Introduction
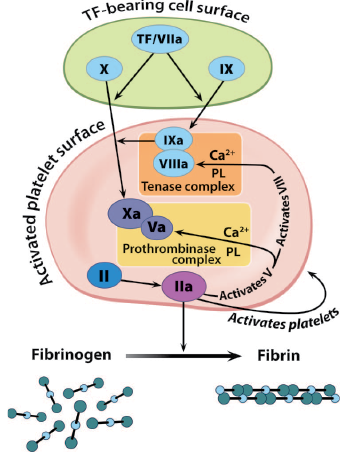
Figure 1. The coagulation cascade. TF = tissue factor; PL = phospholipids.
The increasing use of the direct oral anticoagulants (DOACs) has provided clinicians and patients with alternatives to warfarin for the treatment of venous thromboembolism (VTE), the prevention of cerebrovascular embolic stroke in patients with atrial fibrillation, and thromboprophylaxis in patients undergoing surgery. Four DOACs are currently approved in most countries and have added a novel paradigm for anticoagulation management. However, providers should be aware of perioperative management strategies regarding patients on these agents for both elective and emergency surgery. Currently, a specific reversal agent, idarucizumab, is available for dabigatran, and clinical trials are currently underway for reversing apixaban, rivaroxaban, and edoxaban. In this review, a group of international experts will review perioperative management strategies that include when to stop these drugs for elective surgery or invasive procedures, how to assess and monitor their anticoagulant effects, current protocols for temporary discontinuations of DOAC therapy, and the utility of specific DOAC reversal agents.
Direct Oral Anticoagulants Currently Available
The currently available non-vitamin K DOACs include the direct thrombin inhibitor dabigatran etexilate (Pradaxa®, Boehringer-Ingelheim Pharma), and direct factor Xa inhibitors, rivaroxaban (Xarelto®, Johnson and Johnson/Bayer HealthCare), apixaban (Eliquis®, Bristol Myers Squibb/Pfizer), and edoxaban (Savaysa®, Daiichi Sankyo). The advantages of the DOACs include a rapid onset of action, with a peak effect two to four hours following oral administration, predictable anticoagulant/pharmacodynamic effects, minimal drug interactions, and no present requirement for routine laboratory monitoring. The particular use of each individual agent depends upon multiple factors including current approval, labelling of the drugs, availability, and country-specific approved dose regimens. Of note, there are multiple reviews related to these agents, and a growing body of literature.1-3
One of the important consistent findings from multiple publications is that, compared with warfarin, DOACs have a lower risk for intracranial bleeding and as low or a lower risk for other types of bleeding.4 Warfarin, a vitamin K antagonist, produces an anticoagulant effect by reducing circulating levels of coagulation factors II, VII, IX, and X.5 Although giving vitamin K is a logical reversing agent, its effect is not immediate and time is required to reverse the INR, and it takes 24 to 72 hours to restore adequate levels of functional coagulation factors. On the other hand, the DOACs are reversible direct pharmacologic inhibitors of either thrombin or factor Xa, two critical targets of the hemostatic cascade that have a pharmacologic effect similar to other commonly used parenteral anticoagulants such as low-molecular-weight heparin (LMWH), heparin, or other direct thrombin inhibitors (i.e., bivalirudin, argatroban).3
Although, in general, DOACs have a lower risk of bleeding,6-8 managing anticoagulation in the perioperative period is problematic because all anticoagulants can cause bleeding.9 Despite their apparent safety compared with warfarin, perioperative management strategies for patients receiving DOACs require specific considerations. In a recent international survey, we observed that physicians had limited knowledge about the perioperative management of patients treated with DOACs.10 The evaluation of DOAC-treated patients for procedural interventions should include documenting the timing of the last DOAC dose, renal function that influences elimination time, and the procedure-associated bleeding risk that affects interruption timing. DOACs require specific coagulation assays to measure anticoagulation levels accurately (i.e., dilute thrombin time for dabigatran, anti-Xa levels for oral Xa inhibitors), although standard coagulation screening tests (i.e., prothrombin time [PT] for rivaroxaban, activated partial thromboplastin time [aPTT] for dabigatran) may provide a qualitative assessment if there is a residual DOAC anticoagulant effect.
Specialty societies have endorsed general recommendations for patient management to promote hemostasis in anticoagulated patients requiring surgery or other invasive procedures. These include general stopping rules (such as ≥24 hours for low bleed-risk procedures and ≥48 hours for high bleed-risk surgery in patients with normal renal function) for elective procedures. Switching to LMWH, in general, is not required during periprocedural DOAC interruption because of the rapid offset and onset of DOACs.2
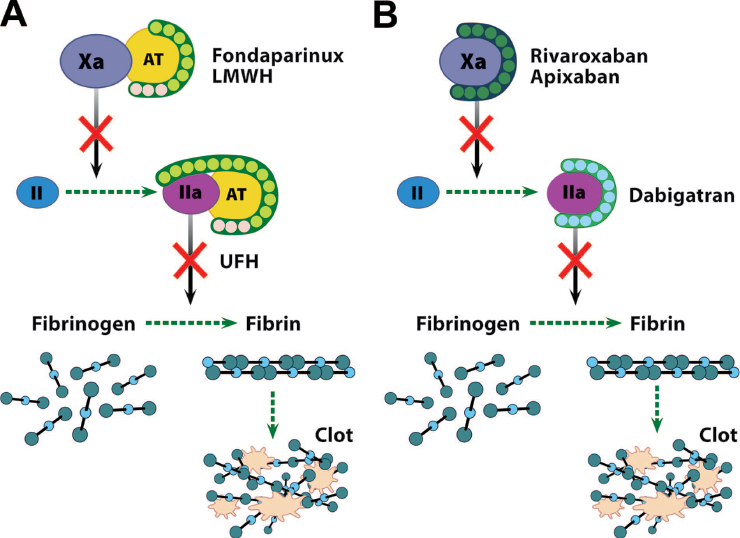
Reproduced with permission. Levy JH, Key NS, Azran MS. Novel oral anticoagulants: implications in the perioperative setting. Anesthesiology 2010;113:728. Figure 2. The primary mechanism of action of the established anticoagulants (unfractionated heparin [UFH], low-molecular-weight heparin [LMWH], and fondaparinux) via antithrombin-dependent binding (A) and the new anticoagulants (rivaroxaban, apixaban, and dabigatran etexilate) via antithrombin-independent binding (B). UFH also inactivates factors Xa, IXa, XIa, and XII via antithrombin, but to a lesser extent than inactivation of thrombin. LMWH also inactivates thrombin via antithrombin, but to a lesser extent than inactivation of factor Xa. AT = antithrombin.
Preoperative Management of Patients Receiving DOACs
Specific considerations for the preoperative management of DOAC-treated patients include pharmacokinetics of the particular drug, renal function, and specific considerations regarding whether the surgery requires emergency intervention or is elective, and the particular risk of thrombosis and bleeding of the individual surgical procedure. Based on the availability of idarucizumab as a specific antidote for dabigatran, patients can be readily managed if they require emergent or urgent surgical or procedural interventions. Although other reversal strategies for oral Xa inhibitors are under investigation, none of them today have been studied in patients requiring emergent procedural interventions. Other potential off-label therapies have been evaluated and will be considered subsequently.
Dabigatran etexilate is the only oral direct thrombin inhibitor. Dabigatran is a prodrug that is encapsulated to allow for absorption in the gut and its major mechanism of metabolism is via renal elimination (~80%). Apixaban, rivaroxaban, and edoxaban are direct factor Xa inhibitors, and are primarily hepatically metabolized (~65–70%). Clinicians should consider the half-life of the DOACs approximately 12 hours in most patients unless they have reduced renal function. Dabigatran elimination is the most dependent on renal function, and preoperative interruption should be based on creatinine clearance (CrCl) calculated according to the Cockcroft-Gault formula.11,12 Renal function is less an issue with rivaroxaban, apixaban, and edoxaban unless there is severe renal insufficiency.13
Multiple recommendations for perioperative management of DOAC-treated patients exist but such recommendations should be considered as potential therapeutic guidance statements given that prospective standardized management protocols are still in de
velopment, and are also based on specific drug recommendations as well.2,14,15 These recommendations are based on an international group of physicians, many of whom are authors of the present article. Readers should examine the American Society for Regional Anesthesia (ASRA) guidelines for discontinuation of anticoagulants prior to regional anesthesia. (https://www.asra.com/advisory-guidelines/article/1/anticoagulation-3rd-edition).
In general, management is based on procedure-related bleeding risk. Selected minimal bleeding risk procedures are likely to be safely undertaken without DOAC interruption (e.g., minor dental procedures, cataract surgery, pacemaker implantaion, skin biopsies) although prospective validation studies are needed. Other procedures can be classified as low bleeding risk (e.g., laparoscopic cholecystecomy or hernia repair), or high bleeding risk (e.g, cardiovascular, intracranial or spine surgery, major cancer surgery, any surgery with spinal or epidural anesthesia).
The European Society of Anaesthesiology and the French Working Group on Perioperative Haemostasis (GIHP) recommend interruption of DOAC therapy ~24 hours (two or three half-lives) before an elective low bleeding risk procedure (non-regional anesthesia related), and 5 days before a medium or high bleeding risk procedure. These recommendations also account for patient’s renal function.16,17The European Heart Rhythm Association’s guide to DOAC use for elective surgery suggests a general stopping rule of ≥24 hours for low-risk procedures and ≥48 hours for high-risk surgery. However, longer interruption intervals are suggested for patients with CrCl <80 mL/min on dabigatran and those with CrCl 15 to 30 mL/min on oral Xa inhibitors.2,18 Other expert consensus documents recommend a 24- to 48-hour interruption interval based on the specific DOAC, renal function, and procedural bleeding risk.19,20 However, as a reminder, caution should be considered for preoperative bridging of any oral anticoagulant with LMWH as noted in recent recommendations and clinical trials.20,21
Additional studies to assess standardized perioperative management protocols in DOAC-treated patients are ongoing.19,22 The management of patients who are receiving DOACs and require emergency surgery or other procedural intervention due to trauma or other emergencies continues to evolve as we develop additional management strategies that will be subsequently discussed.
Measurement of Anticoagulation with the DOACs
One of the major advantages of the DOACs is that routine anticoagulation monitoring is not presently required due to predictable pharmacokinetic and pharmacodynamic properties. However, following acute traumatic injury or in patients who require emergency surgical or otherwise procedural intervention, anticoagulation monitoring may be helpful.23,24 Other information important to obtain for the clinician to guide potential interpretation and management of the results includes the history of when the last dose of anticoagulant was taken, the patient’s renal function, and other potential concomitant medications including potential antiplatelet therapies.23
In dabigatran-treated patients, standard coagulation testing can be used to determine potential effects. The aPTT assay is an effective screening assay to determine a potential anticoagulation effect due to dabigatran, and a prolonged aPTT is consistent with an anticoagulant effect as reported. (http://www.nejm.org/doi/suppl/10.1056/
NEJMoa1502000/suppl_file/nejmoa1502000_appendix.pdf). However, a normal aPTT does not exclude residual anticoagulant effect. A normal thrombin time or diluted thrombin time will exclude an anticoagulant effect of dabigatran. In addition, the dilute thrombin time provides a more reliable and precise measurement of the anticoagulant effect of dabigatran, an assay not currently cleared by FDA but available in specialized centers.25,26 In Europe, the calibrated Hemoclot® thrombin inhibitor assay (Hyphen BioMed, Neuville-sur-Oise, France) is recommended as the method of assessing anticoagulation in dabigatran-treated patients.27 In Europe, the ecarin clotting time (ECT) assay is also commonly used in specialized centers to evaluate anticoagulation in dabigatran-treated patients.28
Monitoring and/or assessing the effects of the anti-Xa “xaban” agents is more complicated despite their growing use as the mainstays of DOAC therapy. Although the INR is used routinely to monitor anticoagulation with vitamin K antagonists, it is not a dependable or specific assay for assessing the anticoagulant effects of the DOACs.25 Following traumatic injury or major surgery, patients routinely have a prolonged PT due to multiple causes and, therefore, it is an insensitive assay of the anticoagulant effects of Xa inhibitors, especially apixaban.29-31 If levels are required, then specific drug-calibrated factor Xa assays, similar to those used to determine low molecular weight heparin concentrations are available in some institutions. These potential quantitative measurements of the “xabans” are calibrated in anti-Xa units and have been reported for rivaroxaban and apixaban,32,33 and edoxaban.34 These assays are not widely available, require specific calibration to each individual agent, and are rarely available on an urgent basis outside of specialized centers.25,31 The different coagulation assays currently available for each DOAC are listed in Table 1.
Table 1. Assays for Monitoring Direct Oral Anticoagulant Activity1,2
| Drug | Quantitative Assays (Provides an Estimate of Anticoagulant Drug Levels) |
Qualitative Assays (to Indicate Presence or Absence of Drug Effect) |
Not Recommended |
| Direct Factor Xa inhibitors (apixaban/ rivaroxaban/ edoxaban) |
Specific, calibrated anti-Factor Xa assays | None currently available | Prothrombin time (except rivaroxaban where there may be a dose-related prolongation), activated partial thromboplastin time, dilute thrombin time or thrombin time assays, or heparin-specific assays such as the activated clotting time assay |
| Direct thrombin inhibitor (dabigatran) | Dilute thrombin time assay (available in some specialized centers in US, ecarin clotting time (not available in US) | Activated partial thromboplastin time, thrombin time | Chromogenic anti-Factor Xa assays, heparin-specific assays such as the activated clotting time assay |
Interruption of Oral Anticoagulation and Bridging/Switching Between Anticoagulants
Previously reported guidelines for periprocedural and/or preoperative management of patients on warfarin anticoagulation included discontinuing warfarin and proceeding with the use of LWMH or unfractionated heparin to bridge patients with atrial fibrillation who were at increased risk for thromboembolic events.35,36 More recent data on anticoagulant bridging to allow for procedural interventions and invasive procedures to proceed has been called into question.37,38 Guidelines from the American Academy of Neurology report that bridging therapy with heparin is associated with increased risk of bleeding compared to warfarin discontinuation.39 In a large, randomized study of atrial fibrillation patients reported by Douketis et al. in 2015 from the BRIDGE investigators, stopping warfarin without LMWH bridging was non-inferior to bridging therapy for arterial thromboembolism when warfarin treatment was interrupted for an elective operation or other elective invasive procedure and was associated with a significant decrease in post-procedural major and minor bleeding.21
For patients anticoagulated with DOACs, the limited data currently available suggest that perioperative bridging with LMWH during DOAC interruption provides no therapeutic benefit and can lead to increased major bleeding. In a recent sub-analysis of data from the RE-LY trial, where dabigatran-treated patients who had treatment interruption for an elective procedure, experienced more major bleeding events with bridging therapy than patients who did not receive bridging therapy, with no significant effect on arterial thromboembolism.40 As a result, bridging therapy is not indicated when anticoagulation needs to be interrupted for short intervals of approximately 24 to 48 hours in advance of an invasive or surgical procedure.28 Similar guidance and recommendations are also suggested for apixaban.41,42 Treatment with apixaban, rivaroxaban, and edoxaban should be stopped at least 24 hours before an invasive or surgical procedure of low risk, but may require longer discontinuation intervals for procedures with a moderate to high risk of bleeding. There is ongoing interest regarding whether certain procedures, particularly pacemaker or defibrillator implantation, can be done without DOAC interruption. Randomized controlled trials currently underway, such as BRUISE CONTROL-2, are expected to inform best practices for such patients.43
Reversal of DOAC-induced Anticoagulation With Specific Agents
When anticoagulated patients present for emergency surgery or following traumatic injury, bleeding is an expected and feared risk in DOAC- or warfarin-treated patients among those perioperative providers caring for them. Therefore, specific reversal agents are under development for all DOACs.
For patients on dabigatran, idarucizumab, a specific reversal agent, is currently approved in many countries for dabigratran reversal in cases of serious bleeding or emergency surgery/procedures. Idarucizumab is a humanized monoclonal antibody that selectively binds dabigatran and reverses dabigatran-induced anticoagulation. In the REVERSE-AD study, idarucizumab reversed the anticoagulant effects of dabigatran in patients with a major bleeding event, or in need of an urgent invasive procedure (within the next 8 hours).44,45 Following intravenous administration, idarucizumab reversal is immediate and lasts for at least 24 hours. Idarucizumab was approved in 2015 by the United States Food and Drug Administration for the reversal of dabigatran-related anticoagulation in cases where emergency surgery and/or urgent procedures are required, or in cases of life-threatening or uncontrolled bleeding.46 An American Heart Association report suggested that a 5 g dose of idarucizumab resulted in immediate and complete reversal of dabigatran anticoagulation in 82–99% of critically ill elderly patients taking dabigatran who presented with life-threatening emergencies, and intraoperative hemostasis was judged by surgeons as “normal” in 93% of the surgical/procedural patients. This study included approximately 200 complex, critically ill patients undergoing a multitude of orthopedic, surgical, and other procedures in a high-risk patient population.47
Andexanet-alfa is in phase III clinical trials as a specific reversal agent for emergency reversal of apixaban, edoxaban, rivaroxaban, fondaparinux, and the low molecular weight heparins such as enoxaparin.48,49 It is important to realize that andexanet-alfa has not been studied for reversal of anticoagulation in surgical patients to date. Andexanet-alfa is a bioengineered human factor Xa decoy protein. By binding to circulating factor Xa inhibitors, andexanet-alfa makes endogenous factor Xa available to contribute to the coagulation cascade.49,50 Ciraparantag is another drug in early evaluation as a reversal agent for factor Xa inhibitors and low molecular weight heparin, but is not currently available.51,52
Currently, when DOAC-treated patients present for emergency surgery or procedural interventions receiving one of the anti-Xa agents, management strategies are needed. Growing data from case reports, in vitro studies, and volunteers suggest some efficacy for the ability of prothrombin complex concentrates (PCCs) to reverse DOACs.51-53 At least one registry trial is underway to assess outcomes in bleeding patients or those requiring urgent care treated with DOACs and reversed with PCCs, and other potential agents. As previously discussed, in emergency situations where patients are bleeding and have taken anti-Xa agents, the ability to rapidly measure therapeutic effects or drug levels with the Xa inhibitors is limited.
One particular noteworthy study evaluated a 5 mm punch biopsy in healthy subjects receiving a single dose of 60 mg edoxaban. The authors noted that four factor-prothrombinanse complex concentrate (4F-PCC) produced a dose-dependent reversal of edoxaban’s effect on bleeding duration, bleeding volume, and thrombin generation and normalized values to baseline levels before anticoagulation using a 50 IU/kg dose of 4F-PCCs.53 However, PT was only partially reversed and this is a consistent finding in all of the PCC reversals of anti-Xa agents.53 In the volunteers who underwent reversal of anticoagulation, there were no safety issues and no thromboembolic events. Notably, this is the only study to evaluate a specific bleeding parameter associated with DOAC reversal using a four factor PCC.53
Summary:
The DOACs have provided important additional therapeutic approaches for anticoagulation in patients. The benefits as previously discussed include predictable pharmacokinetics, no present requirement for routine monitoring, and overall the potential for fewer risks of bleeding and improved outcomes as noted in the multiple studies that led to approval by the Food and Drug Administration. As with any anticoagulants, the drug should be stopped for high-risk surgical procedures in patients at increased risk for bleeding, and for all the agents, renal function should be considered. Monitoring can be used in elective surgical interventions, but for emergencies, the availability and need for emergent or urgent surgery is an important consideration. For dabigatran, idarucizumab is a specific reversal agent that has been studied in a multiplicity of surgical patients. For
the “xbans,” currently there is no approved agent available for specific reversal, and andexanet has not been studied as of yet in surgical patients. Therefore, clinicians need an alternative therapeutic approach, and off-label use of prothrombin complex concentrates has been reported, but all procoagulants pose prothrombotic risks as well. Nonetheless, clinicians need therapeutic approaches when dealing with emergencies and bleeding in surgical patients. In managing patients who are bleeding, standard approaches should always be considered, including hemostatic and hemodynamic support, and with life-threatening hemorrhage, the use of massive transfusion protocols.
Jerrold H. Levy is Professor in the Department of Anesthesiology and Intensive Care, Duke University School of Medicine, Durham, NC.
Pierre Albaladejo is Professor in the Department of Anesthesiology and Intensive Care Medicine, Grenoble University Hospital, Grenoble, France.
Charles-Marc Samama is Professor in the Department of Anesthesiology and Intensive Care Medicine, Assistance Publique-Hôpitaux de Paris, Cochin University Hospital, Paris, France.
Beverley Hunt is Professor at the Thrombosis & Haemophilia Centre, Guy’s & St Thomas’ NHS Foundation Trust, London, England.
Alex C Spyropoulos is Professor in the Department of Medicine, Northwell Health Systems at Lenox Hill Hospital, New York, NY, US.
James Douketis is Professor in the Department of Medicine, McMaster University, Canada.
Disclosures:
J Levy: Scientific Advisory Boards: Bayer, Boehringer-Ingelheim, CSL Behring, Grifols, Instrumentation Laboratories, Jiangsu Singchn, Janssen, Leading Biosciences, and Pfizer.
P Abaladejo: Scientific Advisory Boards: Octapharma, CSL Behring, LFB, Bayer, Boehringer-Ingelheim, CSL Behring, Sanofi, BMS-Pfizer, Daichii-Sankyo. Research support Boehringer-Ingelheim and Portola.
CM Samama: Scientific Advisory Boards: AstraZeneca, Bayer, BMS, Boehringer-Ingelheim, Daichii-Sankyo, Fresenius-Kabi, GSK, Haemonetics, Lilly, Pfizer, Roche, Sanofi; Research support: Bayer, BMS, Boehringer-Ingelheim, LFB, GSK, Haemonetics, Sanofi.
B Hunt: none
A Spyropoulos: Scientific Advisory Boards: Bayer, Janssen, Pfizer, Daiichi-Sankyo, Boehringer Ingelheim, Sanofi, Consultant: Boehringer Ingelheim, Bristol Myers Squibb, Pfizer, Janssen, and Daiichi Sankyo.
J Douketis: Scientific Advisory Boards/Education: Astra-Zeneca, Bayer, Boehringer-Ingelheim, Bristol-Myers-Squibb, Leo Pharma, Pfizer, Sanofi. Consultant: Janssen.
This article does not reflect the opinion of the editors or the APSF. The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Content is provided for purposes of education or discussion, and comprises neither statements of advice nor the opinions of the APSF. It is not the intention of the APSF to provide specific medical or legal advice or to endorse any specific views or recommendations. In no event shall the APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
References
- Raval AN, Cigarroa JE, Chung MK, Diaz-Sandoval LJ, Diercks D, Piccini JP, et al. Management of patients on non-vitamin K antagonist oral anticoagulants in the acute care and periprocedural setting: a scientific statement from the American Heart Association. Circulation 2017;135: e604–e33.
- Heidbuchel H, Verhamme P, Alings M, Antz M, Diener HC, Hacke W, et al. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace 2015;17:1467–507.
- Levy JH, Spyropoulos AC, Samama CM, Douketis J. Direct oral anticoagulants: new drugs and new concepts. JACC Cardiovascular Interventions 2014;7:1333–51.
- Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 2014;383:955–62.
- Gulati G, Hevelow M, George M, Behling E, Siegel J. International normalized ratio versus plasma levels of coagulation factors in patients on vitamin K antagonist therapy. Arch Pathol Lab Med 2011;135:490–4.
- Beyer-Westendorf J, Forster K, Pannach S, Ebertz F, Gelbricht V, Thieme C, et al. Rates, management and outcome of bleeding complications during rivaroxaban therapy in daily care: results from the Dresden NOAC registry. Blood 2014; 124:955–962.
- Healey JS, Eikelboom J, Douketis J, Wallentin L, Oldgren J, Yang S, et al. Periprocedural bleeding and thromboembolic events with dabigatran compared with warfarin: results from the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) randomized trial. Circulation 2012;126:343–8.
- Beyer-Westendorf J, Gelbricht V, Förster K, Ebertz F, Köhler C, Werth S, et al. Peri-interventional management of novel oral anticoagulants in daily care: results from the prospective Dresden NOAC registry. Eur Heart J 2014;35:1888–1896.
- Levy JH. Role of coagulation factor concentrates for reversing dabigatran-related anticoagulation. Anesthesiology 2014;120: 1316–1318.
- Faraoni D, Samama CM, Ranucci M, Dietrich W, Levy JH. Perioperative management of new oral anticoagulants: an international survey. Clinics Lab Med 2014; 34:637–654.
- Stangier J, Rathgen K, Stähle H, Mazur D. Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate: an open-label, parallel-group, single-centre study. Clinical Pharmacokinetics 2010;49:259–68.
- Reilly PA, Lehr T, Haertter S, Connolly SJ, Yusuf S, Eikelboom JW, et al. The effect of dabigatran plasma concentrations and patient characteristics on the frequency of ischemic stroke and major bleeding in atrial fibrillation patients: the RE-LY Trial (Randomized Evaluation of Long-Term Anticoagulation Therapy). J Am Coll Cardiol 2014;63:321–8.
- Kubitza D, Becka M, Mueck W, Halabi A, Maatouk H, Klause N, et al. Effects of renal impairment on the pharmacokinetics, pharmacodynamics and safety of rivaroxaban, an oral, direct Factor Xa inhibitor. Br J Clin Pharmacol 2010;70:703–12.
- Albaladejo P, Bonhomme F, Blais N, Collet JP, Faraoni D, Fontana P, et al. Management of direct oral anticoagulants in patients undergoing elective surgeries and invasive procedures: updated guidelines from the French Working Group on Perioperative Hemostasis (GIHP) – September 2015. Anaesth Crit Care Pain Med 2017;36:73–6.
- Faraoni D,Levy JH, Albaladejo P, Samama CM, Groupe d’Interet en Hemostase P. Updates in the perioperative and emergency management of non-vitamin K antagonist oral anticoagulants. Crit Care 2015;19:203.
- Gogarten W, Vandermeulen E, Van Aken H, Kozek S, Llau JV, Samama CM. Regional anaesthesia and antithrombotic agents: recommendations of the European Society of Anaesthesiology. Eur J Anaesthesiol 2010;27:999–1015.
- Sié P, Samama CM, Godier A, Rosencher N, Steib A, Llau JV, et al. Surgery and invasive procedures in patients on long-term treatment with direct oral anticoagulants: thrombin or Factor-Xa inhibitors. Recommendations of the Working Group on Perioperative Haemostasis and the French Study Group on Thrombosis and Haemostasis. Arch Cardiovasc Dis 2011;104:669–76.
- Heidbuchel H, Verhamme P, Alings M, Antz M, Hacke W, Oldgren J, et al. EHRA practical guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation: executive summary. Eur Heart J 2013;34:2094–106.
- Spyropoulos AC, Douketis JD. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood 2012;120:2954–62.
- Spyropoulos AC, Al-Badri A, Sherwood MW, Douketis JD. Periprocedural management of patients receiving a vitamin K antagonist or a direct oral anticoagulant requiring an elective procedure or surgery. J Thromb Haemost 2016;14:875–85.
- Douketis JD, Spyropoulos AC, Kaatz S, Becker RC, Caprini JA, Dunn AS, et al. Perioperative bridging anticoagulation in patients with atrial fibrillation. N Engl J Med 2015;373:823–33.
- Schulman S, Carrier M, Lee AY, Shivakumar S, Blostein M, Spencer FA, et al. Perioperative management of dabigatran: a prospective cohort study. Circulation 2015;132:167–73.
- Levy JH, Faraoni D, Spring JL, Douketis JD, Samama CM. Managing new oral anticoagulants in the perioperative and intensive care unit setting. Anesthesiology 2013;118:1466–74.
- Samama MM, Guinet C. Laboratory assessment of new anticoagulants. Clinical chemistry and laboratory medicine. CCLM/FESCC 2011;49:761–72.
- Lippi G, Favaloro EJ. Recent guidelines and recommendations for laboratory assessment of the direct oral anticoagulants (DOACs): is there consensus? Clinical Chemistry and Laboratory Medicine 2015;53:185–97.
- Stangier J, Feuring M. Using the HEMOCLOT direct thrombin inhibitor assay to determine plasma concentrations of dabigatran. Blood Coagul Fibrinolysis 2012;23:138–43.
- Boehringer Ingelheim Pharma GmBH. Pradaxa® (dabigatran etexilate) prescriber guide for stroke prevention in atrial fibrilation. 2015 Available at: https://www.pradaxa.co.uk/assets/downloads/spaf-prescriber-guide.pdf.
- Boehringer Ingelheim Pharmaceuticals Inc. Pradaxa prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2015 [updated September 2015]. Available at: http://bit.ly/1r26yMg.
- Douxfils J, Chatelain C, Chatelain B, Dogne JM, Mullier F. Impact of apixaban on routine and specific coagulation assays: a practical laboratory guide. Thrombosis and Haemostasis 2013;110:283–94.
- Cuker A. Laboratory measurement of the non-vitamin K antagonist oral anticoagulants: selecting the optimal assay based on drug, assay availability, and clinical indication. Journal of Thrombosis and Thrombolysis 2015;41:1282–7.
- Konigsbrugge O, Quehenberger P, Belik S, Weigel G, Seger C, Griesmacher A, et al. Anti-coagulation assessment with prothrombin time and anti-Xa assays in real-world patients on treatment with rivaroxaban. Annals of Hematology 2015;94:1463–71.
- Barrett YC, Wang Z, Frost C, Shenker A. Clinical laboratory measurement of direct Factor Xa inhibitors: Anti-Xa assay is preferable to prothrombin time assay. Thromb Haemost 2010;104:1263–71.
- Lindhoff-Last E, Ansell J, Spiro T, Samama MM. Laboratory testing of rivaroxaban in routine clinical practice: When, how, and which assays. AnnMed 2013;45:423–9.
- Daiichi Sankyo Inc. Savaysa® prescribing information. Parsippany, NJ 07054 USA. 2015 [updated September 2015]. Available from: http://dsi.com/prescribing-information-portlet/getPIContent?productName=Savaysa&inline=true.
- du Breuil AL, Umland EM. Outpatient management of anticoagulation therapy. American Family Physician 2007;75:1031–42.
- Hirsh J, Guyatt G, Albers GW, Schunemann HJ. Proceedings of the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy: evidence-based guidelines. Chest 2004;126:172S–696S.
- Steinberg BA, Peterson ED, Kim S, Thomas L, Gersh BJ, Fonarow GC, et al. Use and outcomes associated with bridging during anticoagulation interruptions in patients with atrial fibrillation: findings from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF). Circulation 2015;131:488–94.
- Shaikh AY, McManus DD. A bridge too far? Findings of bridging anticoagulation use and outcomes in the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF). Circulation 2015;131:448–50.
- Armstrong MJ, Gronseth G, Anderson DC, Biller J, Cucchiara B, Dafer R, et al. Summary of evidence-based guideline: periprocedural management of antithrombotic medications in patients with ischemic cerebrovascular disease: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2013;80:2065–9.
- Douketis JD, Healey JS, Brueckmann M, Eikelboom JW, Ezekowitz MD, Fraessdorf M, et al. Perioperative bridging anticoagulation during dabigatran or warfarin interruption among patients who had an elective surgery or procedure. Substudy of the RE-LY trial. Thrombosis and Haemostasis 2015;113:625–32.
- Bristol-Myers Squibb Inc. Eliquis® prescribing information. Bristol-Myers Squibb Company; 2015 [updated September 2015]. Available at: http://packageinserts.bms.com/pi/pi_eliquis.pdf.
- Janssen Pharmaceuticals Inc. Xarelto® prescribing information. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2015 [updated September 2015]. Available at: http://bit.ly/1Iq2OcA.
- EssebagV, Healey JS, Ayala-Paredes F, Kalfon E, Coutu B, Nery P, et al. Strategy of continued vs. interrupted novel oral anticoagulant at time of device surgery in patients with moderate to high risk of arterial thromboembolic events: The BRUISE CONTROL-2 trial. American Heart Journal 2016;173:102–7.
- Pollack CV, Jr., Reilly PA, Eikelboom J, Glund S, Verhamme P, Bernstein RA, et al. Idarucizumab for dabigatran reversal. N Engl J Med 2015;373:511–20.
- Levy JH, Verhamme P, Sellke FW, Reilly. PA, Dubiel R, Eikelboom J, et al. Initial experience with idarucizumab in dabigatran-treated patients requiring emergency surgery or intervention: interim results from the RE-VERSE AD™ Study. European Society of Cardiology Congress 29 August–2 September 2015; London, UK2015.
- Inc BIP. Praxbind® prescribing information. Ridgefield, CT 06877 USA: Boehringer Ingelheim Pharmaceuticals, Inc.; 2015. p. 10.
- http://www.abstractsonline.com/pp8/#!/4096/presentation/58477)
- Siegal DM, Curnutte JT, Connolly SJ, Lu G, Conley PB, Wiens BL, et al. Andexanet alfa for the reversal of factor Xa inhibitor activity. N Engl J Med 2015;373: 2413-2424.
- Lu G, DeGuzman FR, Hollenbach SJ, Karbarz MJ, Abe K, Lee G, et al. A specific antidote for reversal of anticoagulation by direct and indirect inhibitors of coagulation factor Xa. Nature Medicine 2013;19:446–51.
- Connolly SJ, Milling TJ, Jr., Eikelboom JW, Gibson CM, Curnutte JT, Gold A, et al. Andexanet alfa for acute major bleeding associated with factor xa inhibitors. N Engl J Med 2016;375:1131–41.
- Levy JH. Discontinuation and management of direct-acting anticoagulants for emergency procedures. Am J Emerg Med 2016;34:14–8.
- Brown KS, Zahir H, Grosso MA, Lanz HJ, Mercuri MF, Levy JH. Nonvitamin K antagonist oral anticoagulant activity: challenges in measurement and reversal. Crit Care 2016;20:273.
- Zahir H, Brown KS, Vandell AG, Desai M, Maa JF, Dishy V, et al. Edoxaban effects on bleeding following punch biopsy and reversal by a 4-factor prothrombin complex concentrate. Circulation 2015;131:82–90.
