Prescription opioids have played a considerable role in the national opioid epidemic. Specifically, examination of perioperative opioid prescribing suggests a fair degree of both indiscretion and overprescribing. Preoperative use of opioids has been associated with increased perioperative morbidity and mortality as well as a risk for postoperative abuse. Additionally, opioids remaining following surgery are at risk for accidental ingestion or abuse in children and adults respectively. Anesthesia professionals have a unique opportunity to screen patients at risk for abuse or misuse as well as educate patients on safe opioid storage and disposal.
Introduction
 Health care professional-prescribed opioids have played a significant role in the growing opioid epidemic. In 2017, more than 70,000 drug-related deaths occurred in the United States with over 47,000 a result of opioids.1 Opioid-related deaths have surpassed deaths related to breast cancer, gun violence, and automotive accidents (Table 1). According to the National Institutes of Health, the yearly estimated cost of the opioid epidemic exceeds $78.5 billion including the costs of health care, lost productivity, addiction treatment, and criminal justice-related expenses.1
Health care professional-prescribed opioids have played a significant role in the growing opioid epidemic. In 2017, more than 70,000 drug-related deaths occurred in the United States with over 47,000 a result of opioids.1 Opioid-related deaths have surpassed deaths related to breast cancer, gun violence, and automotive accidents (Table 1). According to the National Institutes of Health, the yearly estimated cost of the opioid epidemic exceeds $78.5 billion including the costs of health care, lost productivity, addiction treatment, and criminal justice-related expenses.1
Table 1: Comparison of Death Rates Amongst Common Causes in the United States
| Cause of Death (year) | Death per reported year | Deaths per day |
| Opioids (2017) | 47,6001 | 130 |
| Breast Cancer (2016) | 41,487* | 113 |
| Firearms (2017) | 39,773† | 109 |
| Automotive Accidents (2018) | 36,560‡ | 100 |
*CDC data 2016: https://gis.cdc.gov/Cancer/USCS/DataViz.html
†NHTSA: https://www.nhtsa.gov/traffic-deaths-2018
‡CDC: https://www.cdc.gov/nchs/fastats/injury.htm
A significant driver of the opioid addiction issues relates to medically prescribed opioids. Specifically, examination of perioperative opioid prescribing suggests a fair degree of both indiscretion and overprescribing. One study suggests that as many as 80% of opioid-naïve adult patients filled a prescription for opioids following low-postoperative-pain-risk surgical procedures (e.g., carpal tunnel release, laparoscopic cholecystectomy, inguinal hernia repair, or knee arthroscopy).2 Additionally, between 2004–2008, the mean number of doses prescribed increased following these low-risk procedures.2 A study of 88,637 opioid-naïve adolescents and young adults ages 13–21 years undergoing surgery revealed that 4.8% continued to fill prescriptions for opioids 90 days following low-risk surgery.3
Health care Professionals and the Unintended Consequences of Opioid Prescriptions
Opioids prescribed by health care professionals have resulted in a significant number of opioid-related toxicity cases in children.4 From 2000–2015, there were 188,468 cases of opioid-related exposures reported to the National Poison Data System in persons < 20 years of age.4 Children most at risk were those between ages 0–5 years and adolescents ages 12–17 years with small children at risk of accidental exposures and adolescents at risk of deliberate ingestion.4 Pediatric opioid related exposures have resulted in > 3600 pediatric critical care unit admissions between 2004–2015.5
Unused opioids following surgery endanger adult and pediatric patients by allowing for nontherapeutic use as well as accidental ingestion. A meta-analysis of studies reviewing postsurgical opioid prescriptions suggested that 42–71% of opioid tablets went unused.6 The vast majority of these unused opioids are often stored in the home unsecured and serve as a source for abuse and misuse.6
A study of adults undergoing orthopedic surgical procedures suggested that the preoperative use of opioids is associated with an increase in the following perioperative complications: respiratory failure, surgical site infections, need for mechanical ventilation, pneumonia, myocardial infarction, postoperative ileus or other gastrointestinal events, and an increase in all-cause mortality.7 Additionally, preprocedural long-term opioid use by a family member has been associated with persistent opioid use in opioid-näive adolescents and young adults following surgical and dental procedures for which opioids are prescribed.8 While it is unclear as to who is consuming these opioids (patient vs. family member), it suggests that physicians should be screening patients prior to prescribing opioids to potentially mitigate the long-term use of them by either group.
Health care professionals may have a unique opportunity during the perioperative period to address critical issues pertaining to opioid stewardship (Table 2). Anesthesia professionals typically screen patients for recent illness, smoking, and illicit drug use. During the perioperative period, they may also be able to ascertain the opioid risk by inquiring about the patient’s personal opioid history as well as those in the patient’s home that may be at risk for abuse or misuse. Additionally, the anesthesia encounter provides the opportunity to educate patients on the dangers of opioids and the requirement for proper storage and disposal.
Table 2: Perioperative suggestions to enhance opioid safety and perform risk assessment
|
|
|
|
|
Our Own Experience in Combating the Opioid Crisis
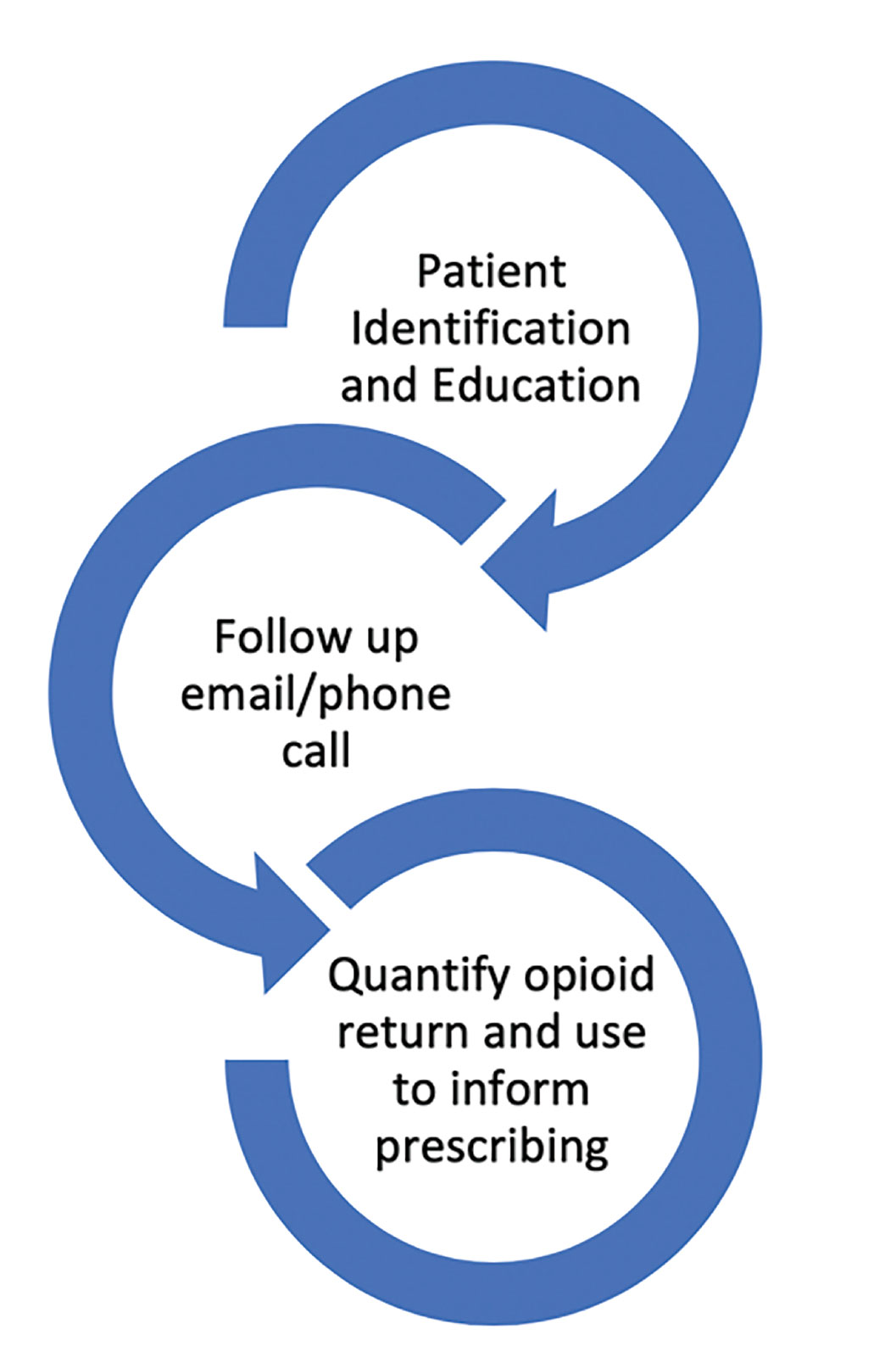
Figure 1: Process of opioid stewardship from education to retrieval.
At our institution, we recently completed an initiative to combat the opioid crisis by combining patient and family education with a simple method for families to dispose of their unused medication.9 This project involved providing a pre-addressed and postage-paid envelope for patients to return their unused opioids, followed by an automated reminder email two weeks postoperatively. This was combined with patient and parental education on safe storage and disposal. This pilot had 64 of 331 participants return unused opioids with a total of nearly 3000 mg of oral morphine equivalents removed from these homes (Figure 1). For those that returned opioids, the median rate of return was 58% (interquartile range = 34.7%–86.1%) of the amount prescribed. Demographic variables associated with increased likelihood for return of medication were Caucasian, married, and holding a postgraduate degree. At present we are working with our pharmacy team to enroll all perioperative patients receiving opioids at discharge in this project with hopes to understand pediatric prescribing on a larger scale.
Conclusion
Efforts have been taken to reduce the prescribing of opioids while tracking prescriptions through implementation of individual state prescription monitoring programs. Anesthesia professionals are uniquely positioned to address opioid-related safety issues during the perioperative period. We may be able to reduce patient exposure by identifying patients at risk, educating patients and families on safe opioid storage, and disposal and advocating for appropriate dosing.
References
- Scholl L, Seth P, Kariisa M, et al. Drug and opioid-involved overdose deaths – United States, 2013–2017. MMWR. 2018;67:1419–1427.
- Wunsch H, Wijeysundera DN, Passarella MA, Neuman MD. Opioids prescribed after low-risk surgical procedures in the United States, 2004-2012. JAMA. 2016;315:1654–1657.
- Harbaugh CM, Lee JS, Hu HM, et al. Persistent opioid use among pediatric patients after surgery. Pediatrics. 2018;141:e20172439
- Allen JD, Casavant MJ, Spiller HA, et al. Prescription opioid exposures among children and adolescents in the United States: 2000–2015. Pediatrics. 2017;139 :e20163382.
- Kane JM, Colvin JD, Bartlett AH, Hall M. Opioid-related critical care resource use in US children’s hospitals. Pediatrics. 2018;141:e20173335
- Bicket MC, Long JJ, Pronovost PJ, et al. Prescription opioid analgesics commonly unused after surgery: a systematic review. JAMA Surgery. 2017;152:1066–71.
- Menendez ME, Ring D, Bateman BT. Preoperative opioid misuse is associated with increased morbidity and mortality after elective orthopaedic surgery. Clin Orthop Relat Res. 2015;473:2402-12.
- Harbaugh CM, Lee JS, Chua KP, et al. Association between long-term opioid use in family members and persistent opioid use after surgery among adolescents and young adults. JAMA Surgery. 2019;154:e185838.
- Adler AC, Yamani AN, Sutton CD, et al. Mail-back envelopes for retrieval of opioids after pediatric surgery. Pediatrics. 2020;145:e20192449
