PREVALENCE OF MEDICAL MISINFORMATION
Medical misinformation can have a profound impact on perioperative patient safety. With users numbering in the billions, platforms such as Facebook, Instagram, TikTok, X (formerly Twitter), Snapchat, Pinterest, Reddit, Messenger, and YouTube command an ever-increasing share of the public’s time, attention, and dependence.1 Consequently, they have also become primary sources of information for politics, sports, general knowledge, and news for the general public. Statistics published by Pew Research in 2022 show that adults under the age of 30 actually trust information from social media almost as much as national news outlets, and in 2023, half of US adults get news at least some of the time from social media.2,3
The relationship between medical care and information on the internet has been fraught since the early days of the internet, predating the more recent increase of medical misinformation. According to the United States Office of the Surgeon General, medical misinformation is “information that is false, inaccurate, or misleading according to the best available evidence at the time.”4 The term “cyberchondria” was first coined more than two decades ago to describe heightened distress or anxiety caused by review of medical information on the internet.5 One framework to explain the etiology of this distress suggests that patients with pre-existing anxiety seek out additional information on the internet for reassurance. Given the possibly unreliable nature of this information, alarm and surprise may follow, causing some patients or family members to find reassurance, whereas others do not. Those that fail to find reassurance seek out even more online health research, which often produces more anxiety and a self-perpetuating cycle takes hold.6
Misinformation can affect understanding of public health concerns, as was seen in the recent COVID pandemic when concerns were expressed regarding social distancing, mask mandates, and vaccination.7,8 Perioperative medicine is no less affected. Patients presenting for labor pain may hesitate to consent for an epidural for analgesia if they consumed medical misinformation regarding potential side effects or complications. In 2022, a scoping review to assess the most common patient-reported barriers regarding epidural use in labor found that patients feared maternal side effects, fetal complications, prolonged labor, and paralysis, among other concerns.9
A similar situation may present when discussing peripheral nerve block techniques for postoperative analgesia, especially if patients found medical misinformation on public health forums. These forums are often not moderated, and the personal anecdotes on these forums can influence patients, both positively and negatively. For example, there was significant public concern regarding peripheral nerve blocks following the lawsuit filed by professional American football player Sharrif Floyd against renowned orthopedic surgeon James Andrews, MD, and his colleagues. Floyd attributed his career-ending injuries to both his knee procedure and the nerve block that followed, with possible embellishments or sensationalism of the story causing panic and fear among future patients needing orthopedic surgery.10 There are reliable sources of information, such as the in-depth analysis provided by journalist Michael McCann in Sports Illustrated, as well as the text of the legal complaint.11 However, there are also sources of potential misinformation, such as a Reddit page featuring a robust discussion of theories regarding the case, and an X/Twitter post that also featured speculation and comments that may appear knowledge-based for members of the general public.12
Sensationalism in news stories may even cause patient fear and hesitancy when discussing medication selection (Table 1). For example, following the death of Michael Jackson, patients became very concerned with the administration of propofol, despite its high safety profile when administered by a trained anesthesia professional. Recent negative coverage regarding fentanyl and its use in illicit drugs may cause undue panic, as well.
Table 1: Sampling of Categories of Medical Misinformation in Anesthesiology With Associated Questions/Statements From Patients or Family Members.
| Common misinformation about anesthesia | Sample patient/family concerns |
| Intraoperative awareness |
“Will I wake up during surgery?” |
| “Please don’t let me wake up during surgery!” | |
| “I saw a movie once, and they were awake during the surgery.” | |
| Medications given are very dangerous (propofol, fentanyl, etc.) |
“Are you going to give me that fentanyl stuff?” |
| “I’ve heard you use that stuff that killed Michael Jackson.” | |
| “Don’t use that on me, are you trying to make me an addict?” | |
| “Matthew Perry died from ketamine. Don’t give me that!” | |
| Anesthesia changes postoperative behavior (e.g., truth serum, seizures) |
“Don’t let me say anything stupid in there.” |
| “Can you get seizures from anesthesia?” | |
| Epidurals cause permanent damage |
“Don’t those things paralyze you?” |
| “I know you can get bad back pain from those things.” | |
| Nerve blocks do not work |
“You just want me to have that so I don’t get any pain meds.” |
| “I’ve heard those things never work and can really hurt!” | |
| Sedation is safer versus general anesthesia |
“I know sedation is so much safer—can I have that instead?” |
| “I’ve heard people die undergoing general anesthesia all the time.” | |
| Understanding how anesthesia works |
“You don’t even know how that stuff works?” |
| “How do you give medication when you don’t know what it does?” |
THE IMPACT OF MEDICAL MISINFORMATION ON PATIENT SAFETY
Medical misinformation may negatively impact patient safety throughout the perioperative period. The detrimental effects of such misinformation may be grouped into three categories: fear and anxiety, delay of treatment, and avoidance of treatment (Figure 1). Fear and anxiety may cause psychological distress, which can lead to perseveration on concerns, gastrointestinal upset, sleep loss, and more. In addition, such negative feelings may provoke physiologic sequelae such as blood pressure and heart rate changes. These physical and psychological effects can further lead to patient noncompliance.
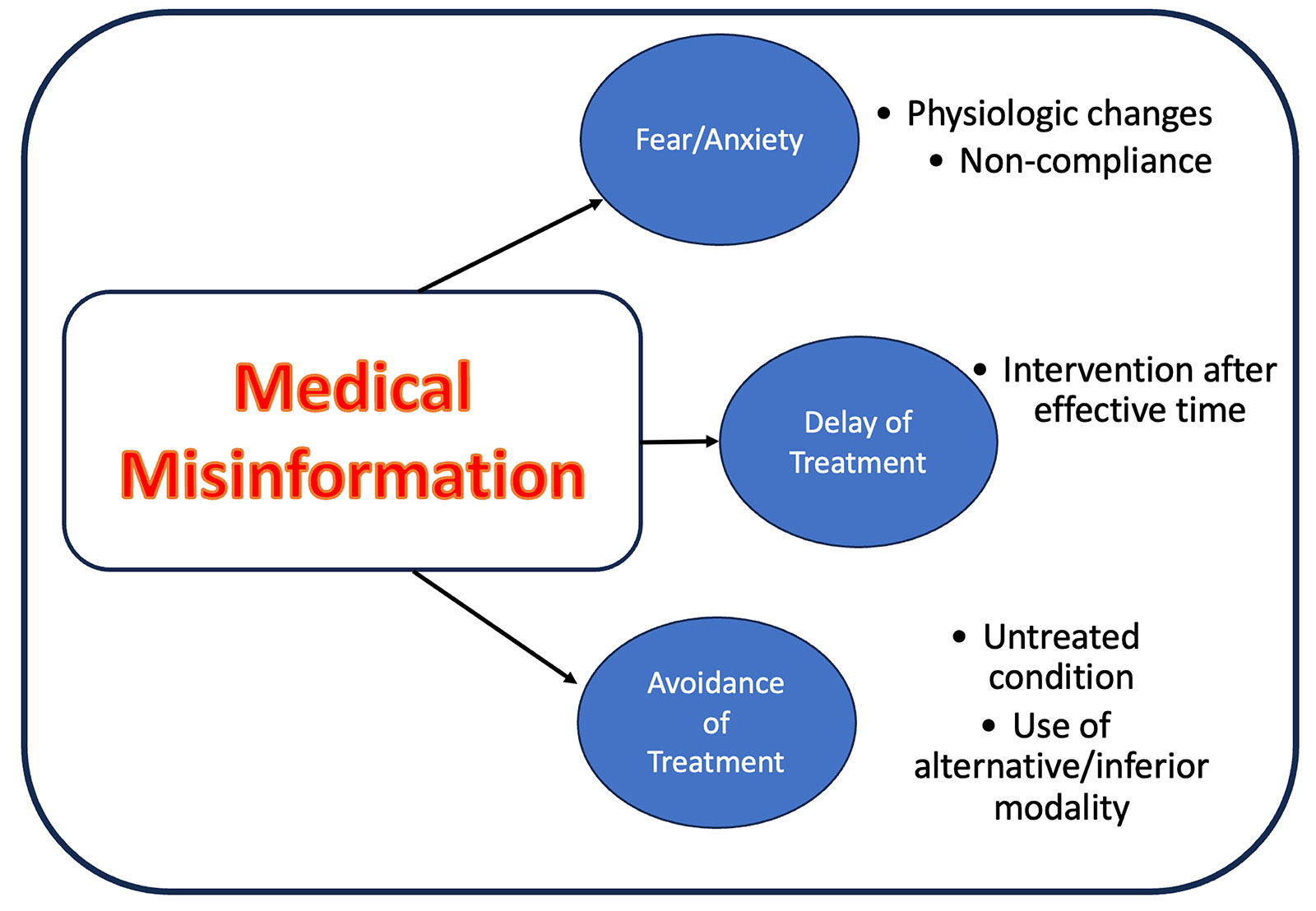
Figure 1: Potential consequences of medical misinformation in anesthesiology.
Delays in treatment may also occur. For example, if a patient initially refuses neuraxial anesthesia due to fear of labor epidurals, this may lead to last-minute epidural analgesia requests as the baby is about to deliver, leading to a rushed provider placing an epidural on an actively contracting patient. It may lead to increased risk in complicated pregnancies, such as those in patients suffering from preeclampsia. Although use of epidurals to control blood pressure in preeclampsia is controversial, early epidural placement is encouraged in parturients with preeclampsia to minimize the need for general anesthesia in the event of an emergent cesarean delivery.13,14 Peripartum safety may therefore be compromised by the introduction of medical misinformation if a delay precludes safe and efficacious epidural use.
The final category is avoidance of treatment. This may affect not only the anesthetic plan developed by the care team, but also may affect a patient’s clinical course. For example, a patient with pulmonary comorbidities may not receive the most optimal perioperative care if they refuse to receive a regional anesthetic nerve block due to misinformation about the risk of paralysis or local anesthetic toxicity. The patient’s pain may instead be treated with opioids, resulting in the potential for respiratory depression and airway obstruction and possible downstream complications and delayed discharge. Another example is the patient that may have benefited from a labor epidural, but instead encounters severe labor pain that remains untreated and may even develop acute stress, or even post-traumatic stress disorder, secondary to their experience during peripartum period.15
HOW TO MINIMIZE THE IMPACT OF MEDICAL MISINFORMATION ON PATIENT SAFETY
What can be done to combat misinformation and to ensure that it does not impact patient safety? Awareness among anesthesia professionals must be increased. Patients who ask such questions as “Will I wake up during surgery” or “Don’t epidurals mess up your back forever?” may be heavily influenced by seeing a video on TikTok or reading a post on Facebook. A friend or family member may have sent them an anxiety-producing video from YouTube in anticipation of their planned surgical procedure, leading to increased concern. Clinicians must be aware that these comments or questions are not seemingly random or fleeting thoughts, but may be deeply rooted in anxiety provoked by misinformation. It is important to consider that the genesis of these questions is fear-based, and though it may arise from incorrect information or irrational concerns, the patient will continue to suffer anxiety if these questions are not answered in a compassionate and thoughtful manner.
After facilitating awareness of this potential phenomenon, it is important to demonstrate empathy for a patient and not to be dismissive. Statements should be used such as “I’m sure this process can be very scary” or “I understand you have some concerns; let’s discuss them further.” Validation of one’s fear, instead of dismissing their concerns as unreasonable, is a valuable first step to attenuating fear and establishing trust between the clinician and patient. Building trust with a patient during the preoperative evaluation is always an important aspect of a focused and targeted evaluation, but it gains new importance when the patient has anxiety due to misinformation.
Upon taking action to build trust, the anesthesiology professional should seek to carefully inquire regarding the patient’s misinformation and to use facts to reassure the patient and their family. However, it is important to remember the importance of patient autonomy. One should not attempt to aggressively persuade a patient, especially for an elective intervention such as a regional anesthetic. Often, this will not only fail to persuade a patient, but may reinforce negative perceptions regarding health care professionals. Nonetheless, empathy, patience, and a willingness to listen to a patient’s concerns are often enough to adequately address the concerns regarding anesthetic care that have been intensified by fear and anxiety due to misinformation.
Unsurprisingly, regulatory agencies and public health organizations have recognized the potentially disastrous impact on patient safety related to medical misinformation. In 2021, the United States Surgeon General released an “Advisory on Building a Healthy Information Environment.”16 This valuable resource offers further recommendations for health care professionals regarding false or misleading data. The recommendations include such items as proactively engaging with patients and the public regarding health information, using empathy, and accessible language. Furthermore, health care professionals are encouraged to use technology and electronic communications platforms to share accurate health information with the public at large. Finally, partnerships with community and local officials are encouraged to help develop localized messaging to address health care concerns in an accurate manner.
Verification of medical information is a complex task, especially for patients and family members who lack medical training. It is important for medical professionals who interact with a patient in the preoperative period to refer discussions regarding anesthesia (especially the choice of techniques and associated risks/benefits) to the anesthesia professional who will take care of the patient. Confusion often results when an unqualified person makes suggestions about possible techniques and medications, as well as their associated potential side effects. The preoperative evaluation and consultation with the designated anesthesia professional will be the single most important source of relevant information for a patient and their family. However, the impetus to consume information regarding anesthesia prior to a procedure is understandable, and patients should be directed (if necessary) to trusted and reputable sources of medical information on the internet, such as the APSF Patient Guide to Anesthesia and Surgery, that are designed for nonclinicians.17
It is important for anesthesia professionals to remember that medical misinformation may negatively affect patients and their families. Members of the public may seek out information prior to a surgical procedure or be sent information by loved ones. That information may be incorrect or sensationalized, thus affecting a patient’s perceptions regarding anesthetic care. Utilizing empathy, patience, and facts, one may work to address medical misinformation to prevent fear and anxiety, delayed treatment, or the avoidance of appropriate medical care.
George Tewfik is an associate professor of anesthesiology at Rutgers New Jersey Medical School in Newark, NJ.
Raymond Malapero is a clinical assistant professor of anesthesiology at Rutgers New Jersey Medical School in Newark, NJ, and is the vice chair of anesthesiology at Jersey Shore University Medical Center in Neptune, NJ.
The authors have no conflicts of interest.
REFERENCES
- Statista. Number of social media users worldwide from 2017 to 2027. https://www.statista.com/statistics/278414/number-of-worldwide-social-network-users/. Accessed December 12, 2024.
- Center PR. Social Media and News Fact Sheet. https://www.pewresearch.org/journalism/fact-sheet/social-media-and-news-fact-sheet/. Accessed December 12, 2024.
- Liedke JaG, Jeffrey. U.S. adults under 30 now trust information from social media almost as much as from national news outlets. Pew Research Center.
https://www.pewresearch.org short-reads/
2022/10/27/u-s-adults-under-30-now-trust-information-from-social-media-almost-as-much-as-from-national-news-outlets/. Accessed December 12, 2024. - Office of the Surgeon General of the US. Health Misinformation. https://www.hhs.gov/surgeongeneral/priorities/health-misinformation/index.html. Accessed December 12, 2024.
- Starcevic V, Berle D, Arnáez S. Recent insights into cyberchondria. Curr Psychiatry Rep. 2020;22:56. PMID: 32852626.
- Starcevic V, Berle D. Cyberchondria: towards a better understanding of excessive health-related Internet use. Expert Rev Neurother. 2013;13:205–213. PMID: 23368807.
- Clemente-Suárez VJ, Navarro-Jiménez E, Simón-Sanjurjo JA, et al. Mis-dis information in COVID-19 health crisis: a narrative review. Int J Environ Res Public Health. 2022;19:5321. PMID: 35564714.
- Zhao S, Hu S, Zhou X, et al. The prevalence, features, influencing factors, and solutions for COVID-19 vaccine misinformation: systematic review. JMIR Public Health Surveill. 2023;9:e40201. PMID: 36469911.
- Kirubarajan A, Schulman H, Ajay A, et al. Patient-reported barriers and facilitators to epidural use in labour: a scoping review. Can J Anaesth. 2022;69:1430–1431. PMID: 36131065.
- McCann M. A deep dive Into Sharrif Floyd’s $180 million lawsuit against Dr. James Andrews. https://www.si.com/nfl/2018/11/07minnesota-vikings-sharrif-floyds-1
80-million-lawsuit-against-dr-james-andrews. Accessed December 12, 2024. - Sharrif K. Floyd, individually and as assignee of The Andrews Institute Ambulatory Surgery Center, LLC, Plaintiff v. ENDURANCE AMERICAN SPECIALTY INSURANCE COMPANY, INC., et al., Defendants.: United States District Court, N.D. Florida, Gainesville Division.; 2023.
- Breer A. Former Vikings DE Sharrif Floyd filing lawsuit against Dr. James Andrews. https://x.com/AlbertBreer/status/1059624814028210176. November 5, 2018. Accessed December 12, 2024.
- Henke VG, Bateman BT, Leffert LR. Focused review: spinal anesthesia in severe preeclampsia. Anesth Analg. 2013;117:686–693. PMID: 23868886.
- Patel P, Desai P, Gajjar F. Labor epidural analgesia in pre-eclampsia: a prospective study. J Obstet Gynaecol Res. 2005;31:291–295. PMID: 16018774.
- Simkin P. Pain, suffering, and trauma in labor and prevention of subsequent posttraumatic stress disorder. J Perinat Educ. 2011;20:166–176. PMID: 22654466.
- Murthy VHMD, M.B.A. Vice Admiral, U.S. Public Health Service Surgeon General of the United States. Confronting health misinformation: the U.S. Surgeon General’s advisory on building a healthy Information environment. U.S. Public Health Service, 2021. PMID: 34283416.
- APSF. Patient guide to anesthesia & surgery. https://www.apsf.org/patient-guide/. Accessed December 12, 2024.

I find it disconcerting that the authors reference “disinformation” in the context of the COVID-19 pandemic as an authoritative example. We now know, that much of the “disinformation” at that time is actually true: a face mask made out of a t-shirt (or even an ear loop mask!) will not stop viral spread, the COVID-19 mRNA vaccines do not abolish viral transmission, and the virus likely did escape from a laboratory in China.
There is a tendency towards hubris in medicine – how do we avoid including our own biases in our estimation of what is “misinformation?”