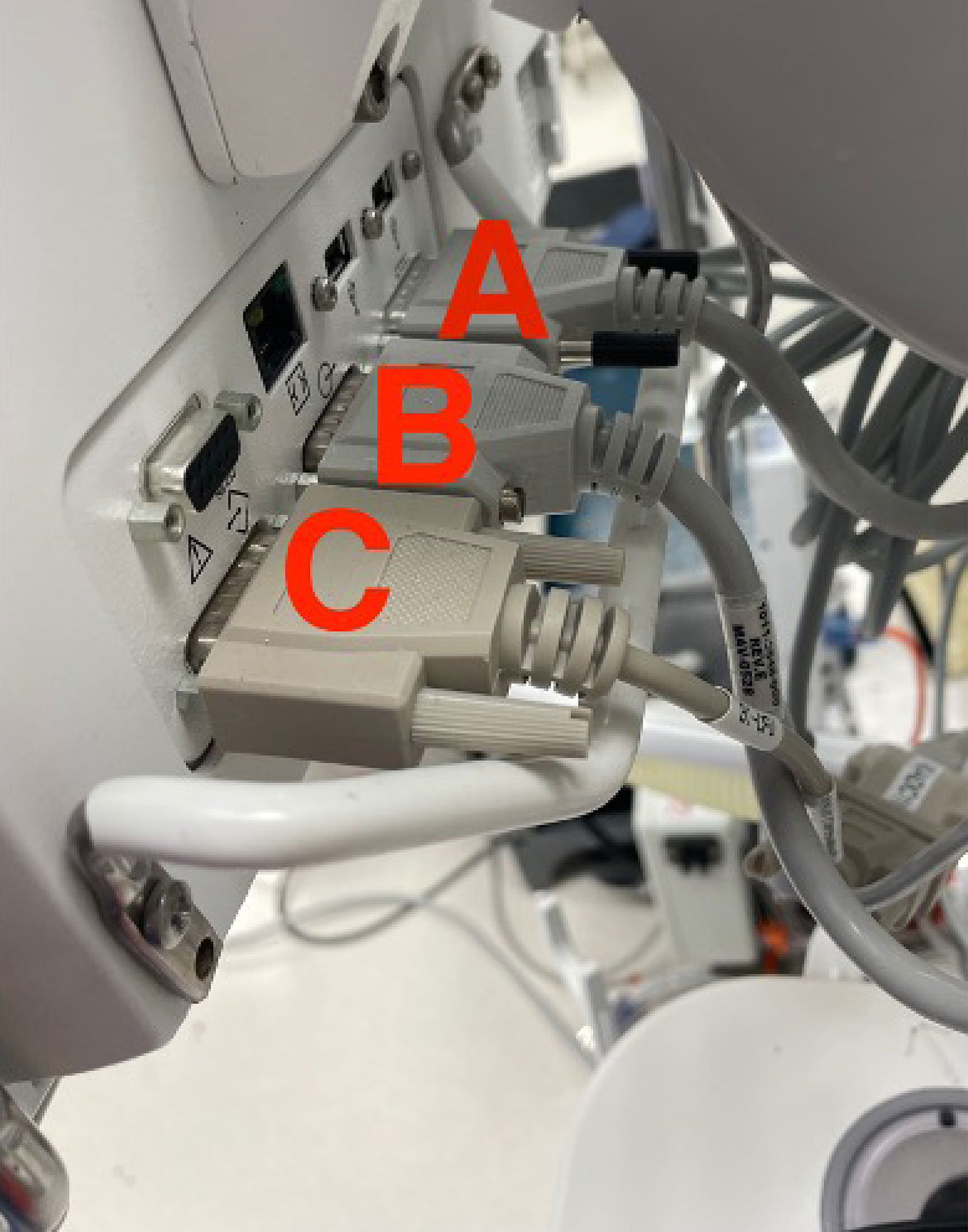
Figure 1: Cable A: System Power Interface; Cable B: System Signal Interface; Cable C: Serial Port – standard interface for external communication to electronic health record.
Intraoperative equipment failures are increasingly rare events, but may cause serious harm based on an analysis of the American Society of Anesthesiologists (ASA) Closed Claims database.1 Pre-anesthesia checkout procedures strive to make these events preventable, but certain failures cannot be prevented with a standard checklist. A task force organized under the ASA Committee on Equipment and Facilities initiated a comprehensive anesthesia apparatus checkout recommendation which we follow at our institution.2 Despite this practice, our institution recently experienced two critical malfunctions of the General Electric Aisys Anesthesia Carestation (GE Healthcare, Chicago, IL).
Both instances resulted in power loss to the anesthesia monitor display unit leading to the loss of all ventilation parameters, cessation of mechanical ventilation, and the inability to use volatile anesthetics. During both cases, the cause of the anesthesia machine malfunction was not immediately known, but both intraoperative teams eventually identified a loose connection behind the anesthesia monitor display unit (Figure 1). One case identified a missing securement screw where the System Power Interface cable (Cable A) is connected to the display unit. For the second case, the cables appeared connected, but an untightened screw was discovered upon closer examination. After firmly reinserting the Cable A into the back of the monitor, the anesthesia machine progressed through the startup cycle. The anesthesia monitor display unit then displayed a nonspecific error screen (“internal problem prevents normal operation”) and instructed the user to mechanically ventilate with the alternate O2 control and cycle power on the anesthesia machine (Figure 2). Alternate O2 control was automatically engaged shortly after the malfunction occurred, and both cases briefly utilized total intravenous anesthesia because the power failure precluded use of volatile anesthetic agents. After the machine restarted, both anesthesia teams were able to resume normal operations, and there was no patient harm.
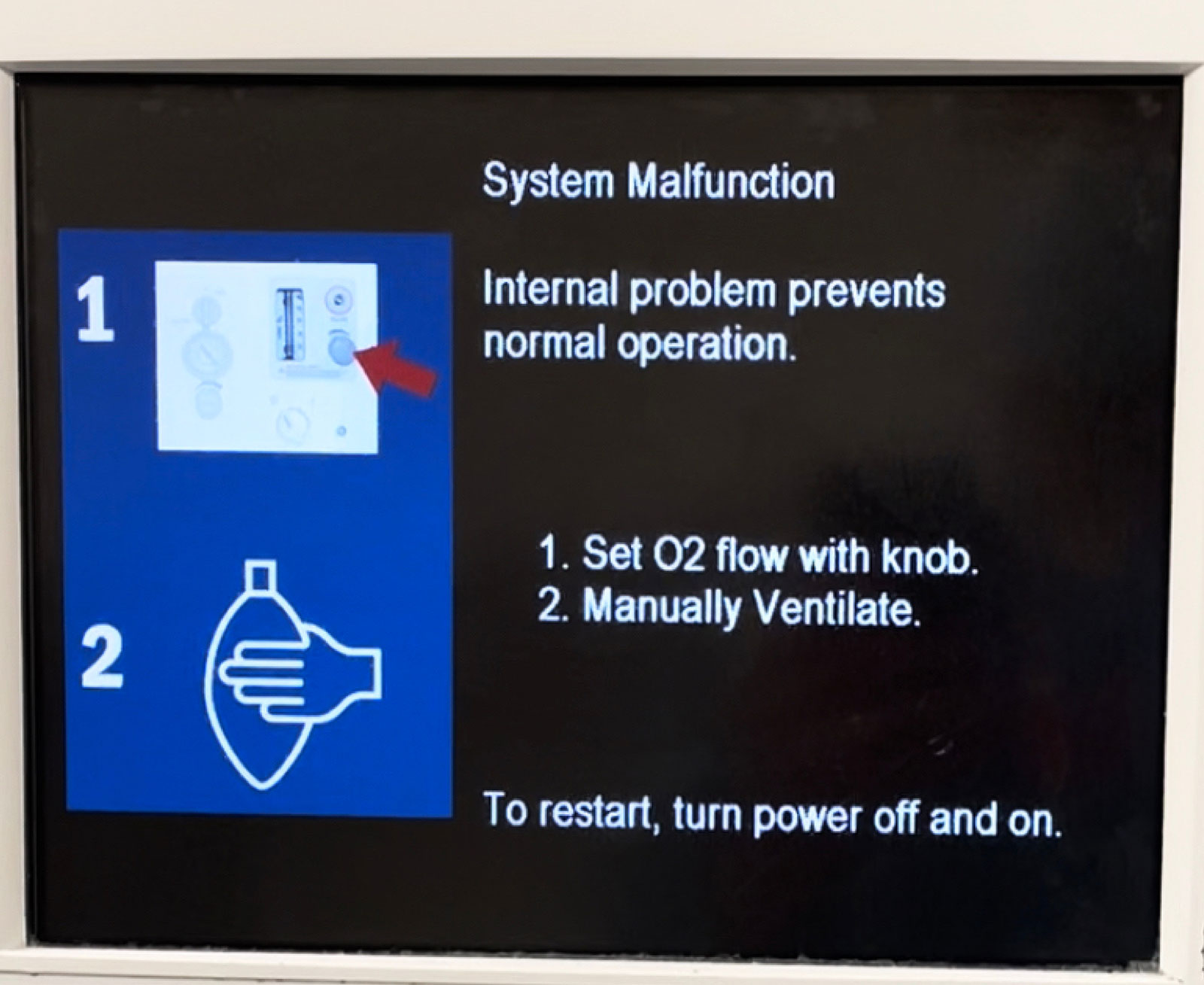
Figure 2: Error screen instructing the user to mechanically ventilate with the alternate O2 control and cycle power on the anesthesia machine
Upon review of the error history after the events, the logs noted two errors: “DU to PSC Comm Error” and “POWER CNTRL COM FAIL,” pointing to a disconnection of the communication cable between the anesthesia controller board and the anesthesia monitor display unit (Figure 3). Recreating this error with a biomedical technician demonstrated that even a slightly untightened screw can lead to a transient cable disconnection with movement of the monitor arm. The machine will not initiate the startup sequence until the communication cable is reseated firmly. A similar error has also occurred with cable “C” disconnections (Figure 1), which interrupt anesthesia machine external communication to the electronic health record.
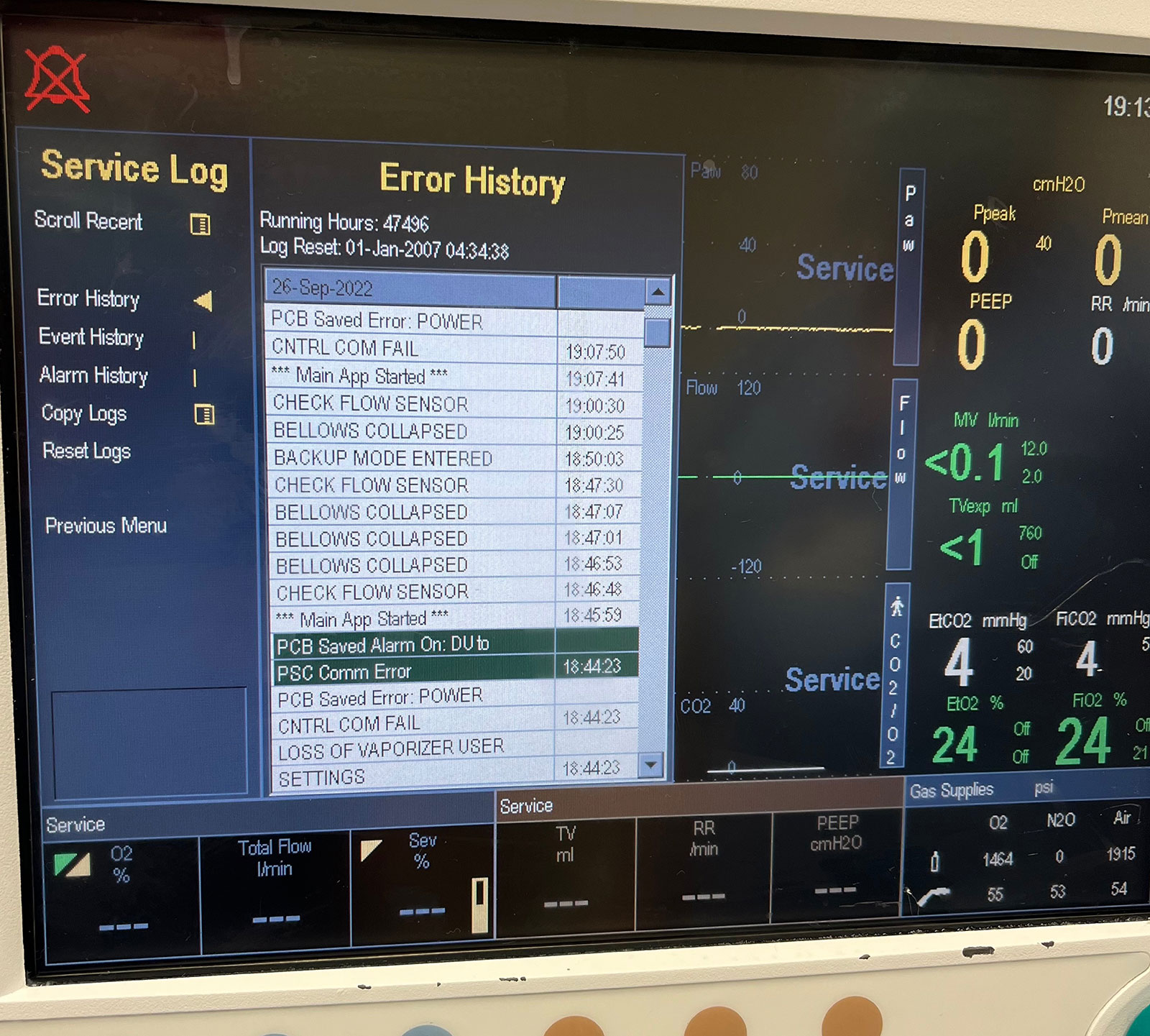
Figure 3: Error log showing “DU to PSC Comm Error” and “POWER CNTRL COM FAIL”
Our anesthesia machines are fifteen years old and nearing fleet replacement. On the 12-month preventative maintenance (PM) schedule, checking these communication cables is listed under “Visual Inspection Procedure”.3 These loose connections are also not detected by the automated machine check or standard preinduction checklists. These cases are the first occurrences of this malfunction at our institution, but we are concerned that this will happen with increasing frequency with other anesthesia machines in our fleet as the screws continue to disengage over time.
A solution to this fault would be placement of a retainment clip as a redundant securement mechanism. Redundancy to prevent failure of critical systems is a hallmark of safety innovation not only in anesthesia, but also in aviation and other industries.4-5 Improved designs can prevent errors particularly for rare problems where standard checklists may fail.6 Unfortunately, this proposal may not be feasible given the current design and the number of machines in clinical service. After fifteen years of use, older anesthesia machines are probably experiencing more screw failures along with other maintenance requirements. The General Electric Aisys Anesthesia Carestation would not meet ASA anesthesia machine obsolescence guidelines for several more years.7 We have asked our biomedical department to retighten the screws for all our anesthesia machines and suggested a more proactive PM requirement to confirm that these screws are tightened to prevent cable disconnections. Heightened vigilance about this potentially catastrophic vulnerability is necessary as these machines age.
David Corpman, MD, is a CA-3 resident in the Department of Anesthesia and Perioperative Care at UCSF Medical Center, San Francisco, CA.
Linda Liu, MD, is a professor in the Department of Anesthesia and Perioperative Care at UCSF Medical Center, San Francisco, CA.
The authors have no conflicts of interest.
REFERENCES
- Mehta SP, Eisenkraft JB, Posner KL, Domino KB. Patient injuries from anesthesia gas delivery equipment: a closed claims update. Anesthesiology. 2013;119:788–795. PMID: 23835591
- Feldman JM, Olympio MA, Martin D, Striker A. New guidelines available for pre-anesthesia checkout. APSF Newsletter. 2008;23:1. https://www.apsf.org/article/new-guidelines-available-for-pre-anesthesia-checkout/ Accessed Nov. 4, 2022.
- Aisys Anesthesia Machine Technical Reference Manual. Datex-Ohmeda. M1046983. 11/2016.
- Lawrence E. Advisory Circular: System safety analysis and assessment for part 23 airplanes. US Department of Transportation Federal Aviation Administration. November 17, 2011. https://www.faa.gov/documentLibrary/media/Advisory_Circular/AC%2023.1309-1E.pdf. Accessed Nov 4, 2022.
- National Infrastructure Advisory Council. A framework for establishing critical infrastructure resilience goals. US Department of Homeland Security. October 19, 2010. https://www.dhs.gov/xlibrary/assets/niac/niac-a-framework-for-establishing-critical-infrastructure-resilience-goals-2010-10-19.pdf. Accessed Nov 5, 2022.
- Mariyaselvam MZA, Young PJ. When checklists fail: human factors learning from aviation and safety by design. Anesthesiology. 2018;129:1192–1193. PMID: 30422860
- Dorsch J. Anesthesia machine obsolescence guidelines published. ASA Newsletter. 2004;68:27–28. https://pubs.asahq.org/monitor/article/68/9/27/1204/Anesthesia-Machine-Obsolescence-Guidelines. Accessed Nov 7, 2022.
Response
GE HealthCare would like to thank the team from University of California San Francisco School of Medicine for submitting their experience with an Aisys Anesthesia Machine display cable disconnection resulting in loss of the display and control during two procedures. In response to this report, GE HealthCare performed an extensive review of the technical description of the failure, the design of the display cable, and GE HealthCare’s servicing documentation (Technical Reference Manual).
Per the description in the report, the cable that became disconnected is the communication cable between the Display Unit and the Anesthesia Control Board. When there is a communication loss between the Display Unit CPU and the Anesthesia Control Board CPU, the system is designed to display the “System Malfunction” screen as described in the report.
The report points out that the loose cable connection is not detected by the pre-use machine checkout and/or during preventative maintenance. As this condition is a result of a communication loss between the Display Unit CPU and the Anesthesia Control Board CPU, the machine will enter the System Malfunction state if the communication loss is greater than 10 seconds regardless of the state of the machine (Power-up, Checkout, or Planned Maintenance). Therefore, if the disconnect were to have occurred, or been present, during pre-use machine checkout it would have been identified.
The Maintenance Procedures section in the Technical Reference Manual recommends a visual inspection procedure of the machine including a step to “Check all external electrical cabling. Ensure all are correctly connected and are not deteriorated.” This portion of the Maintenance Procedure is intended for the service personnel to check the condition and tightness of the external cables, including the display communication cable.
Also, the recommended maintenance for the Aisys Anesthesia Machine, as detailed in the Maintenance Procedures section, requires the 3v battery in the display CPU to be replaced every 48-months. The replacement of this battery requires the display cables to be disconnected and the display to be removed from the Aisys Anesthesia Machine. Therefore, it is likely based on the age of the machines that these display cables have been removed and reinstalled at least three times since the machine was manufactured.
GE HealthCare strives for continuous improvement and will consider the authors’ suggestions for maintenance improvements and cable retention for future designs.
www.gehealthcare.com/about/contact-us
Sincerely,
Anthony Bean
Systems Engineering Manager – Anesthesia & Respiratory Care GE HealthCare

The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or group responses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intention of APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
