Dear RAPID Response:

A 4.3kg 6-week-old patient was in the operating room (OR) for repair of a ventricular septal defect. After a minor adjustment in table height using the pendant (hand controller), our Skytron 3602 OR table continued to rise on its own until it reached its full height. The bed’s motion could be paused by continuously pressing any of the other buttons on the pendant, but only while the button remained depressed. As the bed went to full height, we ensured our lines and monitors were not under tension. The ventilator circuit only just reached the patient’s endotracheal tube. Our clinical engineering team changed out the bed control pendant, and we regained normal control of the bed. Fortunately, this event happened after the surgery was complete and the dressing on; had the bed malfunction occurred during cardiopulmonary bypass, decannulation and exsanguination could easily have resulted.
Our biomedical engineering group was familiar with the problem, diagnosing a stuck button on the pendant. Our hospital first noticed the same problem in May of 2019, when unanticipated upward movement of a Skytron bed occurred during a robotic hernia repair. Fortunately, the robot was not docked, as this would have the potential to do catastrophic damage to the patient. Since then, we have documented 4 additional incidents at our institution, 3 with Skytron 3602 and 1 with Skytron 6701 beds. The motion in each case was upward vertical motion. Two of these incidents were the subject of prior Medwatch reports to the FDA.1
We queried the U.S. Food and Drug Administration Manufacturer and User Facility Device Experience (MAUDE) database from 2015 to the present for unintended movement in Skytron OR tables. Although the level of detail in the MAUDE database is not deep, we were able to exclude some reports that pointed to different etiologies, such as sudden movement consistent with a component failure, or other electro-mechanical failures indicated by visible smoke or leaking hydraulic fluid. We also excluded bed movements that could not be achieved by a single stuck button on the hand controller. We found 4 reports that are at least suggestive of experiences similar to ours. Two were reports of unintended vertical motion, one of which bundled four separate incidents.2 The other 2 reports are of unintentional airplaning.3
Investigation by one of our biomedical engineers suggested the cause of the unintended motion was a stuck button. There is a disk-shaped piece of plastic underneath the button overlay the operator presses. This piece interfaces with the actual switch behind it. With just the right (or wrong) vector of force applied to the button, the plastic disk can jam into the switch, resulting in continuous bed movement. While difficult, it has been possible to recreate the fault in our lab.
All of the buttons on this pendant style share the same design, suggesting that any of them could trigger this kind of fault. We suspect that because the table up button is frequently used for its table lock function, that particular button may be more prone to wear, explaining why all of our cases have involved vertical motion. But the role of component wear is unclear, since the failure leading to unintended motion appears to be inherent in the pendant design. Our events have occurred with pendants that are less than 5 years old. We understand that a pendant bed control with a different underlying design is under development, but the time-line for release is unclear.
Skytron’s examination of our pendant showed evidence of fluid invasion, most likely related to overly wet cleaning cloths used during room turnovers. In addition, Skytron’s testing leads them to posit a different mechanism for the fault, one more directly related to component wear over many uses. The authors of this letter are unable to adjudicate the most likely mechanism of the unanticipated movement.
Our institution has implemented a program of training and review for our hospitality staff to ensure cleaning processes that reduce the risk of leaving the pendant wet beyond the necessary dwell time of our cleaning agents. We have also undertaken a program of education for every member of the OR team. If a Skytron OR table is moving when no button is being pressed:
- Press any other button on the bed controller to arrest the table’s motion.
- If time and clinical circumstances allow, try pressing the activated button to see if it will unstick.
- Have someone go under the OR table to press the red emergency stop button.
It is now our policy to turn off the OR table once final positioning is achieved for robotic cases. However, there are many cases, such as those with cardiopulmonary bypass, for which intermittent bed repositioning is required throughout the case, yet where large unintended changes in patient position could have catastrophic results. Turning off the bed for the duration of surgery is rarely a viable solution, nor even a broadly applicable band-aid.
Stephen Weston, MD, is associate professor in the Department of Anesthesia and Perioperative Care at the University of California, San Francisco.
Claudia Benkwitz, MD, PhD, is associate professor in the Department of Anesthesia and Perioperative Care at the University of California, San Francisco.
Richard Fechter is a clinical engineer at the University of California, San Francisco.
The authors have no conflicts of interest.
References
- Food and Drug Administration, MAUDE (Manufacturer and User Facility Device Experience) Database. Reports 8619119 and 9409491. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/search.cfm Accessed June 4, 2020.
- Food and Drug Administration, Manufacturer and User Facility Device Experience Database. Reports 8752471, 8939952. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/search.cfm Accessed June 4, 2020.
- Food and Drug Administration, Manufacturer and User Facility Device Experience Database. Reports 9340635, 6081727. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/search.cfm Accessed June 4, 2020.
Reply:
This letter follows up a comprehensive investigation and review by Skytron and its manufacturer, Mizuho, of reported UCSF pendant control concerns regarding inadvertent table movement, and responds to your request for information dated September 14, 2020. Skytron and Mizuho have concluded their investigation of the UCSF pendant controls, which included extensive physical examination and testing of the UCSF controls. As discussed in a meeting with the UCSF team on Friday, September 4, 2020, the returned UCSF pendant controls exhibited a high degree of atypical use and uncommonly displayed both external and internal damage, along with resulting loss of functionality. Specifically, the damage and observed loss of functionality in the 22 UCSF returned units included:
- 20 Units with fluid ingress
- 10 Units with corrosion related to fluid ingress
- 5 Units backlight failure
- 22 Units physical damage to cover
- 2 Units inconsistent or failed battery on/off function
- 1 Unit continuous table up movement
- 9 Units with damage to button face
Thus, over 90% of the UCSF units revealed internal evidence of fluid ingress to the electronic components (consistent with dipping of the controls and/or other improper cleaning techniques), and 50% of the units exhibited corrosion to the circuit boards and/or wiring. One control with fluid ingress and external damage was also found to have internal physical damage to the button resulting in a continuous table up movement. Skytron has concluded that the reported issues with the UCSF controls were caused by a combination of fluid ingress and atypical use and force applied to the pendants.
The use and maintenance of the pendant controls contributed to the malfunction experienced by UCSF. Skytron understands and appreciates the challenges of the clinical environment and strives to ensure that its products are sufficiently robust to meet such challenges. With respect to maintenance of pendants, however, Skytron’s manual and cleaning instructions are clear. Skytron specifically cautions against immersing pendant controls in liquids and allowing fluid entry into electrical connectors:
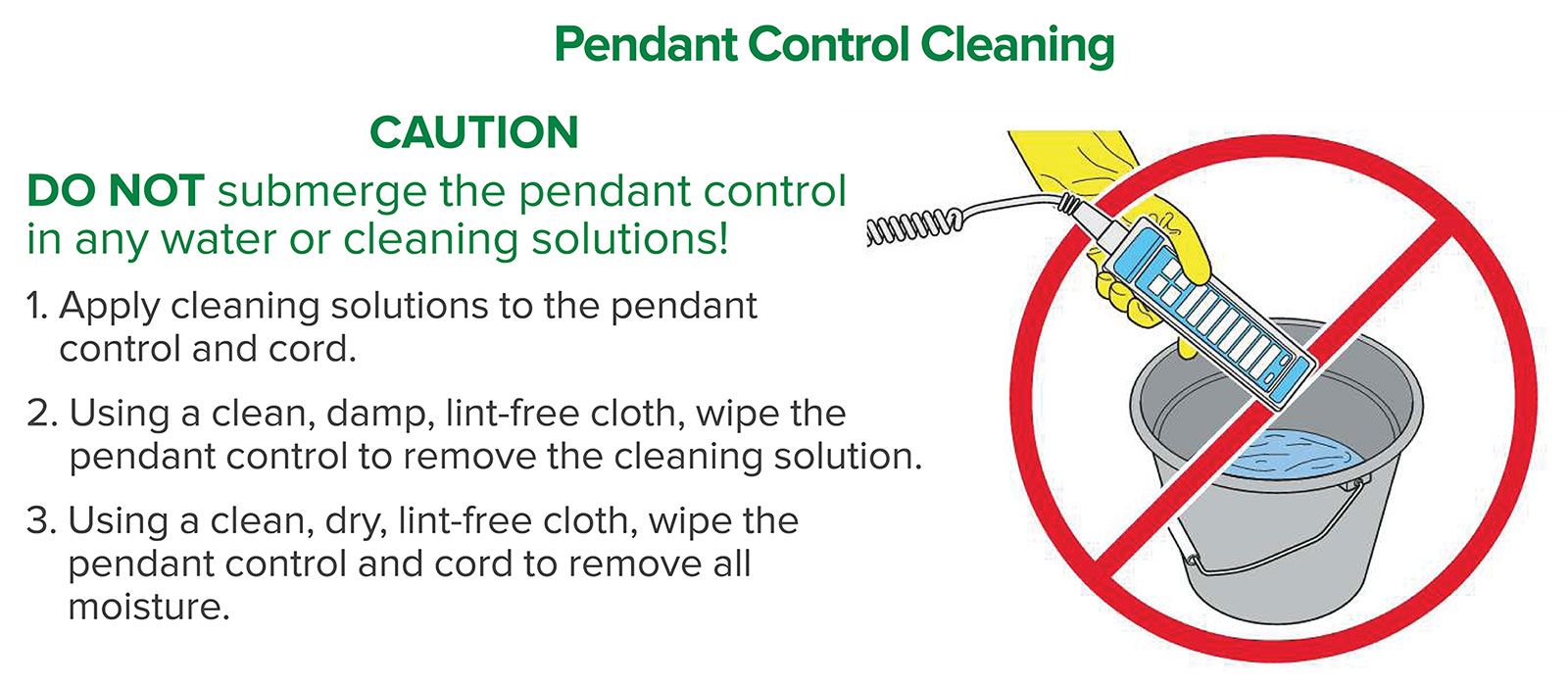
Figure 1: Pendant Control Cleaning.
When properly maintained, the pendant controls are sufficiently robust and operate safely and reliably. To be sure, as part of the investigation, Skytron and its manufacturer examined the entire history of complaint data and MDR reports for the pendants across all user facilities, taking into consideration the frequency of occurrence and the number of tables in distribution. The data demonstrated an extremely low complaint rate, and do not indicate a failure of the device design or suggested maintenance procedures.
The experience of the UCSF team, however, is being considered as we develop future product design enhancements and continuing education of our customers regarding proper maintenance of the pendants. Skytron’s focus remains on understanding and meeting the specific needs of our users as we develop products that ensure patient safety and customer satisfaction.
Skytron continues to work with UCSF to meet its user needs and ensure product satisfaction, including reinforcement of proper maintenance, cleaning, and inspection protocols.
Please call or email me if you have any further questions.
Sincerely,
Erin Woolf
Quality Manager, Skytron
The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or group responses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intention of APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
