Watch the new APSF Operating Room Fire Safety Video: Surgical Fires – A Preventable Problem.
Read the original article at: https://www.apsf.org/article/from-the-literature-ecri-review-explains-warns-of-or-fires/
 The thought of a fire in the operating room sends chills down the spines of health care professionals that are trusted to ensure our patient’s safety. This dreaded complication which often results in severe and disfiguring injuries can be eradicated at a minimal cost and should be a continued focus for the APSF and other organizations of stakeholders. Extrapolated study data from the Pennsylvania Patient Safety Authority to the country as a whole indicate a recent reduction in the number of surgical fires from 650 to 217 events each year in the United States.1,2 While these data are encouraging, it magnifies the need to mandate reporting of surgical fires in all states, not just rely on a single state’s data. The actual number of fires is probably higher than estimated since only half of the states require mandatory reporting of such occurrences. Our optimism for news that surgical fire cases have dropped is offset by the rate of anecdotal incidents and the solicitations for expert opinions in legal proceedings which have not changed since APSF’s original efforts.
The thought of a fire in the operating room sends chills down the spines of health care professionals that are trusted to ensure our patient’s safety. This dreaded complication which often results in severe and disfiguring injuries can be eradicated at a minimal cost and should be a continued focus for the APSF and other organizations of stakeholders. Extrapolated study data from the Pennsylvania Patient Safety Authority to the country as a whole indicate a recent reduction in the number of surgical fires from 650 to 217 events each year in the United States.1,2 While these data are encouraging, it magnifies the need to mandate reporting of surgical fires in all states, not just rely on a single state’s data. The actual number of fires is probably higher than estimated since only half of the states require mandatory reporting of such occurrences. Our optimism for news that surgical fire cases have dropped is offset by the rate of anecdotal incidents and the solicitations for expert opinions in legal proceedings which have not changed since APSF’s original efforts.
In the ASA closed claims database, surgical fires accounted for 1.9% (103/5297) of the liability claims.3 Electrocautery induced fires increased from less than one percent of surgeries from 1985–1994 to 4.4% between 2000 and 2009.3 Unfortunately, the circumstances surrounding these cases remain unchanged over time: it is usually the use of open delivery of oxygen via nasal cannula or face mask, coupled with the use of a monopolar electrical surgical device within the area of the head and neck. Most claims occur in outpatient settings, involving the upper body (85%), and utilize monitored anesthesia care (MAC) (81%).3 The closed claims cases of OR fires with patients under general anesthesia, occur with otolaryngology procedures in which the FiO2 is greater than 0.30, ninety-seven percent of the time.3 The data indicate that claims were paid in seventy-eight percent of the cases with the median settlement value, $120,000.00.3
Many of the fires during MAC anesthesia occur when a clinician connects a nasal cannula or face mask to the auxiliary oxygen outlet. In most anesthesia workstations this outlet can only deliver 100% oxygen. However, some anesthesia workstations can now mix oxygen with air to provide a lower FiO2. For instance, the GE Carestation 650 incorporates an O2/air blender into the auxiliary gas outlet and analyzes the FiO2 of the gas mixture.4
High flow nasal oxygen is a newer technology that is being utilized in some MAC anesthesia cases. These devices can deliver 50–100 L/min of oxygen with an FiO2 of 1.0, unless an O2/air blender is used. These very high flow rates of oxygen present a markedly increased fire risk, unless great care is taken to ensure the oxygen is dissipated before the surgeon uses an electrosurgical unit (ESU) or laser.5
A particularly devastating type of OR fire can occur when a tracheal tube is ignited by a laser or ESU. In these cases, a “blowtorch” effect is created that can severely damage the airway and the lungs.4 The anesthesia professional must always use a tracheal tube that is protective to the wavelength of laser being used by the surgeon. Tracheostomies are another airway procedure that can result in an airway fire. This often occurs when the surgeon uses an ESU to enter the trachea in the presence of high oxygen concentrations. The resulting fire often results in major morbidity for the patient.6
“The Patient Is On Fire” is an article published by the ECRI Institute (previously known as the “Emergency Care Research Institute”) in the January 1992 issue of Health Devices.7 It describes the triad of fuels, oxidizers, and ignition sources that are still present in the modern operating room of 2020. Fuels include the alcohol-based surgical prep solutions, surgical drapes, towels, tracheal tubes, and laryngeal mask airways. Oxidizers include oxygen and nitrous oxide. Ignition sources include the ESU lasers, and fiberoptic lights.7
Alcohol-based surgical prep solutions can readily fuel an OR fire.8 Not only is the alcohol itself highly flammable, but the alcohol vapors formed during evaporation are also combustable. The OR team must ensure that the prep has completely dried and any alcohol-soaked towels are removed from the area before the patient can be draped.
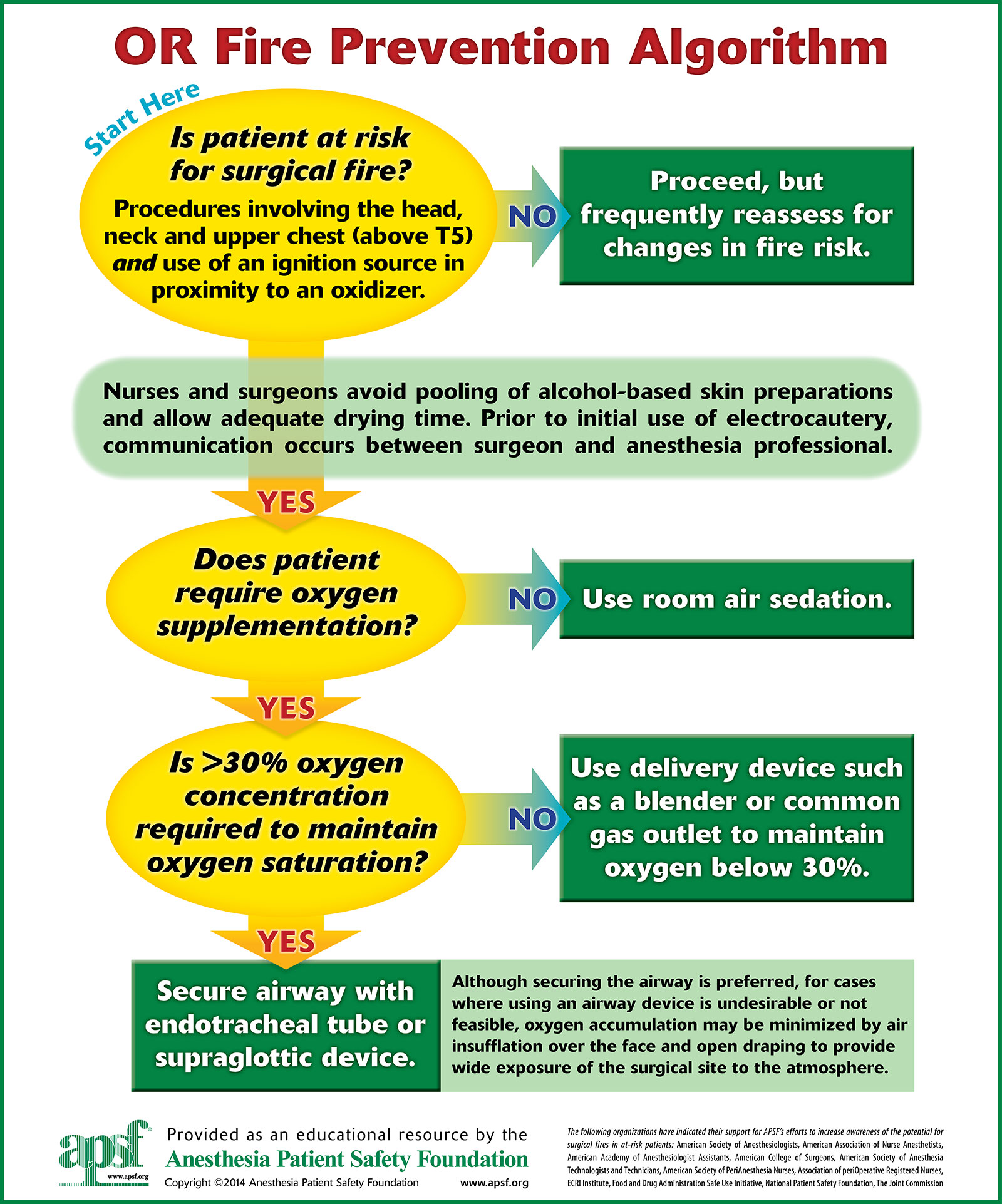
Figure 1: Fire Safety Algorithm (printable posters available at https://www.apsf.org/videos/or-fire-safety-video/
Surgical fires have been a key area for educational focus by the American Society of Anesthesiologists (ASA), the Anesthesia Patient Safety Foundation (APSF), the Association of periOperative Registered Nurses (AORN), and the National Fire Protection Association (NFPA). The APSF has created and revised a safety algorithm, which is provided on the APSF website and which can serve as a cognitive aid for health care professionals to avoid high-risk situations for OR fires. The ASA has also revised their OR Fire Prevention algorithm since its original publication (Figure 1).9
Educating physicians, nurses, technicians, and all surgical staff is vitally important. In 2013, the ASA published a practice advisory for health care providers in an effort to prevent surgical fires: 9
- Conduct a fire risk assessment at the start of every surgery. “A Fire Risk Assessment Tool” should be implemented before each surgery, in the “time out” or safety checklist. Assessment should be made to determine the presence of major risk factors such as: 1) Use of an open oxygen source; 2) The presence of an ignition source; 3) A procedure at or above the level of the xiphoid process; 4) Use of a flammable surgical prep solution.
- Encourage communication among surgical staff.
- Ensure the safe use and administration of oxidizers. Titrate the minimum concentration of oxygen necessary to meet the needs of the patient.
- Safely use any devices that may serve as an ignition source. Support personnel should be aware of the use and maintenance of any instrument that may ignite a fuel source.
- Safely use surgical suite items that may serve as a fuel source.
- Practice ways to manage surgical fires. The ASA practice advisory has offered several steps for managing a surgical fire: 1) Eliminate the primary ignition source. 2) Extinguish the fire and remove all sources of fuel. 3) Discontinue the patient from the breathing circuit for airway fires and remove the tracheal tube. Move the patient to safety and re-establish the airway. 4) Review the fire scene and remove any potential sources of flammable materials.3
If a fire should occur, it is important that every member of the OR team knows the location and use of a fire extinguisher. The ECRI and the ASA practice advisory recommend the carbon dioxide (CO2) extinguisher as the most appropriate for use in the OR.
Preventive measures to avoid fires in operating rooms have a place in our daily preparation. Knowledge of the risks should encourage yearly programs to prepare personnel, minimize patient injury as well as limit damage to the operating room. The APSF’s surgical fire video is frequently viewed and downloaded, and the content remains useful and accurate.10 The availability of treatment algorithms (Figure 1) for reference in each operating room and the performance of a fire risk assessment for each patient in the “time-out” certainly makes good clinical sense.
What is next regarding surgical fire prevention? The best answer is culture change. Integration of fire risk assessments and preventative actions in surgical safety checklists can mitigate this catastrophic and preventable event. We can also integrate surgical fire prevention into education simulation centers throughout the world. Engaging surgeons who perform high fire risk cases in prevention and education activities will ensure they are aware of the risks and can take mitigation steps when possible. We can also promote educational programs such as the “FUSE program” by SAGES (Fundamental Use of Surgical Energy by the Society of American Gastrointestinal and Endoscopic Surgeons) which is an excellent educational tool for surgeons and anesthesia professionals, as well as anyone working in the OR. As a specialty, we must remain engaged with professional organizations, standards groups, accreditors, and certification boards to ensure the topic of surgical fire prevention remains prominently positioned with emphasis on increasing knowledge and practice.
Anesthesia professionals are trained to be vigilant. Our patients trust us with their well being. Continual education and the knowledge of the risks as well as management in the event of an operating room fire continue to deserve our time and study. We emphasize that fire prevention requires zero additional cost and approaches 100% effectiveness. Therefore, we strongly believe that surgical fire prevention is a primary way in which to exemplify the APSF’s vision that “No one shall be harmed by anesthesia care.”
Charles E. Cowles, Jr., MD, MBA, FASA, is associate professor and chief safety officer at the University of Texas MD Anderson Cancer Center.
Chester Lake MD, MS, is assistant professor of anesthesiology at the University of Mississippi Medical Center.
Jan Ehrenwerth, MD is professor emeritus at Yale University School of Medicine.
The authors have no conflicts of interest.
References
- Surgical fires: decreasing incidence relies on continued prevention efforts. Pa Patient Saf Advis. 2018;15(2). Available at: http://patientsafety.pa.gov/ADVISORIES/Pages/201806_SurgicalFires.aspx. Accessed April 20, 2020.
- Cowles, CE. Fire Safety in the operating room. In: UpToDate, Nussmeier, N (Ed), UpToDate, Waltham, MA. https://www.uptodate.com/contents/fire-safety-in-the-operating-room/print Accessed June 25, 2020.
- Mehta SP, Bhananker SM, Posner KL, et al. Operating room fires: a closed claims analysis. Anesthesiology. 2013;118:1133–1139.
- Ehrenwerth J. Electrical and Fire Safety: Chapter 24. In: Ehrenwerth J, Eisenkraft JB, Berry JM, eds. Anesthesia Equipment: Principles and Applications, 3rd ed. Philadelphia: Elsevier: In Press.
- Cooper J, Griffiths B, Ehrenwerth J. Safe use of high flow nasal oxygen (HFNO) with special reference to difficult airway management and fire risk. APSF Newsletter. 2018;33:51–53. https://www.apsf.org/article/safe-use-of-high-flow-nasal-oxygen-hfno-with-special-reference-to-difficult-airway-management-and-fire-risk/ Accessed August 12, 2020.
- Lew EO, Mittleman RE, Murray D. Endotracheal tube ignition by electrocautery during tracheostomy: case report with autopsy findings. J Forensic Sci. 1991;36:1586–1591.
- ECRI Institute. The patient is on fire! A surgical fires primer. Health Dev. 1992:21:19–34.
- Barker SJ, Polson JS. Fire in the operating room: a case report and laboratory study. Anesth Analg. 2001;93:960–965.
- Apfelbaum JL, Caplan RA, Barker SJ, et al. Practice advisory for the prevention and management of operating room fires: an updated report by the American Society of Anesthesiologists Task Force on Operating Room Fires. Anesthesiology. 2013;118:271–290.
- Anesthesia Patient Safety Foundation: Prevention and Management of Operating Room Fires (Video). https://www.apsf.org/videos/or-fire-safety-video/; 2010. Accessed June 30, 2020.
