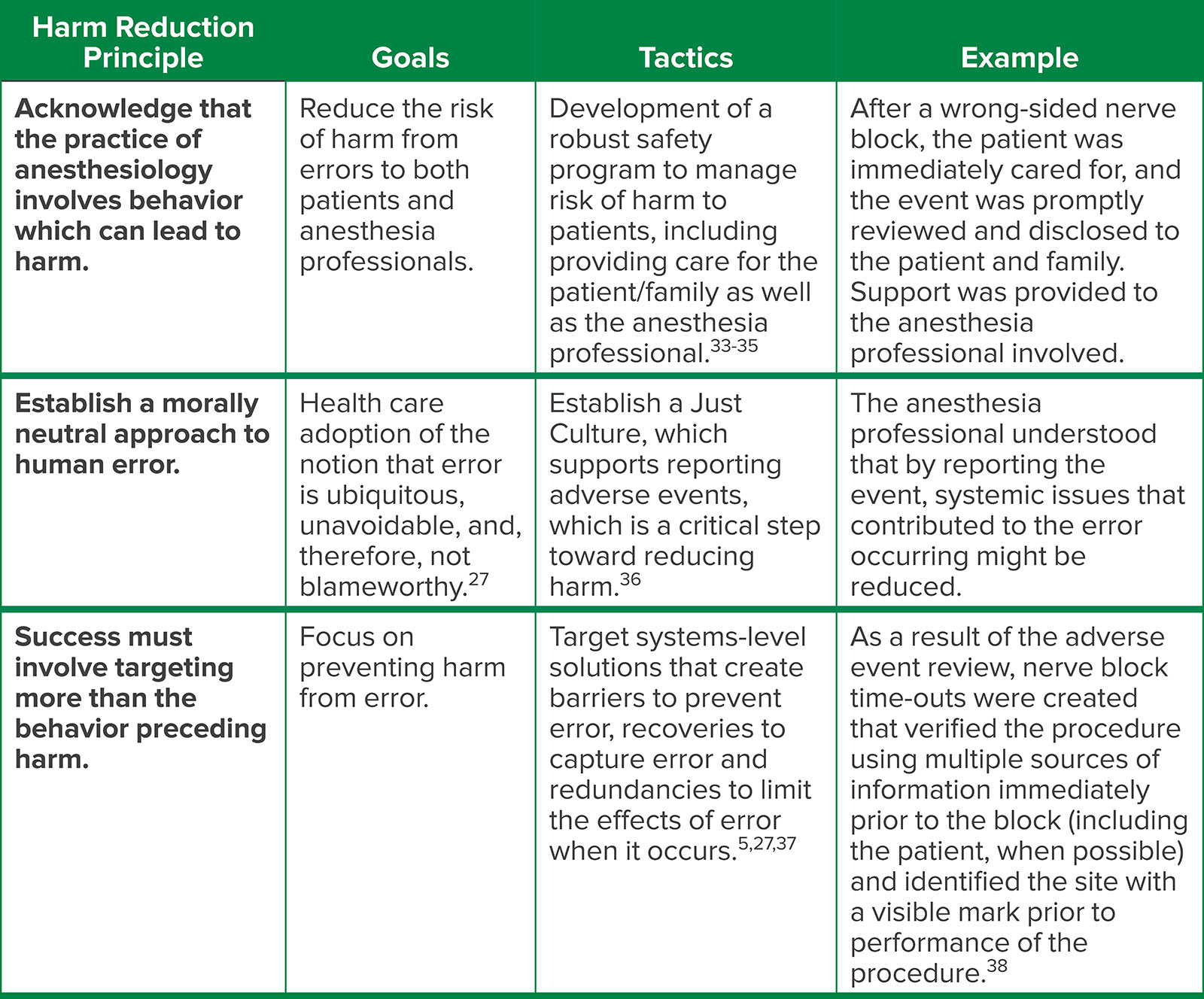
Table 2: An Example of Harm Reduction in Perioperative Care: Wrong-Sided Nerve Block.
Jonathan B. Cohen MD, MS is an associate member in the Department of Anesthesiology at Moffitt Cancer Center, Tampa, Florida, USA
The author has no conflicts of interest.
REFERENCES
- American Society of Anesthesiologists. FDA approves OTC naloxone consistent with longstanding ASA recommendations. March 29, 2023. https://www.asahq.org/advocacy-and-asapac/fda-and-washington-alerts/washington-alerts/2023/03/fda-approves-otc-naloxone-consistent-with-longstanding-asa-recommendations Accessed July 22, 2023.
- MacCoun RJ. Moral outrage and opposition to harm reduction. Criminal Law and Philosophy. 2013;7:83–98. https://doi.org/10.1007/s11572-012-9154-0 Accessed July 22, 2023.
- Stoljar N. Disgust or dignity? The moral basis of harm reduction. Health Care Anal. 2020;28:343–351. PMID: 33098488
- Marlatt GA, Larimer ME, Witkiewitz K. (Eds.). Harm reduction: pragmatic strategies for managing high-risk behaviors. Guilford Press; 2011.
- Carayon P, Wooldridge A, Hoonakker P, et al. SEIPS 3.0: Human-centered design of the patient journey for patient safety. Applied Ergon. 2020;84:103033. PMID: 31987516
- Weinger MB. Chapter 48: Human factors in anesthesiology. In: Carayon P, ed. Handbook of Human Factors and Ergonomics in Health Care and Patient Safety. 2nd ed. CRC Press; 2012:803–823.
- Gaba DM, Fish KJ, Howard SK, Burden A. Crisis management in anesthesiology. 2nd ed. Elsevier Health Sciences; 2014.
- Loukopoulos LD, Dismukes RK, Barshi I. The multitasking myth: handling complexity in real-world operations. Ashgate Publishing; 2009.
- Weinger MB, Herndon OW, Paulus MP, et al. An objective methodology for task analysis and workload assessment in anesthesia providers. Anesthesiology. 1994;80(1):77–92. PMID: 8291734
- Gazoni FM, Amato PE, Malik ZM, Durieux ME. The impact of perioperative catastrophes on anesthesiologists: results of a national survey. Anesth Analg. 2012;114:596-603. PMID: 21737706
- Yanklowitz, S. Pirkei Avot: A social justice commentary. CCAR Press; 2018.
- Shappell SA, Wiegmann DA. A human error approach to accident investigation: the taxonomy of unsafe operations. Int J Aviat Psychol. 1997;7:269–291. https://doi.org/10.1207/s15327108ijap0704_2
- Perrow C. Normal accidents: living with high risk technologies. Princeton University Press; 1999.
- Cooper JB, Newbower RS, Long CD, McPeek B. Preventable anesthesia mishaps: a study of human factors. Anesthesiology. 1978;49:399–406. PMID: 727541
- Conklin T. Pre-accident investigations: an introduction to organizational safety. Ashgate Publishing; 2012.
- Woods DD, Dekker S, Cook R, et al. Behind human error. 2nd ed. Ashgate Publishing; 2010.
- Lusk C, DeForest E, Segarra G, et al. Reconsidering the application of systems thinking in healthcare: the RaDonda Vaught case. Br J Anaesth. 2022;129:e61-e62. PMID: 35753806
- Dismukes K, Berman BA, Loukopoulos LD. The limits of expertise: rethinking pilot error and the causes of airline accidents. Ashgate Publishing; 2007.
- Leape LL. Testimony before the Subcommittee on Health of the Committee of Veterans’ Affairs House of Representatives One Hundred Fifth Congress First Session, United States, October 12, 1997.
- Fairbanks RJ, Kellogg KM. Mean talk: why punitive language in patient safety event reporting indicates a suboptimal safety culture. Ann Emerg Med. 2021;77:459–461. PMID: 33642129
- Anesthesia Patient Safety Foundation. Position statement on criminalization of medical error and call for action to prevent patient harm from error. May 25, 2022. https://www.apsf.org/news-updates/position-statement-on-criminalization-of-medical-error-and-call-for-action-to-prevent-patient-harm-from-error/ Accessed July 22, 2023.
- Holden RJ. People or systems? To blame is human. The fix is to engineer. Prof Saf. 2009;54:34–41. PMID: 21694753
- American Society of Anesthesiologists. Statement on Safety Culture. October 26, 2022. https://www.asahq.org/standards-and-guidelines/statement-on-safety-culture Accessed July 22, 2023.
- Marx D. Patient safety and the Just Culture. Obstet Gynecol Clin North Am. 2019;46:239–245. PMID: 31056126
- Timms M. Blame Culture is toxic. here’s how to stop it. Harvard Business Review. February 09, 2022. https://hbr.org/2022/02/blame-culture-is-toxic-heres-how-to-stop-it Accessed July 22, 2023.
- Pickard H. Responsibility without blame for addiction. Neuroethics. 2017;10:169–180. PMID: 28725286
- Amalberti R, Hourlier S. Chapter 24: Human error reduction strategies in health care. In: Carayon P, ed. Handbook of Human Factors and Ergonomics in Health Care and Patient Safety. 2nd ed. CRC Press; 2012:385-399.
- Read GJM, Shorrock S, Walker GH, Salmon PM. State of science: evolving perspectives on ‘human error’. Ergonomics. 2021;64:1091–1114. PMID: 34243698
- Hollnagel E, Wears R, Braithwaite J. From safety I to safety -II: a white paper. 2015. https://www.england.nhs.uk/signuptosafety/wp-content/uploads/sites/16/2015/10/safety-1-safety-2-whte-papr.pdf Accessed July 22, 2023.
- Kellogg KM, Hettinger Z, Shah M, et al. Our current approach to root cause analysis: is it contributing to our failure to improve patient safety? BMJ Qual Saf. 2017;26:381–387. PMID: 27940638
- Lee JC. The opioid crisis is a wicked problem. Am J Addict. 2018;27:51. PMID: 29283484
- Wears R, Sutcliffe K. Still not safe: patient safety and the middle-managing of American medicine. Oxford University Press; 2019.
- Cohen JB, Patel SY. The successful anesthesia patient safety officer. Anesth Analg. 2021;133:816–820. PMID: 34280174
- Lambert BL, Centomani NM, Smith KM, et al. The “Seven Pillars” response to patient safety incidents: effects on medical liability processes and outcomes. Health Serv Res. 2016;51:2491–2515. PMID: 27558861
- Vinson AE, Randel G. Peer support in anesthesia: turning war stories into wellness. Curr Opin Anaesthesiol. 2018;31:382–387. PMID: 29543613
- Reason J. Safety paradoxes and safety culture. Injury Control and Safety Promotion. 2000;7:3–14. https://doi.org/10.1076/1566-0974(200003)7:1;1-V;FT003
- Marx D. Patient Safety and the “Just Culture.” 2007. https://www.unmc.edu/patient-safety/_documents/patient-safety-and-the-just-culture.pdf Accessed July 22, 2023.
- Deutsch ES, Yonash RA, Martin DE, et al. Wrong-site nerve blocks: a systematic literature review to guide principles for prevention. J Clin Anesth. 2018;46:101–111. PMID: 29505959
