Anesthesia professionals are routinely involved in the transport of patients throughout the hospital (intrahospital transport). Studies on the outcomes of patients undergoing perioperative transport by anesthesia professionals are rare, as most literature involves nurses or other care providers and rarely focuses on the perioperative population. Thus, we must learn from reports published in critical care or emergency medicine. The incidence of intrahospital adverse events (ITAEs) during transport or within 24 hours of transport approaches 80% in some studies.1,2 The frequency of patients requiring medical intervention from ITAEs has been reported to range from 4 to 9%.2-4 Production pressure, reduction in support personnel, and increased patient acuity may heighten the risk of peri-operative transport.1,5 As such, now is the time to ask, “Is our approach to perioperative patient transport right and are we doing it safely?” We review the current literature to understand the incidence and contributing factors leading to ITAEs as well as practices from other areas that can be applied to our field.
The variability in the incidence of ITAEs may be partially attributed to the lack of consensus regarding what an adverse event entails during transport. It can be defined as “any unintended event or outcome, which may have or did reduce the safety margin for the patient.” 5 Or, it can be any observation that fell outside of some predefined threshold (e.g., hypotension with SBP < 100 mmHg, hypertension with SBP > 160 mmHg).6 A meta-analysis describing the incidence of ITAEs commented on the high heterogeneity among studies making it difficult to accurately report a range of frequencies.7 For instance, many studies did not clearly define an ITAE while others defined one based on author team consensus. Additionally, there was no method for distinguishing whether patient changes were indeed ITAEs or merely represent physiologic variability that just happened to occur during transport.
Despite the heterogeneity in the literature regarding the incidence and types of ITAEs, common themes prevail. ITAEs are often classified as respiratory, cardiovascular, neurological, and equipment related.7 Commonly reported individual events included hypertension, hypotension, arrythmias (including cardiac arrest), decreased arterial saturation, and agitation.7 Equipment-related problems included malfunction, accidental dislodgement of lines, tubes, and catheters, and empty oxygen cylinders. A recent multicenter prospective study reported similar findings.8 Among 102 ITAEs identified in the multicenter study, cardiac (30.3%), airway and/or respiratory (17.6%), neurologic (16.6%), and equipment problems (12.7%) were the most common.8 The association between the physiologic changes and transport itself was difficult to determine. Regardless, equipment-related adverse events continue to be prominent with some studies attributing over one-third of ITAEs to problems with tools and technology, including unreliable functioning of transport equipment and errant management of such equipment by health care providers.9
Patient transport may also subject anesthesia professionals to physical harm due to ergonomic factors. Transport stretchers or beds may weigh as little as 100 pounds up to as much as 700 pounds.10 Bed width and length may be challenging to maneuver while simultaneously managing an airway or performing an intervention during ITAE. Anesthesia professionals report a high rate of work-related musculoskeletal disorders with a large percentage reporting the need for analgesics while over 40% report sick leave associated with such injuries.11
Table 1: Adverse Events and Risk Factors Associated With Patient Transport.
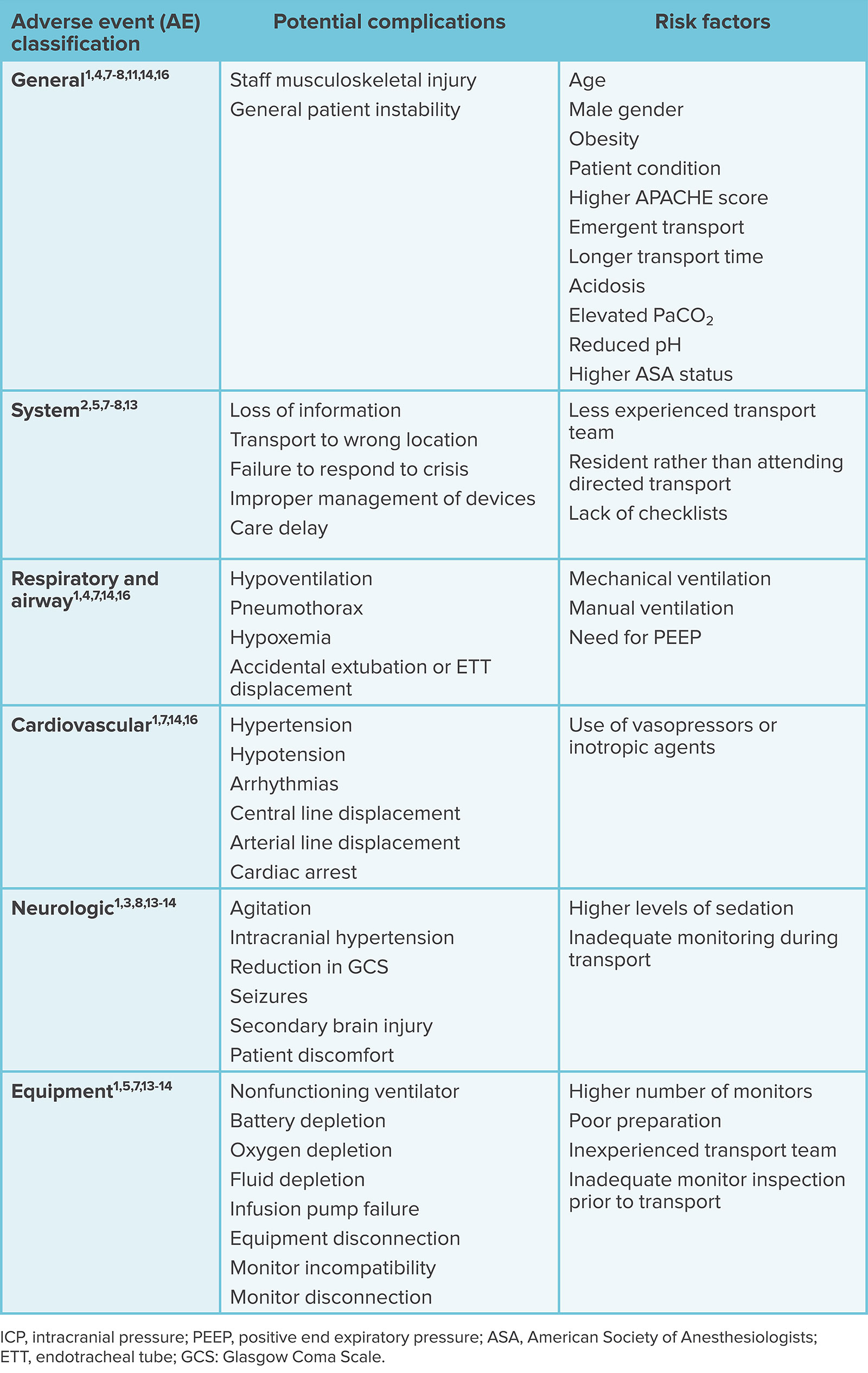
Numerous studies have evaluated risk factors for complications during transport (Table 1).1,4-7,2-14 Risk factors may be classified as patient-specific, equipment-related, or systematic. Patient-specific factors associated with higher rates of complications include higher severity of illness scores, older age, the need for pharmacologic support (specifically, sedative medications and/or vasopressors), mechanical ventilation (specifically, PEEP > 6 cm H2O), obesity, and compromised arterial oxygen saturation before transport.1,3-4,7,12,15 In general, the literature suggests that critically ill patients in particular are at increased risk for ITAEs. Equipment-related risk factors include the use of mechanical ventilation and increasing number of monitors utilized during transport.5,6,14 System or situational risk factors include longer duration of transport (> 60 minutes outside of the ICU), poor hand-off communication, urgent or emergency transport, staffing shortages, and the use of less experienced health care or transport providers.2,5,6,13,16,17 Factors not identified in studies but a subject of discussion are cluttered hallways and focus of a care provider on the act of physically moving a bed which may limit their ability to observe obstacles which threaten safe transport (Figure 1).
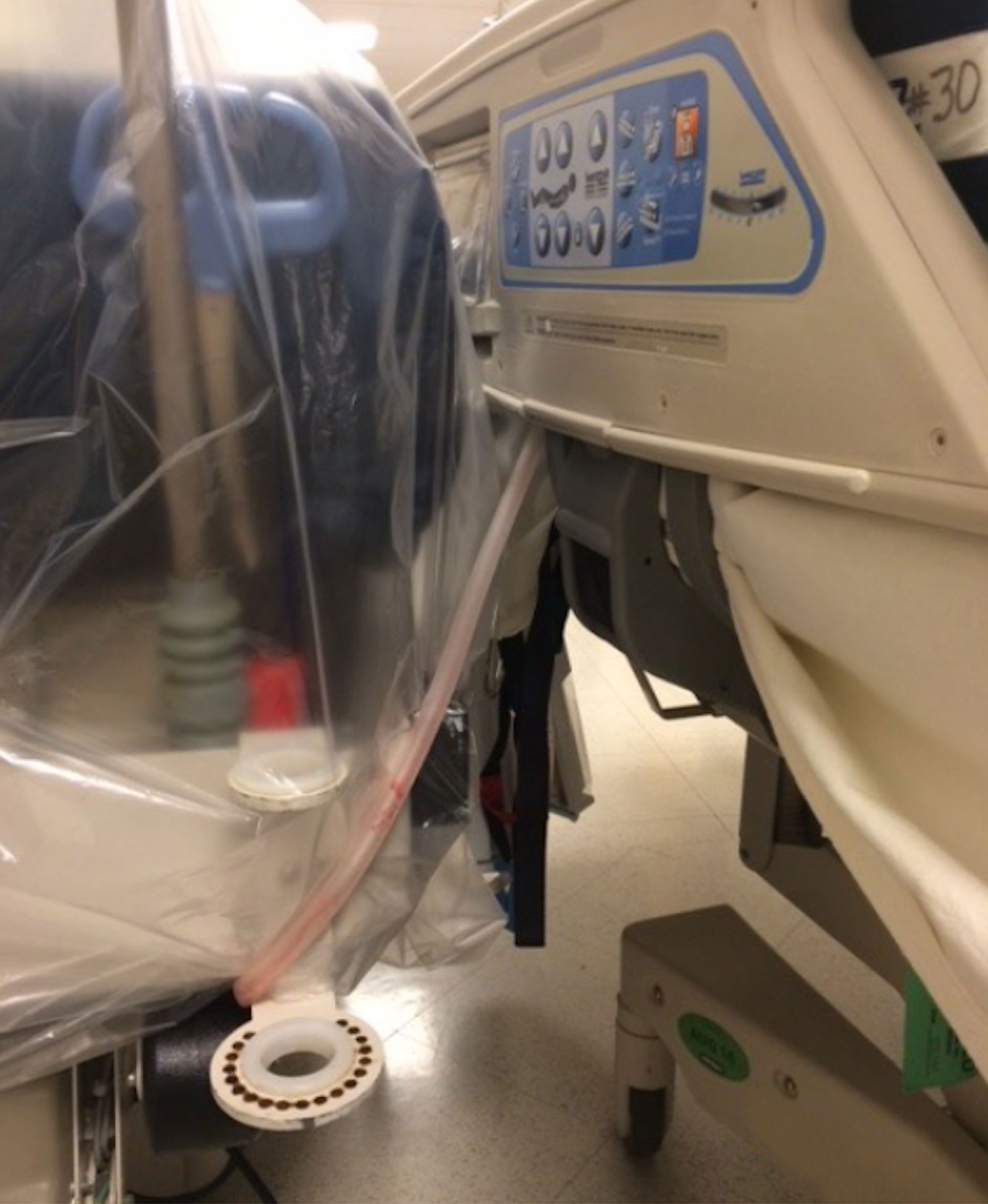
Figure 1: Example of unsafe environmental factors. A chest tube wrapped around a bed post in a cluttered hallway.
The American College of Critical Care Medicine and the Society of Critical Care Medicine have established guidelines for intrahospital transport of critically ill patients to and from the ICU, which provide a foundation for improving our perioperative practice.17 The SCCM guidelines focus on four critical components of transport: communication, personnel, equipment, and monitoring.17 Communication includes provider-to-provider handoff when the receiving location assumes management of the patient and conveys information to other disciplines such as respiratory care regarding the timing of transport and equipment required.17 In terms of personnel, the guidelines recommend a minimum of two people accompany a critically ill patient during transport. A provider with expertise in airway management and advanced cardiac life support is strongly recommended to accompany volatile patients. Basic monitors including blood pressure, pulse oximetry, and EKG should accompany every critically ill patient during transport without exception. The level of monitoring should not be reduced during transport. Medications necessary for resuscitation should be readily available. Equipment should be fully charged and capable of functioning for the entirety of the transport duration. The American Society of Anesthesiologists provides additional guidelines on the transport of patients from the operating room (OR) to the postanesthesia care unit (PACU).18 The ASA guidelines on PACU transport state that a patient who has received general anesthesia, regional anesthesia, or monitored anesthesia “shall be accompanied by a member of the anesthesia care team who is knowledgeable about the patient’s clinical condition.”18 During transport, the patient should be consistently assessed and treated with levels of monitoring and/or support that are suitable for the patient’s clinical condition based on the anesthesia professionals’ clinical judgment.18 Other actions that may limit adverse effects during transport include regular patient/equipment checks, meticulous patient preparation, correct use of protocols, and transport locations that are within easy reach.5,19,20 Some studies have also found reductions in ITAEs and increased compliance with guidelines by incorporating standardized transport checklists into their practice.21-22
Table 2: Perioperative Intrahospital Patient Transport Checklist
| System | Critical Points |
| Identification/ Information |
Identification bracket on patient |
| Chart with patient | |
| Necessary consents present | |
| Confirm ICU / PACU / OR prepared for patient | |
| Airway |
Endotracheal tube secured |
| Airway precautions necessary | |
| Manual resuscitator (Bag-valve-mask) present | |
| Emergency airway management equipment necessary /available | |
| Breathing |
Mode of delivery of oxygen confirmed |
| Oxygen supply adequate | |
| Transport ventilator charged/ functioning | |
| Patient on ventilator | |
| Circulation |
Intravenous line identified for resuscitation |
| Emergency medications necessary / available | |
| Infusion pumps and monitor adequately charged | |
| Hemodynamic alarms set | |
| Defibrillator necessary / present | |
| Neurologic |
Sedation / pain control adequate |
| Spinal precautions necessary | |
| Extras/Precautions |
Patient stable / safe for movement |
| Personal protective equipment present | |
| Lines, tubes, drains secured | |
| Rails raised | |
| Final |
Connect monitors |
| Plug in bed | |
| Perform comprehensive hand-off |
Perioperative transport of seriously ill patients should remain under the guidance of the anesthesia care team. As patient acuity, production pressure, and care volume continue to increase, anesthesia professionals must be proactive in efforts to increase transport safety for our patients while maintaining our well-being. We offer several recommendations that may help us achieve those goals:
- Patient assessment before transport should include the identification of risk factors associated with ITAEs.
- All anesthesia team members as well as others involved in patient movement should be educated on the potential harm of intrahospital transport and on proven practices that minimize these harms (e.g., guidelines, and the use of checklists during transport).
- The use of perioperative patient transport checklists may be beneficial to assure that patients are prepared, equipment is functioning with back-up power supply, records are present, and communication has occurred (Table 2). Such checklists should be used at initiation of transport, during hand-off at the receiving location, and upon return to the original location.
- Anesthesia professionals should participate in system design when patient transport is involved. Factors to consider are uncluttered hallways, easily maneuverable beds and stretchers, and team formation that allows the anesthesia professional to observe the patient and intervene without distraction while other team members assume primary responsibility for patient physical bed movement.
- Perioperative transport by anesthesia professionals should be promoted as an important focus of academic study.
Caroline Andrew, RN, MD, is a resident physician of anesthesiology, Massachusetts General Hospital, Boston, MA
Michael Fitzsimmons, MD, is an associate professor of anesthesiology at Harvard Medical School and staff anesthesiologist at Massachusetts General Hospital, Boston, MA
The authors have no conflicts of interest.
REFERENCES
- Jia L, Wang H, Gao Y, et al. High incidence of adverse events during intra-hospital transport of critically ill patients and new related risk factors: a prospective, multicenter study in China. Crit Care. 2016;20:12. PMID: 26781179.
- Papson JP, Russell KL, Taylor DM. Unexpected events during the intrahospital transport of critically ill patients. Acad Emerg Med. 2007;14:574–577. PMID: 17535981
- Nonami S, Kawakami D, Ito J, et al. Incidence of adverse events associated with the in-hospital transport of critically ill patients. Crit Care Explor. 2022;4:e0657. PMID: 35265855
- Lahner D, Nikolic A, Marhofer P, et al. Incidence of complications in intrahospital transport of critically ill patients–experience in an Austrian university hospital. Wien Klin Wochenschr. 2007;119:412–416. PMID: 17671822
- Beckmann U, Gillies DM, Berenholtz SM, et al. Incidents relating to the intra-hospital transfer of critically ill patients. An analysis of the reports submitted to the Australian Incident Monitoring Study in Intensive Care. Intens Care Med. 2004;30:1579–1585. PMID: 14991102
- Gillman L, Leslie G, Williams T, et al. Adverse events experienced while transferring the critically ill patient from the emergency department to the intensive care unit. Emerg Med J. 2006;23:858_661. PMID: 17057138
- Murata M, Nakagawa N, Kawasaki T, et al. Adverse events during intrahospital transport of critically ill patients: A systematic review and meta-analysis. Am J Emerg Med. 2022;52:13–19. PMID: 34861515
- Zirpe KG, Tiwari AM, Kulkarni AP, et al. Adverse events during intrahospital transport of critically ill patients: a multicenter, prospective, observational study (I-TOUCH Study). Indian J Crit Care Med. 2023;27:635–641. PMID: 37719359
- Bergman LM, Pettersson ME, Chaboyer WP, et al. Safety hazards during intrahospital transport: a prospective observational study. Crit Care Med. 2017;45:e1043–e1049. PMID: 28787292
- Vann MA, Katz JD. Physical hazards in the anesthesiologist’s workplace. ASA Monitor. 2019;83:16–18. https://pubs.asahq.org/monitor/article-abstract/83/12/16/108409/Physical-Hazards-in-the-Anesthesiologist-s?redirectedFrom=fulltext. Accessed December 3, 2024.
- Tolu S, Basaran B. Work-related musculoskeletal disorders in anesthesiologists: a cross-sectional study on prevalence and risk factors. Ann Med Res. 2019;26:1406–1414. https://annalsmedres.org/index.php/aomr/article/view/1258. Accessed December 3, 2024.
- Labaste F, Silva S, Serin-Moulin L, et al. Predictors of desaturation during patient transport to the postoperative anesthesia care unit: an observational study. J Clin Anesth. 2016;35:210–214. PMID: 27871524
- Veiga VC, Postalli NF, Alvarisa TK, et al. Adverse events during intrahospital transport of critically ill patients in a large hospital. Rev Bras Ter Intensiva. 2019;31:15–20. PMID: 30843950
- Parmentier-Decrucq E, Poissy J, Favory R, et al. Adverse events during intrahospital transport of critically ill patients: incidence and risk factors. Ann Intensive Care. 2013;3:10. PMID: 23587445
- Oliveira E, Marques A, Moinho N, Almeida V. Does the transportation of patients from the operating room to the post-anesthetic care unit should be done with supplemental oxygen? Eur J Anesth. 2012;29:222. https://journals.lww.com/ejanaesthesiology/Fulltext/2012/06001/Does_the_transportation_of_patients_from_the.737.aspx. Accessed December 12, 2024.
- Harish MM, Janarthanan S, Siddiqui SS, et al. Complications and benefits of intrahospital transport of adult Intensive Care Unit patients. Indian J Crit Care Med. 2016;20:448–452. PMID: 27630455
- Warren J, Fromm RE Jr, Orr RA, et al. Guidelines for the inter- and intrahospital transport of critically ill patients. Crit Care Med. 2004;32:256–262. PMID: 14707589
- Committee on Standards and Practice Parameters. Standards for Postanesthesia Care. American Society of Anesthesiologists. https://www.asahq.org/standards-and-practice-parameters/standards-for-postanesthesia-care. Published October 2004. Updated October 2019. Accessed December 12, 2024.
- Lin SJ, Tsan CY, Su MY, et al. Improving patient safety during intrahospital transportation of mechanically ventilated patients with critical illness. BMJ Open Qual. 2020;9:e000698. PMID: 32317274
- Fanara B, Manzon C, Barbot O, et al. Recommendations for the intra-hospital transport of critically ill patients. Crit Care 2010;14:R87. PMID: 20470381
- Choi HK, Shin SD, Ro YS, et al. A before- and after-intervention trial for reducing unexpected events during the intrahospital transport of emergency patients. Am J Emerg Med. 2012;30:1433–1440. doi.org/10.1016/j.ajem.2011.10.027
- Venn AM, Sotomayor CA, Godambe SA, et al. Implementation of an intrahospital transport checklist for emergency department admissions to intensive care. Pediatr Qual Saf. 2021;6:e426. PMID: 34235354.
