 Anesthesia professionals are encountering patients with non-cardiac implantable electrical devices (NCIED) with increasing frequency. These devices are otherwise known as neurologic stimulators and include, but are not limited to spinal cord stimulators (SCS), deep brain stimulators (DBS), and vagal nerve stimulators (VNS). The indications for placement of NCIEDs are expanding and as such the likelihood that an anesthesia professional will encounter them during elective and emergent surgical procedures is increasing.
Anesthesia professionals are encountering patients with non-cardiac implantable electrical devices (NCIED) with increasing frequency. These devices are otherwise known as neurologic stimulators and include, but are not limited to spinal cord stimulators (SCS), deep brain stimulators (DBS), and vagal nerve stimulators (VNS). The indications for placement of NCIEDs are expanding and as such the likelihood that an anesthesia professional will encounter them during elective and emergent surgical procedures is increasing.
TYPES OF NCIEDS
Vagal Nerve Stimulators (VNS):
VNS are pulse generators placed in the mid-cervical neck, usually on the left. The left is typically chosen to avoid severe bradycardia that can occur with the right-sided vagal nerve stimulation. Indications for VNS include seizure reduction, cluster headache prevention, and refractory depression.
Deep Brain Stimulator (DBS):
DBS is an implanted lead used to stimulate structures deep within the brain. The most common targets include the thalamus, globus palladium, and subthalamic nuclei. The target for the lead is dependent on the pathology being treated. It is considered to be a minimally invasive targeted neurosurgical intervention. Since its success with Parkinson’s disease, its utilization has expanded to other movement disorders (tremors, tics, and dystonias), psychiatric illnesses (major depression and obsessive-compulsive disorder), chronic pain, and refractory epilepsy.
Spinal Cord Stimulators (SCS):
SCS inhibit chronic pain by continuously stimulating the large diameter afferent fibers in the spinal cord. The electrode itself lies in the dorsal epidural space, and its location is determined by the location of the pain being treated.
In general, low thoracic to lumbar placement is used to manage lower extremity pain and chronic low back pain and mid-cervical to high thoracic placement is used to manage upper extremity pain.
There are additional NCIEDs as well, such as the hypoglossal nerve stimulator, phrenic nerve stimulators, sacral nerve stimulators, and gastric nerve stimulators. The hypoglossal nerve stimulator, for example, helps treat obstructive sleep apnea (OSA). Obesity and OSA are on the rise and patients are growing less tolerant of traditional treatments such as continuous positive airway pressure (CPAP). This has given way to the increased utilization of the hypoglossal nerve stimulator for the treatment of OSA. Hypoglossal nerve stimulators treat OSA by sending electrical pulses to the hypoglossal nerve, controlling tongue movement and causing the tongue to move forward during sleep, thereby reducing airway collapse and possible obstruction.
PREOPERATIVE CONSIDERATIONS
In order to provide safe anesthetic care and prevent day of service delays, patients with NCIEDs should undergo a preoperative evaluation such as in the anesthesia preoperative clinic prior to elective cases. This will help identify patients with NCIEDs in advance, allow time to contact the providers managing their devices, and inform those providing anesthetic care for these patients (Figure 1).
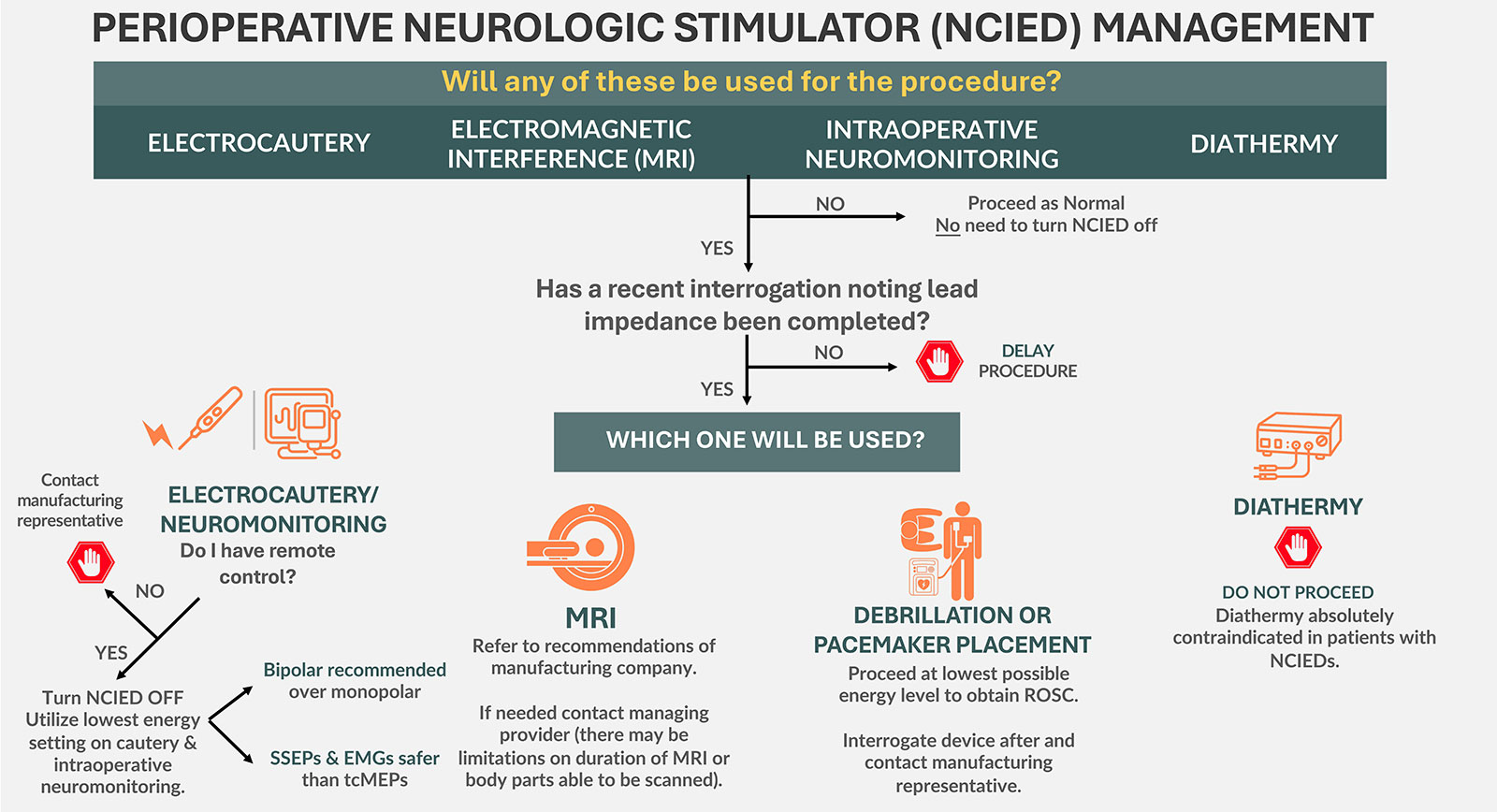
Figure 1: Potential intraoperative device interactions when patients present with NCIEDs.
NCIED: Non-cardiac implantable electrical device; MRI: Magnetic Resonance Imaging; SSEP: Somatosensory Evoked Potential; EMG: Electromyography; tcMEPs: Transcortical Motor Evoked Potential; ROSC: Return of Spontaneous Ventilation
Prior to anesthetizing a patient with an NCIED, there are several questions that should be asked of the patient and/or the provider managing their device (Table 1).1,2
Table 1: General Perioperative Concerns for Patients with NCIEDs2
| Identify the type of device, the manufacturer, and model. Does the patient have a device identification card? |
| Where are the leads and pulse generator located? |
| How is the device turned off or inactivated? Does the patient have a remote or magnet? |
| What symptoms develop when the device is turned off? |
| When was the device implanted? What is the battery status? |
| When was the last device check/interrogation? |
| What was the lead impedance on the last device check? |
| Determine availability of “safe modes” for surgery or for MRI. |
| The provider who placed the device should be contacted for perioperative device recommendations (as part of preoperative clinic assessment). |
| Does the surgery/procedure require neuromonitoring? If so, discuss with the provider who placed the device as certain neuromonitoring modalities may be deemed unsafe (preop. clinic provider). |
| Contact the device representative to determine if they need to be present on the day of surgery for pre/postoperative interrogation (preop. clinic provider). |
| Does the patient also have any additional implanted devices? If so, the providers managing both devices should be contacted for recommendations. |
It is imperative to request a recent interrogation of the device from the managing provider noting the lead impedance, as this is used to assess the electrical performance and structural integrity of the leads in the NCIED and should changes be seen in the lead impedance, the procedure may potentially need to be delayed.
In addition, the surgeon performing the procedure should be made aware the patient has an NCIED. A preoperative discussion should include special surgical needs that will be utilized the day of surgery (i.e., neuromonitoring or electrocautery) and determine whether those needs will interact with the device. During the preoperative evaluation regarding the device, it is imperative to determine if the device should be reprogrammed to a specific setting (i.e., MRI safe mode or surgery safe mode) or turned off.
DAY OF SURGERY
Prior to case start, all individuals involved in the care of a patient with a NCIED should be aware that the patient has the device; this includes preoperative, operative, and postoperative care teams. Two commonly used intraoperative tools that can interact with NCIEDs are electrocautery and intraoperative neuromonitoring.
ELECTROCAUTERY
Electrocautery induces an electrical current within the body, and patients with NCIEDs undergoing surgery with electrocautery are at risk for harm. These risks can be mild, such as potentially reprogramming the device and changes in stimulator output. However, there is also the possibility of significant harm including thermal skin burns, damage to the electrode, failure of the generator, or thermal injury to the underlying neurologic tissue. Due to these greater risks, manufacturers of most NCIEDs recommend avoiding the use of electrocautery.3-5 If electrocautery is necessary, the recommendations by most manufacturers is to first confirm the device’s lead impedance with a recent interrogation and then turn the device off. If the device has a current output setting, then this should be set to the lowest setting possible or to zero prior to turning off the device. Some devices have a surgery mode available which can be another safe option.6
For many NCIEDs, a remote is used to adjust the settings. For both SCS and DBS, the remote can be utilized to turn the device off by holding it over the generator. However, VNS systems are unique in that many patients will carry their remote in the form of a wand or bracelet. Holding the remote over the generator for a specified period, usually 2–3 seconds of time generates an impulse rather than shutting the device off. How the VNS turns off varies depending on the manufacturer. Therefore, it is important to verify that the device is turned off, which can be visualized on the controller screen. Regardless of the NCIED, care must be taken to be sure the device is off or reprogrammed to the proper setting. If there is a question regarding the NCIED settings, the device representative should be contacted.4
When using electrocautery in patients with an NCIED, bipolar cautery is preferred to unipolar/monopolar cautery. With monopolar cautery, the current travels between the device tip and the return plate or grounding pad on the patient. Therefore, the risk of current traveling through the NCIED is higher. With bipolar cautery, the majority of the current travels between the tips of the bipolar cautery and is less likely to affect the NCIED. If monopolar cautery is necessary, the surgeon should utilize the lowest power setting possible. The grounding pad should be placed so that the current is least likely to travel through the NCIED and its generator, such as the contralateral distal limb. Full-length table grounding pads should be avoided. Patients should be made aware of the need to use electrocautery as part of the surgical procedure and the subsequent risks which include potential thermal injury to brain or nervous system tissue, reprogramming of the device, and potential damage to the leads.7,8
Despite these warnings, many published reports testify to the generally safe use of both monopolar and bipolar electrocautery. A survey of 167 pediatric spinal surgeons reported no complications due to the intraoperative use of electrocautery.9 Most respondents reported short-term use of monopolar cautery. After a procedure involving the use of electrocautery, the provider should always confirm that the NCIED is on and functioning properly.5,10,11
INTRAOPERATIVE NEUROMONITORING
Many functional neurosurgeons recommend against the use of transcortical motor-evoked potentials (tcMEPs) in patients with NCIEDs. Intraoperative neuromonitoring transmits an electrical current through the patient’s body. In theory, this can also be conducted along the path of the NCIED and may damage the device or cause tissue injury along the length of the leads. TcMEPs utilize a higher energy system than somatosensory-evoked potentials (SSEPs) and for this reason SSEPs are considered to be relatively safe and well-tolerated in patients with these implanted devices.
In practice, there are several case reports that describe the use of intraoperative neuromonitoring in patients with spinal cord stimulators with no postoperative complications.9,12 However, for many neurosurgeons, the potential risks of utilizing tcMEPs in patients with vagal nerve stimulators or deep brain stimulators is not worth the benefits they may provide. If intraoperative neuromonitoring is to be employed, the lowest energy level possible should be used to obtain signals regardless of the device and type of monitoring utilized.
DEFIBRILLATION/CARDIOVERSION
The presence of a NCIED should not impede emergent cardioversion or defibrillation. The patient with a NCIED should be cardioverted or defibrillated in the setting of a cardiac emergency per advanced cardiac life support guidelines. However, clinicians should place pads as far from the device as possible and use the lowest energy that is feasible to treat the arrhythmia. The NCIED should be interrogated afterward to evaluate function.10,13,14
MRI CONSIDERATIONS WHEN AN NCIED IS PRESENT
MRIs pose a potential risk of harm to the patient or damage to the device if proper precautions are not taken. It is necessary to confirm the manufacturer and the exact model of the NCIED prior to the MRI. The provider responsible for the device should also be contacted before the MRI to discuss any safety concerns. The device manual or the manufacturer’s technical helpline should be consulted if there is any uncertainty regarding the specific scan requirements for the patient’s system. Many newer devices are MRI conditional, meaning only part of the patient’s body can now be scanned, such as the limbs, or they can only undergo scans for a specified period of time and then require a rest period. This varies from device to device and many older models are not MRI-conditional. It is imperative to confirm the specific MR-conditional components and location of the system to determine if the MRI can be safely completed.15,16 In addition, prior to the MRI, lead impedance should be checked. If it is discovered that the lead impedance is outside of the acceptable range per the manufacturer’s guidelines, the MRI should not be completed.
Some devices have an MRI safe mode. This setting will turn off stimulation and detection, but allow other background processes to continue to function. The NCIED should be set to MRI safe mode prior to the patient entering the scanner and programmed back to the original settings once the MRI is completed and the patient is safely outside of the scanner. The device should be interrogated at some point after the MRI. The timing of the interrogation should be determined by the provider or the device representative.
REGIONAL AND NEURAXIAL APPROACHES WHEN AN NCIED IS PRESENT
Regional and neuraxial anesthesia can pose challenges in patients with NCIEDs (Table 2). Any upper extremity block in a patient with a DBS or cranial nerve stimulator/NCIED should be performed under direct visualization. Using either ultrasound or fluoroscopy, the provider needs to confirm that the needle does not come into contact or transect the NCIED wires. In addition, the use of peripheral nerve stimulation to identify the location of the brachial plexus should be avoided. If the stimulation needle comes into contact with any portion of the NCIED an electrical current can be conducted, which can travel to the implanted electrode and/or pulse generator. This, like electrocautery, has the potential to damage the NCIED. There are case reports that describe the use of upper extremity block placement with peripheral nerve simulation in patients with DBS without complications.1,17,18 However, with the widespread use of ultrasound for peripheral nerve blocks, the need to perform blind peripheral nerve stimulation guided nerve blocks is unnecessary and should be avoided in patients with NCIEDs.
Table 2: Key Points When Performing an Acute Pain Procedure in a Patient with a Non-cardiac Implantable Electrical Device (NCIED)
| REGIONAL: |
|
| SPINAL: |
|
| EPIDURAL: |
|
There is an increasing number of pregnant women with SCS. Several case reports exist of the successful use of both epidurals and spinals in patients with SCS.19 However, the decision to perform neuraxial anesthesia in patients with these devices should only be made after proper review of imaging identifying the location of the leads, level of insertion, extension wires, and the internal pulse generator. The physician managing the device should also be notified as they may have additional guidance to offer considering SCS reside in the dorsal epidural space.19-21
It is imperative that the neuraxial placement occur below the level of the SCS insertion, to avoid transecting the SCS. Appropriate emphasis should be placed on sterility during neuraxial placement to avoid infection as this can result in future SCS removal. In addition, the feel of loss of resistance may be altered if the SCS electrodes are near the entry level for the epidural. Due to the development of fibrosis from the SCS, the epidural spread of local anesthetic may be impeded and result in patchy analgesia or a failed block. Moreover, fibrosis can also result in the epidural catheter being directed caudally rather than cranially or coiling locally in the epidural space, which can cause compression of the cauda equina and lumbar roots.19,21
ECT WHEN AN NCIED IS PRESENT
Electroconvulsive therapy (ECT) is a procedure used to treat certain psychiatric conditions including refractory depression, bipolar disorder, and catatonia. While under general anesthesia, an electrical current is applied to the brain, inducing a seizure. As aforementioned, electrical currents have the potential to cause harm to the patient or damage to the device. With ECT, there is a particular concern for patients with a DBS. While there are no existing guidelines on how to manage patients with NCIEDs who are scheduled for ECT, there are many case reports demonstrating the safe use of ECT in this patient population.22 It is imperative to inform the provider managing the NCIED that the patient is being evaluated for ECT. The provider will be able to comment on the safety of proceeding with the ECT and share recommendations regarding the device prior to the ECT. Most recommendations would include reprogramming the NCIED to the lowest possible stimulation setting and then turning off the device prior to the ECT. The NCIED should be turned on immediately after the ECT, particularly DBS. Allowing only temporary interruption of the DBS for the procedure minimizes the symptoms being treated by the DBS and thus the negative impact of turning the device off. The team managing the device will decide when the NCIED should be interrogated or if any imaging is required during the course of ECT. In patients with a DBS, it is important to consider ECT electrode placement. Ideally, the electrodes would be positioned so that the ECT stimulus current path would be directed away from the DBS electrodes.23 While there are no reports of adverse outcomes in patients with NCIEDs who underwent ECT, these patients should still be approached with caution as there is no evidence-based safety guidelines for this patient population.
POSTOPERATIVE CONSIDERATIONS
Prior to emergence, if the NCIED was turned off, it should be turned back on. This will prevent disease symptoms from complicating emergence and extubation. If a representative was needed to reprogram the NCIED, that person should be present for emergence and recovery. The skin around the NCIED and its generator should be examined for any thermal injuries and the patient should be evaluated for any neurologic changes.
CONCLUSION
The number of patients presenting with NCIEDs is increasing. The article is meant to be used as a tool in the management of these patients in the perioperative period. As these devices are constantly being improved and updated, good communication with the managing provider or manufacturing representative is paramount.
Jacqueline M. Morano, MD, FASA, is assistant professor of anesthesiology at the North-western University Feinberg School of Medicine, Chicago, IL.
Jamie L. Uejima, MD, is assistant professor of anesthesiology at the Northwestern University Feinberg School of Medicine, Chicago, IL.
The authors have no conflicts of interest.
REFERENCES
- Venkatraghavan L, Chinnapa V, Peng P, Brull R. Non-cardiac implantable electrical devices: brief review and implications for anesthesiologists. Can J Anaesth. 2009;56:320–326. PMID: 19296193.
- Morano JM, Uejima JL, Tung A, Rosenow JM. Management strategies for patients with neurologic stimulators during nonneurologic surgery: an update and review. Curr Opin Anaesthesiol. 2023;36:461–467. PMID: 37552004.
- Boston Scientific. Vercise DBS physician manual. www.bostonscientific.com/content/dam/elabeling/nm/91098825-11A_Vercise_Physician_Manual_OUS_ML_s.pdf. Accessed February 2023.
- VNS Therapy. VNS therapy magnet. Updated March 3 2023. https://www.livanova.com/epilepsy-vnstherapy/en-us/magnets. Accessed March 2023.
- Medtronic. Intellis platform spinal cord stimulation for the healthcare professional. https://www.medtronic.com/us-en/healthcare-professionals/products/neurological/spinal-cord-stimulation-systems/intellis-platform.html. Accessed February 2023.
- Voutsalath MA, Bichakjian CK, Pelosi F, et al. Electrosurgery and implantable electronic devices: review and implications for office-based procedures. Dermatol Surg. 2011;37:889-–899. PMID: 21585593.
- Seemann M, Zech N, Lange M, et al. [Anesthesiological aspects of deep brain stimulation : special features of implementation and dealing with brain pacemaker carriers.] Anaesthesist. 2013;62:549–556. Anasthesiologische Aspekte der tiefen Hirnstimulation : Besonderheiten bei der Anlage und im Umgang mit Hirnschrittmachertragern. PMID: 23817843.
- Cordero I. Electrosurgical units—how they work and how to use them safely. Community Eye Health. 2015;28:15–16. PMID: 26435589.
- McMahon R, Morgan SJ, Brooks JT, et al. Does the presence of programmable implanted devices in patients with early onset scoliosis alter typical operative and postoperative practices? A survey of spine surgeons. Spine Deform. 2022;10:951–964. PMID: 35143030.
- Bull C, Baranidharan G. Spinal cord stimulators and implications for anaesthesia. BJA Educ. 2020;20:182–183. PMID: 33456948.
- Medtronic. Neuromodulation Technical Services US. Neuromodulation standard letter. Deep brain stimulation (DBS) systems.) Systems. https://health.ucdavis.edu/neurology/deep-brain-stimulation/content/Medtronic-Letter.pdf. Accessed February 2023.
- Srisooksai G, Mohamed BA, Martin PA, et al. Transcranial motor evoked potential monitoring in a patient with a deep brain stimulator: a case report. J Clin Neurophysiol. 2021;38:e1–e4. PMID: 32501949.
- Wittstock M, Buchmann J, Walter U, Rösche J. Vagus nerve stimulation and external defibrillation during resuscitation; a letter to editor. Emerg (Tehran). 2018;6(1):e27. PMID: 30009229.
- Sobstyl M, Michalowska M, Fiszer U, Zabek M. Deep brain stimulation failure due to external cardioversion in a patient with Parkinson’s disease. Neurol Neurochir Pol. 2017;51:324–330. PMID: 28587730.
- Abbott Medical MR conditional brain stimulation system clinician’s manual. https://www.neuromodulation.abbott/us/en/healthcare-professionals/mri-support/mri-dbs-full-systems.html. Accessed February 2023.
- Medtronic. Deep brain stimulation: MRI access. https://www.medtronic.com/us-en/healthcare-professionals/therapies-procedures/neurological/deep-brain-stimulation/mri-information.html. Accessed February 2023.
- Gandhi R, Chawla R. Anaesthetic management of shoulder arthroscopic repair in Parkinson’s disease with deep brain stimulator. Indian J Anaesth. 2014;58:309–311. PMID: 25024475.
- Minville V, Chassery C, Benhaoua A, et al. Nerve stimulator-guided brachial plexus block in a patient with severe Parkinson’s disease and bilateral deep brain stimulators. Anesth Analg. 2006;10:1296. PMID: 16551956.
- Patel S, Das S, Stedman RB. Urgent cesarean section in a patient with a spinal cord stimulator: implications for surgery and anesthesia. Ochsner J. 2014;14:131–134. PMID: 24688346.
- Medtronic. Getting an MRI when you have an implanted spinal cord stimulation device. Updated April 2022. https://www.medtronic.com/us-en/patients/treatments-therapies/spinal-cord-stimulation-chronic-pain/life-with-scs/getting-mri.html. Accessed February 2023.
- Kett A, Gentile ND, Kocur M. Successful administrations of neuraxial anesthesia intrapartum in a pregnant patient with an implanted thoraco-lumbar spinal cord stimulator: a case report. Gynecol Obstet Case Rep Vol 6 No. 4:24. August 27, 2020. https://www.primescholars.com/articles/successful-administrations-of-neuraxialanesthesia-intrapartum-in-a-pregnant-patientwith-an-implanted-thoracolumbar-spinalcord-stim.pdf. Accessed February 2023.
- Conklin M, Nussbaum AM. Electroconvulsive therapy for depression in patient with implanted spinal cord stimulator. J ECT. 2021;37:e22–e23. PMID: 34029307.
- Peroski MS, Chu MM, Doddi SR, Regenold WT. The safety of electroconvulsive therapy in patients with implanted deep brain stimulators: a review of the literature and case report. J ECT. 2019;35:84–90. PMID: 30407933.

First of all, thank you for the excellent article on the management of patients with NCIEDs. I agree that we are seeing more of these patients in our practice. Managing this workflow involves a tremendous amount of work, and just playing devil’s advocate, why should this be any of our work? Outside of doing a neuraxial procedure on someone with a SCS, this is all for protecting the patient from what the surgeon is contemplating. The surgeon who has NPs and a whole team around them. Similarly to position issues, this should really be the surgeon/cardiologists/psychiatrists’ responsibility. They are the ones using things that might adversely affect the devices, and doesn’t affect the anesthetic at all. I’m all for patient safety but there has to be some responsibility put on the person who is directly affecting the devices. We can be experts and consultants but all the perioperative concerns you outline so well do not involve anything we are doing that affects these devices.
Thank you for both your interest in our article and your comment. We appreciate your thought-provoking comment as we too have pondered who is ultimately responsible for the management of these devices in the perioperative period. While it is imperative that the managing provider of the device make recommendations prior to a scheduled procedure, we believe that there should be a collaborative approach with the surgical team, but led by the anesthetist in the perioperative period to ensure the safety of the patient. Similar to when your patient presents with a pacemaker or ICD, we are the ones responsible for assuring that these devices are in the appropriate surgery modes and/or off and that all personal are made aware of these devices and the changes needed. According to the ASA’s Statement on the Anesthesia Care Team, “anesthetic management includes the perioperative management of coexisting disease as well as the prevention and management of periprocedural complications.” When it comes to patient safety in the perioperative period, if you want it done right then the anesthetizing team should do it.