Related Article:
Residual Neuromuscular Blockade: A Continuing Patient Safety Issue
| Editors’ Note: This issue contains a series of articles regarding the safe use of nondepolarizing neuromuscular blocking drugs. All anesthesia professionals should understand the importance of appropriately monitoring and reversing neuromuscular blockade. We believe that these articles will increase awareness, provide important educational information, and improve patient safety. |
The Anesthesia Patient Safety Foundation (APSF) believes that residual neuromuscular blockade in the postoperative period is a patient safety hazard that could be addressed partially by better and consistent use of our qualitative standard train-of-four (TOF) nerve stimulator monitors, but will ultimately require quantitative (objective TOF) monitoring along with traditional subjective observations to eliminate this problem completely.1-2 APSF and other anesthesia professionals believe that every patient receiving nondepolarizing neuromuscular blocking drugs (NMBDs) should have at least qualitative, and preferably quantitative monitoring of the intensity of neuromuscular blockade using a peripheral nerve stimulator during the intraoperative period and assessment of the pharmacologic antagonism of neuromuscular blockade and adequacy of neuromuscular function prior to tracheal extubation.1-10
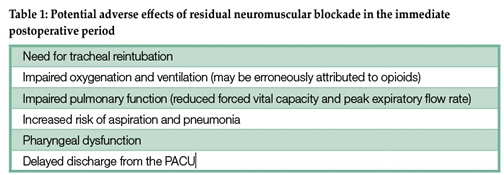
The peer review literature supports the conclusion that residual neuromuscular blockade in the immediate postoperative period is more common than appreciated. This weakness may contribute to adverse patient events (Table 1).3-9 Based on quantitative TOF monitoring as many as 40% of patients arriving in the PACU have evidence of residual neuromuscular blockade.4,9
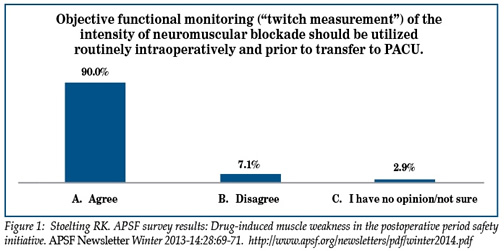
Despite the evidence in the peer review literature and a survey of anesthesia professionals in which 90% of respondents agreed that quantitative TOF monitoring should be used routinely for patients receiving nondepolarizing NMBDs prior to transfer to the PACU, quantitative measurements of drug-induced neuromuscular blockade and the adequacy of pharmacologic reversal have not been widely utilized by anesthesia professionals (Fig. 1).1 Achievement of the goal of routine qualitative or quantitative monitoring using a peripheral nerve stimulator is difficult when the daily experiences of anesthesia professionals do not predictably demonstrate the existence of a problem that may occur well after the anesthesia professional has turned over care to another health care professional.4 Universal adoption of quantitative monitoring is further impeded by the limited availability of easy-to-use, reliable monitoring technology. Many anesthesia professionals continue to rely on clinical signs (head lift, hand grip, negative inspiratory force, tidal volume) that are insensitive indicators of residual skeletal muscle weakness and applicable only to awake patients. Likewise, reliance on visual/tactile assessment of the TOF (low sensitivity to detect fade) to titrate the effects and assess the pharmacologic reversal of nondepolarizing NMBD is an insensitive and unreliable monitoring technique. Though double-burst stimulation (DBS) and fade with 100 Hz tetanic stimulation significantly improve the ability to detect residual neuromuscular blockade over single twitch or TOF monitoring or clinical signs, these modalities of assessing neuromuscular blockade are inferior to methods of quantitative monitoring such as acceleromyography.10
A recommendation for routine qualitative or quantitative monitoring of neuromuscular blockade with peripheral nerve stimulators as part of the “Standards for Basic Anesthetic Monitoring” has not been promulgated by any of the North American professional anesthesia associations (American Society of Anesthesiologists, American Association of Nurse Anesthetists, American Academy of Anesthesiologist Assistants, Canadian Anesthesiologists’ Society). To date, these anesthesia professional associations are either silent regarding monitoring neuromuscular blockade or limit their statements to (1) “monitor neuromuscular response” [no specific quantitative monitor mentioned] or (2) a “peripheral nerve stimulator should be available when patients receive neuromuscular blockers.”
In contrast, the 2015 “Recommendations for standards of monitoring during anaesthesia and recovery” published by the Association of Anaesthetists of Great Britain and Ireland (AAGBI) mandates that “a peripheral nerve stimulator must be used whenever neuromuscular blocking drugs are given.”9 These recommendations also list a peripheral nerve stimulator (if neuromuscular blocking drugs are used) as part of the “minimum monitoring for anaesthesia” along with pulse oximetry and capnography.9 This AAGBI mandate reflects the increasing recognition of the role of NMBDs in adverse postoperative pulmonary events.
In my opinion, there is no compelling reason to ignore this evidence-based patient safety issue and the obvious change in practice (qualitative, or preferably quantitative/objective monitoring with peripheral nerve stimulators to guide pharmacologic drug reversal) that would likely reduce the risk of potential adverse physiologic effects of lingering drug-induced muscle weakness in the early postoperative period.
What will it take for “North American” anesthesia professionals to accept the reality of this patient safety risk?
Why are “we” so “hesitant” to routinely use qualitative or quantitative assessments of neuromuscular function with peripheral nerve stimulators to guide both the administration and reversal of nondepolarizing NMBDs?
Would “we,” knowing what we know, or should know, regarding the facts relevant to residual weakness due to nondepolarizing NMBDs, expect, at a minimum, qualitative monitoring with peripheral nerve stimulators if we were the patient?
My guess is “we” would expect qualitative, and more likely, quantitative monitoring of neuromuscular blockade as part of our care!
It is time to “Do as I would expect, not as I do!”
Robert K. Stoelting, MD
President, APSF
References
- Stoelting RK. APSF survey results: Drug-induced muscle weakness in the postoperative period safety initiative. APSF Newsletter Winter 2013-14;28:69-71. Available at: https://www.apsf.org/newsletters/pdf/winter2014.pdf.
- Stoelting RK. Residual drug-induced muscle weakness in the postoperative period—a patient safety issue. ASA Newsletter 2015;79:64-65. Available at: http://www.asahq.org/search?q=February%202015%20ASA%20Newsletter.
- Brull SJ, Naguib M. What we know: Precise measurement leads to patient comfort and safety. Anesthesiology 2011;115:918–920.
- Todd MM, Hindman BJ, King BJ. The implementation of quantitative electromyographic neuromuscular monitoring in an academic anesthesia department. Anesth Analg 2014;119:323–331.
- Viby-Mogensen J, Claudius C. Evidence-based management of neuromuscular block. Anesth Analg 2010;111:1–2.
- Donati F. Neuromuscular monitoring: what evidence do we need to be convinced? Anesth Analg 2010;111:6–8.
- Kopman AF. Managing neuromuscular block: where are the guidelines? Anesth Analg 2010;111:9–10.
- Gopalaiah VK, Nair AP, Murthy HS, et al. Residual neuromuscular blockade affects postoperative pulmonary function. Anesthesiology 2012;117:1234-44.
- Checketts MR, Alladi R, Ferguson K, et al. Recommendations for standards of monitoring during anaesthesia and recovery 2015: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia 2015; Available at https://www.aagbi.org/sites/default/files/Standards%20of%
20monitoring%2020150812.pdf - Capron F, Fortier LP, Racine S, Donati F. Tactile fade detection with hand or wrist stimulation using train-of-four, double-burst stimulation, 50-hertz tetanus, 100-hertz tetanus, and acceleromyography. Anesth Analg 2006 May;102:1578–84.
