Over the past decade, sodium-glucose cotransporter-2 inhibitors (SGLT2i) have been well established as excellent therapeutic agents for the management of type 2 diabetes mellitus (T2DM).1 Several randomized controlled trials (EMPEROR and CANVAS) have further established that SGLT2i demonstrate additional benefits in heart failure and chronic kidney disease, leading to their increased prevalence in the perioperative setting.2-4 However, there has been growing concern regarding euglycemic ketoacidosis, an uncommon but life-threatening side effect associated with SGLT2i use.1 SGLT2i inhibit glucose reabsorption in the proximal convoluted tubule resulting in glycosuria and reductions in serum glucose levels without an increase in insulin levels. Additionally, glucagon production can be stimulated resulting in lipolysis, ketoacid production, and, rarely, anion gap metabolic acidosis.5 Since several perioperative factors (e.g., fasting state, increase in stress hormones) can exacerbate this risk, anesthesia professionals must carefully consider the risk of perioperative SGLT2i-associated ketoacidosis.
REVIEW OF CURRENT RECOMMENDATIONS AND CHALLENGES
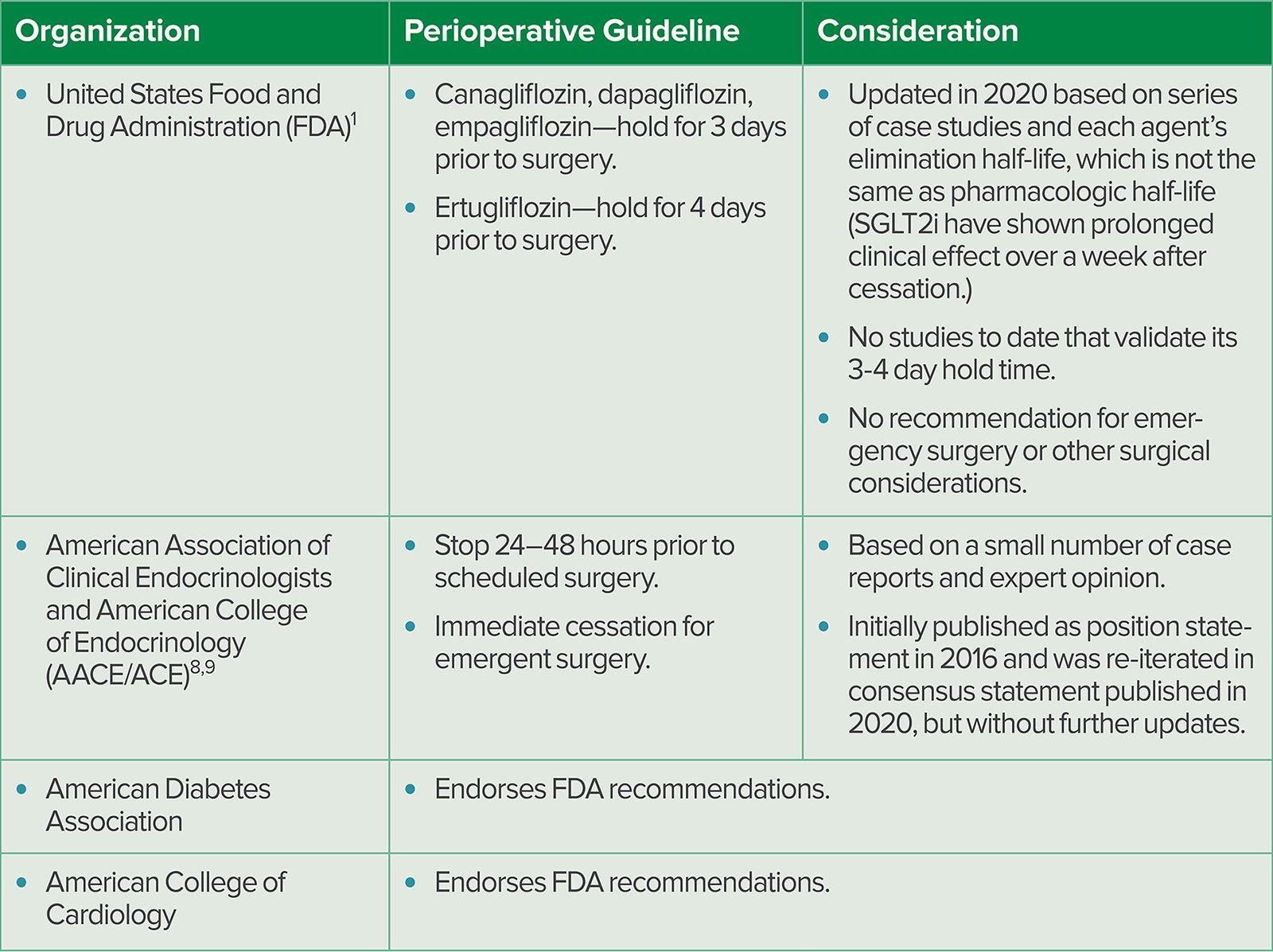
Currently, there is no consensus on perioperative management of SGLT2i and many published recommendations are outdated or based on limited data (Table 1). In 2020, an article in Anesthesiology recommended continuing SGLT2i for ambulatory surgery but stopping on the morning of surgery.6 However, these recommendations were extrapolated from expert opinions. In addition, they were published before United States Food and Drug Administrative (FDA) updated its recommendation to stop SGLT2i at least 3–4 days before all scheduled surgery. The FDA’s current recommendations also appear to be based on limited case reports and the elimination half-life of SGLT2i.1 In 2023, the validity of the FDA recommendations were evaluated by reviewing 99 reported cases of SGLT2i associated diabetic ketoacidosis; no cases were found in patients who held SGLT2i for longer than 3 days.7 Despite this being the largest systematic review to date on the subject, only 58.6% of the reviewed cases discontinued SGLT2i preoperatively, making the study further underpowered, and none of the reviewed cases discontinued SGLT2i for more than 2 days preoperatively. Despite a lack of validity, the FDA’s recommendation has been adopted by several organizations. Other individual institutions have published their own recommendations, but these are still based on limited case reports and do not demonstrate consensus on hold times for SGLT2i.8-10
Table 1: Summary of Current Notable Recommendations on Perioperative SGLT2i Use.
Several factors contribute to the current lack of evidence for perioperative management of SGLT2i. The most concerning factor is that, due to its atypical presentation, SGLT2i-associated euglycemic ketoacidosis is underreported, which makes it challenging to understand its prevalence and impact on a patient’s perioperative outcome.11 In fact, outside the perioperative setting, two large meta-analyses assessing 82 randomized controlled trials demonstrated that SGLT2i are not significantly associated with a higher risk of diabetic ketoacidosis compared to other hypoglycemic agents.12,13 Position statements from the American Association of Clinical Endocrinologists and American College of Endocrinology also suggest that the risk of diabetic ketoacidosis associated with SGLT2i is no greater than the low levels occurring in the general diabetes population.8 However, neither the meta-analyses nor position statements specifically comment on the risk of euglycemic ketoacidosis, which is marked by a different clinical presentation, diagnostic criteria, and occurrence rate. The question remains: what makes SGLT2i administration an exceptional risk factor for euglycemic ketoacidosis compared to other hypoglycemic agents during the perioperative period? Are there other perioperative factors that affect the risk of SGLT2i- associated euglycemic ketoacidosis? Several sources repeatedly comment that these critical questions are yet to be answered, which impedes the development of evidence-based perioperative guidelines for SGLT2i.
RECENT UPDATES ON PERIOPERATIVE SGLT2I USE
Based on an updated review of current literature, there are new findings that elucidate the prevalence and impact of perioperative SGLT2i-associated diabetic ketoacidosis. In 2022, the first and largest population-based study examining the incidence rate of SGLT2i-associated postoperative diabetic ketoacidosis was published.14 The incidence of postoperative diabetic ketoacidosis within 30 days postoperatively was six times higher in SGLT2i users compared to nonusers, which is much higher than previously suspected. SGLT2i users who developed diabetic ketoacidosis postoperatively had higher rates of complications (e.g., need for mechanical ventilation, infection, longer hospital stay) and overall increased mortality. This is the first study to establish SGLT2i as an independent risk factor for developing postoperative diabetic ketoacidosis.
However, this population study did not have uniform diagnostic criteria for diabetic ketoacidosis and did not clarify which of them, if any, were euglycemic at presentation. This is concerning since SGLT2i can cause prolonged glycosuria and ketonemia up to 9–10 days after cessation, which can confound the diagnosis.15 In fact, a 2023 single-institution retrospective analysis showed that all patients on SGLT2i, after average preoperative hold time of 1.5 days, developed some degree of ketoacidosis with mean increase in anion gap from 12.6 mmol/L preoperatively to 13.4 mmol/L postoperatively.16 These findings suggest that diagnosis of clinically significant ketoacidosis is a complex clinical consideration of not just pertinent laboratory values, but also clinical symptoms and presenting circumstances. Without clear diagnostic criteria differentiating the types of ketoacidosis, we may not understand the true incidence and impact of SGLT2i-associated euglycemic ketoacidosis, which continues to hinder the development of evidence-based perioperative SGLT2i guidelines.
PRACTICE CONSIDERATIONS AND RECOMMENDATIONS
There are several perioperative factors that should be considered when assessing the risk of SGLT2i-associated diabetic ketoacidosis (Table 2). Advanced T2DM (HgbA1c >8%) was recently reported to increase the risk by 3.1-fold.14 Emergent surgery, which was previously suggested as a risk factor given its inherent stress and urgency, was also recently reported to increase the risk by 24.5-fold.14 Bariatric surgery has long been considered a risk factor as perioperative SGLT2i-associated euglycemic ketoacidosis was first reported in bariatric patients, thought due to postoperative dietary changes as well as complications.7,11 This concern can be expanded to consider adequate postoperative nutritional intake (to overcome postoperative catabolic state) as an indicator for when to resume SGLT2i. Such a complex variety of factors should be incorporated when developing a guideline to manage patients on SGLT2i. For example, the University of Pennsylvania recently published a comprehensive single-center guideline incorporating factors such as anticipated procedure duration, anesthesia type, preoperative HgbA1c and glucose and basic metabolic panel, and underlying patient comorbidities to better identify which patients may be at high risk of perioperative SGLT2i-associated euglycemic ketoacidosis.17 While this guideline still endorses the FDA recommendation for preoperative SGLT2i cessation and needs further evidence for optimization, this is the first published approach to developing an algorithm to guide the management of high-risk euglycemic ketoacidosis cases for anesthesia providers taking care of patients on SGLT2i.
Table 2: Factors That Can Increase the Risk of Perioperative SGLT2i-Associated Euglycemic Ketoacidosis.
| Underlying comorbidities | |
| Female sex | Suggested based on case review.7 |
| Advanced or poorly controlled T2DM | Previously suggested as an independent factor.7,19 Recently, HgbA1c >8% reported to cause 3.1-fold increased risk.14 |
| Liver disease | Suggested as liver function is critical in glucose metabolism.19 |
| Concomitant insulin use | Recently reported to cause 2.8-fold increased risk.14 |
| Obesity | Suggested due to ketosis.7 |
| Surgical type | |
| Emergency | Previously suggested as an independent factor associated with as much as 25% of SGLT2-associated DKA.7,16 Recently reported to cause 24.5-fold increased risk.14 |
| Bariatric | Supported by several systematic reviews as a prominent factor due to its postoperative nutrition management.7,11 |
| Cardiac | Suggested through several case reports.16 |
| Other perioperative considerations | |
| Pre- and Postoperative hypovolemia | Suggested as it can mask the usual hyperglycemia induced polyuria.11 |
| Postoperative nutrition | Supported by current guidelines, reviews and meta-analyses; inadequate nutrition can worsen postoperative catabolic state and worsen metabolic complications.19 |
| Infection/sepsis | Suggested as it can impair adequate glycemic control and cause physiological stress.7,11 |
| Glucocorticoid use | Suggested as it can promote hyperglycemia and insulin resistance.11 |
| T2DM: Type 2 Diabetes Mellitus; DKA: Diabetic Ketoacidosis | |
Finally, it is important to highlight that for certain patients, SGLT2i cessation in the perioperative setting may be more harmful. At the end of EMPEROR trials that demonstrated cardioprotective benefit of empagliflozin, the patients who were prospectively withdrawn from treatment had increased risk of cardiovascular death and hospitalization for heart failure within 30 days of discontinuation back to pretreatment baseline.18 Given the rapid reversal of the cardioprotective benefits of SGLT2i, some advocate for early detection and treatment of ketoacidosis (e.g., intraoperative lab monitoring for acidosis and insulin infusion use) rather than perioperative discontinuation of SGLT2i in heart failure patients.19,20 There also has never been a case of euglycemic ketoacidosis in patients taking SGLT2i for cardiorenal indications in the absence of T2DM, so SGLT2i should be continued in this population.17
We suggest a perioperative algorithm for patients on SGLT2i (Figure 1). Given the lack of evidence in current literature, this algorithm may not apply to every case. However, we highlight the most significant perioperative considerations supported by current data, such as emergent procedures and other confounding risk factors for diabetic ketoacidosis.7,11,14,16,19 For emergent or urgent procedures, we recommend proceeding with surgery with close perioperative monitoring for acidosis and early initiation of insulin infusion, as the risk of delaying surgery may outweigh the risk of diabetic ketoacidosis. While data are lacking, the current FDA and other institutional guidelines suggest holding SGLT2i for all scheduled surgeries, including outpatient procedures with expected rapid return to preoperative state. 1,8,9 Therefore, for elective procedures, if the patient is considered high risk, we recommend rescheduling surgery, but if the patient is considered low risk, we recommend assessing other patient and surgical factors.17 For non-diabetic patients taking SGLT2i for heart failure or cardiorenal protection, we do not believe this algorithm applies; based on current data, they should continue SGLT2i and are considered at low risk for diabetic ketoacidosis. However, depending on other confounding risk factors, they too may require close perioperative monitoring for acidosis.
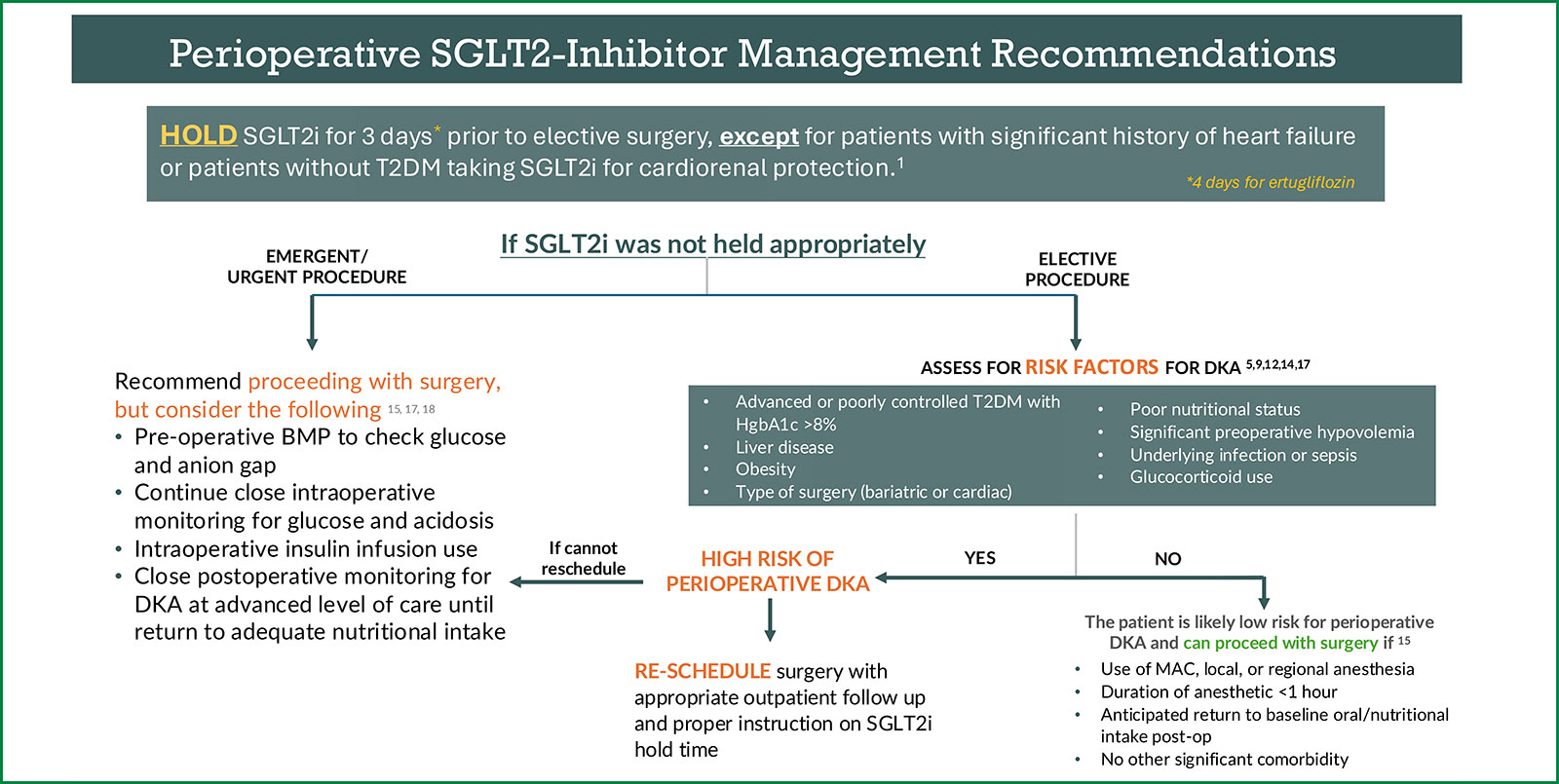
Figure 1: Recommendations for perioperative management of SGLT2i. Management pathways are influenced by the urgency of surgery and other significant patient or surgical factors that may increase risk of perioperative diabetic ketoacidosis. This algorithm does not apply to nondiabetic patients taking SGLT2i for heart failure or cardiorenal protection, as data suggest they should continue SGLT2i. Note that there are no Class 1 evidence for the perioperative management of SGLT2i. SGLT2i: Sodium-Glucose Cotransporter-2 Inhibitor; BMP: Basic Metabolic Panel; T2DM: Type 2 Diabetes Mellitus; DKA: Diabetic Ketoacidosis; MAC: Monitored Anesthesia Care.
In summary, we believe that SGLT2i pose an increased risk for diabetic ketoacidosis and other morbidities in the perioperative setting. However, the optimal preoperative hold time for SGLT2i and how cases should be handled if the hold time is not met remains controversial. The latter is particularly important for anesthesia professionals as many patients currently do not adhere to a universal hold time. While further research is needed, we encourage clinicians to consider the currently reported risk factors, along with other patient and surgical factors, to risk-stratify and individualize the management of patients taking SGLT2i, from case cancellation consideration to enhanced postoperative monitoring.
Soyun M. Hwang is an assistant professor of anesthesiology and critical care, Mayo Clinic, Rochester, MN.
Arney S. Abcejo is an associate professor of anesthesiology, Mayo Clinic, Rochester, MN.
Adam K. Jacob is a professor of anesthesiology, Mayo Clinic, Rochester, MN.
Jesse M. Raiten is a professor of anesthesiology and critical care, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA.
Manpreet S. Mundi is a professor of medicine in the Division of Endocrinology, Diabetes, Metabolism and Nutrition, Mayo Clinic, Rochester, MN.
The authors have no conflicts of interest.
REFERENCES
- FDA Drug Safety Communication. FDA revises labels of SGLT2 inhibitors for diabetes to include warnings about too much acid in the blood and serious urinary tract infections. Updated March 16, 2022. Available at: https://www.fda.gov/drugs/drug-safety-and-availability/fda-revises-labels-sglt2-inhibitors-diabetes-include-warnings-about-too-much-acid-blood-and-serious. Accessed August 5, 2024.
- Peacock SC, Lovshin JA. Sodium-glucose cotransporter-2 inhibitors in the perioperative setting. Can J Anesth. 2018;65:143–147. PMID: 29159514.
- Anker SD, Butler J, Filippatos G, et al. Empagliflozin in heart failure with a preserved ejection fraction. New Engl J Med. 2021;385:1451–1461. PMID: 34449189.
- Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. New Engl J Med. 2017;377:644–657. PMID: 28605608.
- Kumar S, Bhavnani SP, Goyal P, et al. Preoperative cessation of SGLT2i. American College of Cardiology Expert Analysis. Published October 7, 2022. Available at: https://www.acc.org/Latest-in-Cardiology/Articles/2022/10/07/17/21/Preoperative-Cessation-of-SGLT2i. Accessed August 5, 2024.
- Preiser JC, Provenzano B, Mongkolpun W, et al. Perioperative management of oral glucose-lowering drugs in the patient with type 2 diabetes. Anesthesiology. 2020;133:430–438. PMID: 32667156.
- Seki H, Ideno S, Shiga T, et al. Sodium-glucose cotransporter 2 inhibitor-associated perioperative ketoacidosis: a systematic review of case reports. J Anesth. 2023; 37:465–473. PMID: 36849747.
- Handelsman Y, Bloomgarden ZT, DeFronzo RA, et al. American Association of Clinical Endocrinologists and American College of Endocrinology position statement on the association of SGLT-2 inhibitors and diabetic ketoacidosis. Endocr Pract. 2016;22:753–762. PMID: 27082665.
- Garber AJ, Handelsman Y, Grunberger G, et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type 2 diabetes management algorithm—2020 executive summary. Endocr Pract. 2020;26:107–129. PMID: 32022600.
- Grant B, Chowdhury TS. New guidance on the periperative management of diabetes. Clin Med. 2022; 22:41–44. PMID: 34921055.
- Thiruvenkatarajan V, Meyer EJ, Nanajappa N, et al. Perioperative diabetic ketoacidosis associated with sodium-glucose co-transporter-2 inhibitors: a systematic review. Br J Anesth. 2019; 123:27–36. PMID: 31060732.
- Tang H, Li D, Wang T, et al. Effect of sodium-glucose cotransporter 2 inhibtors on diabetic ketoacidosis among patients with type 2 diabetes: a meta-analysis of randomized controlled trials. Diabetes Care. 2016;39:e123–124. PMID: 27311492.
- Monami M, Nreu B, Zannoni S, et al. Effects of SGLT-2 inhibitors on diabetic ketoacidosis: a meta-analysis of randomized controlled trials. Diabetes Res Clin Pr. 2017;130:53–60. PMID: 28570924.
- Lui DTW, Wu T, Au ICH et al. A population-based study of SGLT2 inhibitor-associated postoperative diabetic ketoacidosis in patients with type 2 diabetes. Drug Saf. 2023;46:53–64. PMID: 36289137.
- Pujara S, Ioachimescu A. Prolonged ketosis in a patient with euglycemic diabetic ketoacidosis secondary to dapagliflozin. J Investig Med High Impact Case Rep. 2017;5:2324709617710040. PMID: 28589154.
- Steinhorn B, Wiener-Kronish J. Dose-dependent relationship between SGLT2 inhibitor hold time and risk for postoperative anion gap acidosis: a single-centre retrospective analysis. Br J Anesth. 2023;131:682–686. PMID: 37541949.
- Raiten JM, Morlok A, D’Ambrosia S, et al. Perioperative management of patients receiving sodium-glucose cotransporter 2 inhibitors: development of a clinical guideline at a large academic center. J Cardio Vasc An. 2024;38:57–66. PMID: 37932195.
- Packer M, Butler J, Zeller C, et al. Blinded withdrawal of long-term randomized treatment with empagliflozin or placebo in patients with heart failure. Circulation. 2023;148:1011–1022. PMID: 37621153.
- Oosterom-Eijmael MJP, Hermanides J, van Raalte DH, Hulst AH. Risk of perioperative discontinuation of SGLT2 inhibitors. Br J Anesth. 2024;133:239–240. PMID: 38834489.
- Mehta PB, Robinson A, Burkhardt D, et al. Inpatient perioperative euglycemic diabetic ketoacidosis due to sodium-glucose cotransporter-2 inhibitors – lessons from a case series and strategies to decrease incidence. Endocr Pract. 2022;28:884-888. PMID: 35753675.
