
![]()
Dear Q&A,
We write to describe an instance of anesthesia machine ventilator failure during provision of anesthesia. The case in point was an emergency vascular operation for a pulseless lower extremity. In preparation for the case, the anesthesia machine checkout was performed on the Dräger GS Premium. All tests confirmed that the anesthesia machine was indeed operational and ready for use.
The patient was brought to the operating room, and, after immediate re-evaluation, the patient was induced. After confirmation of bilateral breath sounds and verification of end-tidal CO2, manual ventilation was discontinued and the mechanical ventilation was initiated. At this point the ventilator immediately alarmed “Ventilator Failure!!!,” “Check APL Valve!!!,” “Apnea Pressure!!” (Figures 1, 2). Interestingly, there was no loss of tidal volumes at this point, and, contrary to the alarms, the ventilator appeared to function appropriately. Despite stopping mechanical ventilation and commencing manual ventilation, the alarm continued. After several minutes of inspection of the circuit, a small cut in the APL valve tubing was discovered. The tubing was replaced, the alarms ceased, an uneventful anesthetic ensued, and there were no untoward effects on the patient.
In an effort to delineate whether this type of ventilator failure can be discovered by routine automated machine checkout, we initiated mechanical ventilation mode both before and after making a small cut on the APL valve tubing. The machine passed the ventilator leak test, the system leak test, the compliance test, and the safety relief valves test after making the cut on the APL valve (Page 33, Figures 3, 4); yet , the ventilator flashed the same failure alarms as previously mentioned after mechanical ventilation was initiated. (Figures 1, 2).
The purpose of this letter is to remind anesthesia providers that successful automated machine checks, while useful, do not preclude the possibility of machine failures. Indeed, in a previous letter response to the APSF, it was noted by Dräger “No anesthesia system on the market has completely automated all aspects of the checkout procedures and eliminated the need for manual checkout” (APSF Newsletter, winter 2009–2010). The case highlighted above underscores this message and anesthesia team members should keep in mind this unique case of anesthesia machine failure.
Matthew Charous, MD Michael Presta, DO Scott Byram, MD Loyola University Medical Center Maywood, IL
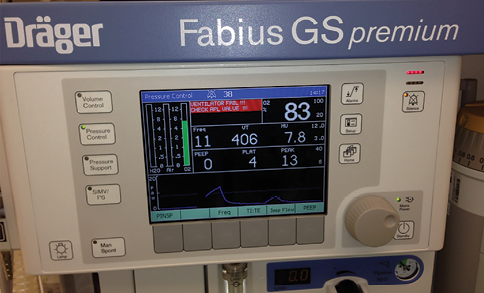
Figure 1. The authors successfully performed the anesthesia machine checkout on the Dräger GS Premium machine prior to anesthesia induction. At the initiation of mechanical ventilation, despite the machine passing checkout, the machine alarms sounded for “Ventilator Failure!!!,” “Check APL Valve!!!,” “Apnea Pressure!!”
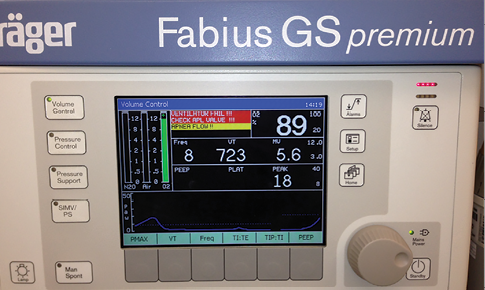
Figure 2. Despite the ventilator alarms, there was no loss of tidal volumes, and the ventilator appeared to function appropriately. The alarms continued—even after resumption of manual ventilation. Close inspection revealed a small cut in the APL valve bypass tubing as the source of the problem.
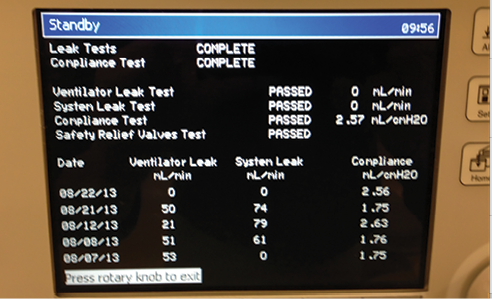
Figure 3. In an effort to replicate this scenario and to delineate whether this type of ventilator failure can be discovered by routine, automated machine checkout, the authors initiated mechanical ventilation mode both before and after making an intentional small cut on the APL valve bypass tubing. The machine passed the ventilator leak test, the system leak test, the compliance test, and the safety relief valves test after the cut in the APL tubing was made, but the venilator alarms sounded once mechanical ventilation was started. (Read Dr. Paulsen’s answer to find out how to prevent this scenario from happening to you.)
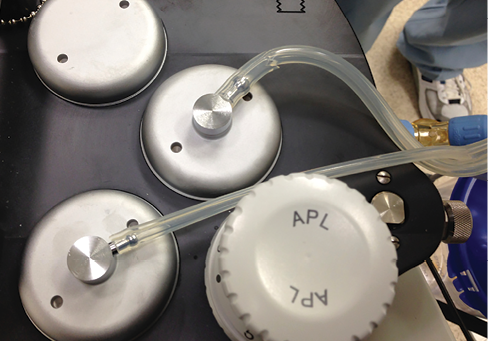
Figure 4. Small cut on the APL valve bypass tubing (red arrow).
![]() Dear Dr. Charous,
Dear Dr. Charous,
Dr. Charous and colleagues aptly point out that the automated machine checkout procedures do not preclude the possibility of machine failure. Carrying this concept a step further would be to recognize that the more solenoid valves and electronics that have to be added to completely and automatically check every aspect of anesthesia performance, the more there is potential for catastrophic events to occur.
In Charous’ reported incident, the anesthesia machine performed exactly as designed. The automated checkout procedure did not find any faults among those machine elements that were part of the automated test algorithm. In spontaneous/manual ventilation mode, the machine performed as expected. However, when the ventilator was switched on, with a leak in the APL bypass hose, the machine quickly alarmed, announcing “ventilator Failure Check APL Valve” indicating a leak in the APL Bypass hose. The machine reverted to spontaneous/manual ventilation mode, enabling the patient to be manually ventilated.
This incident emphasizes the need for an enhanced checkout procedure that includes a functional test of the breathing circuit and ventilator. Before applying the breathing circuit to the patient, the breathing bag should be removed from the bag arm and connected to the circuit elbow or wye piece. The oxygen flush should be used to inflate the breathing bag, which is acting as a lung. The ventilator should be activated and the “lung” observed for inflation and deflation with each breath. The breathing circuit pressure should be checked along with the exhaled volume. Only after a successful test should the breathing bag be returned to the bag arm and the APL valve set to minimum in preparation for the patient. Employing such a test every time the machine is to be used will uncover a number of breathing circuit issues that could interfere with ventilation of the patient.
A. William Paulsen, PhD, AA-C Chair, APSF Committee on Technology
The APSF sometimes receives questions that are not suitable for the Dear SIRS column. This Q and A column allows the APSF to forward these questions to knowledgeable committee members or designated consultants. The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or group responses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of the APSF. It is not the intention of the APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall the APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
