Epidural steroid injections are frequently performed for patients with lumbar and cervical radiculopathy, the accepted indications. A review of Medicare insurance claims carried out in 2001 indicated a procedure rate of 26.5 per 1000 nationwide among Medicare recipients 65 and older.1 The rate of serious complications resulting from these procedures is impossible to estimate in the U.S. because of the lack of mandatory reporting and the reluctance to report cases that are being or may become litigated. The ASA Closed Claims Project indicated that epidural steroid injections accounted for 40% of all claims involving pain management cases that occurred between 1970 and 1999.2 Fourteen cases of spinal cord injury were reported, of which 6 resulted in paraplegia and 1 in quadriplegia. With the rapid increase in procedure rates for epidural steroid injections since that time, the incidence of these devastating complications has undoubtedly increased. Given the potential for serious complications following epidural steroid injections, it is important that the procedure be avoided for patients who are unlikely to respond, such as those with purely axial back pain, neural claudication, and non-radicular sources of back and leg pain.
Unfortunately, physicians who participate as expert witnesses in malpractice claims report much of the information regarding spinal cord injury associated with epidural steroid injections verbally and informally. However, information from those sources as well as from the few published reports of complications can provide some insight into the mechanisms and causes of some very preventable complications.
The most likely causes of spinal cord injury following epidural steroid injection are epidural bleeding, epidural abscess, direct spinal cord trauma, and embolization of particulate matter into the arterial supply of the cord. The first 2 causes should be extremely rare with the use of meticulous aseptic technique and adherence to guidelines regarding the use of antithrombotic and thrombolytic agents (see Practice Advisory at ASRA.com). This discussion will concentrate on the 2 latter issues.
 |
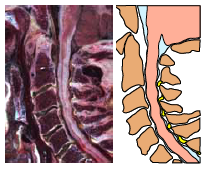 |
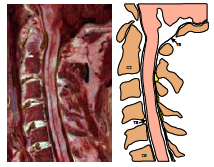
| Midline sagittal cryomicrotome section and index drawing of cervical vertebral column from C1 to C6 of a 65-year-old male. The C3 and C5 vertebral bodies are indicated by “3” and “5.” The cord occupies a large share of the vertebral canal. Minimal epidural fat and veins are found in the anterior epidural space. There is no posterior epidural compartment because the dura is uniformly in contact with the ligamanta flava and lamina. From Hogan QH: Epidural anatomy examined by cryomicrotome section. Regional Anesthesia 1996;21:395-406. Reprinted with permission. | Midline sagittal cryomicrotome section and drawing of cervical vertebral column of a 75-year-old male, revealing severe degenerative disc disease at all disc levels. Disc material has extruded into the spinal canal at levels C5-6 and C6-7. Thickening of the dura, buckling of the ligamanta flava, osteophyte formation at the vertebral body margins, and extruded disc material have resulted in cord compression and deformity with minimal cerebrospinal fluid surrounding the cord. The only posterior epidural space is at C7-T1 (just visible at the right picture margin). From Hogan QH: Epidural anatomy examined by cryomicrotome section. Regional Anesthesia 1996;21:395-406. Reprinted with permission. |
Direct Spinal Cord Injury
Some of the opinions and information presented here are based on medical records observed by physicians serving as expert witnesses in malpractice cases that are now closed. There are only a few published reports of such complications.
It is important to realize that although needle penetration of the spinal cord can produce injuries, with a wide range of severity, injection of any material into the cord is invariably devastating. It is critical, therefore, to insure proper needle placement prior to injecting anything, including contrast dye. The vast majority of serious injuries related to cord trauma are associated with cervical epidurals. Following are some suggestions that should help minimize the risk of serious injury:
- Obtain and view MRI scans prior to performing the procedure. Disc herniation may shift the cord posteriorly and obliterate the posterior subarachnoid space. In patients with previous cervical spine surgery there may be scar formation and adherence of dura to more superficial tissues at the proposed level of injection, increasing the risk of direct needle trauma to the cord. If there is pre-existing canal stenosis and spinal cord compression, the additional pressure created by the volume of drug injected, or by the pharmacological effect of those drugs, may result in neurological injury, particularly if there is already some loss of function.
- Avoid epidural needle placement above C6-7. There is typically a small amount of epidural fat in the midline posteriorly at C7-T1, creating a space between the ligamentum flavum and the dura. Midline epidural fat is minimal at C6-7, and there is none at C5-6 and above. Low volume cervical injections often spread upward several segments. If it is felt that steroid placement at higher levels is indicated, it may be safer to introduce an epidural catheter in the upper thoracic spine and advance it under fluoroscopy to the desired level.
- When possible, obtain a lateral view of the spine following needle placement prior to injecting. This is difficult at the lower cervical levels because of the superimposed shoulder joints, particularly in thick-necked patients. A “swimmer’s view,” with one arm at the side, the other raised above the head, has been used successfully to obtain a view of the needle within the spinal canal.3
- Avoid deep sedation. The deeply sedated patient may become agitated and may move unexpectedly. Also, paresthesias may alert us to the fact that we have contacted the cord. There are many anecdotal accounts of patients who have had intense paresthesias and/or motor responses to contact of a needle with the spinal cord, as well as a number of cases in which general anesthesia or moderate to deep sedation appeared to block such responses.4 Unfortunately, even in the non-sedated patient, needle entry into the cord may not result in a noticeable response.5,6 Nevertheless, the vigilance of an awake patient offers at least some added safety.
- Do not use the hanging drop technique to determine epidural needle placement, since this is not a reliable means of identifying the epidural space. I am aware of 2 malpractice claims in which spinal cord injury was associated with failure of the hanging drop technique to indicate epidural needle entry.
Ischemic Spinal Cord and Brain Injury
Reports of spinal cord, brainstem, and cerebellar infarction following cervical transforaminal epidural steroid injections began to appear in the scientific literature in the early 2000s.7 It was postulated that such Injuries might result from accidental injection of particulate material into radicular arteries lying adjacent to the targeted nerve root. Demonstration of contrast dye spread into a radicular artery during transforaminal injection confirmed the likelihood of intra-arterial drug injection as a cause of ischemic injury,8 and it has been shown that essentially all commercially-available steroid suspensions contain particles large enough to occlude arterioles and capillaries.9 Spinal cord injury has also been documented following transforaminal steroid injections at lumbar, sacral,10 and thoracolumbar levels.11 During intra-arterial injection, contrast is likely to spread epidurally as well as intravascularly, and the thin pattern of intra-arterial spread is easy to miss.12 Digital subtraction fluoroscopy can enhance the visualization of the intravascular dye.8 Undoubtedly, the use of small gauge needles increases the likelihood of intra-arterial spread. The use of a pencil point side port needle does not appear to offer protection against this complication.13 Another possible mechanism of cord injury following foraminal injection is needle placement into the dorsal root ganglion. This structure is large and is positioned at the outer margin of the intervertebral foramen. The very short length of dorsal roots at this level (e.g., 1 cm) increases the likelihood of delivery of injectate into the substance of the cord.
Following are some suggestions to reduce the risk of intraneural injection or intra-arterial embolization of particulate steroids:
- Following aspiration, inject contrast under live fluoroscopy. Obtain a still image a few seconds later to insure that the dye pattern has not changed. If available, use digital subtraction. Inject dye through small extension tubing to minimize needle tip movement between dye and steroid injection.
- Consider a local anesthetic test dose with minimal sedation. Look for signs of systemic symptoms and numbness and paresthesias locally.
- Consider the use of non-particulate steroids. This is controversial, as there is little evidence that soluble steroids have equivalent efficacy, and early studies indicated that soluble steroid preparations remain in the spinal canal only for brief periods.14
- Consider using the interlaminar approach, particularly for cervical injections. The arteries supplying the spinal cord do not traverse the dorsal epidural space, so the risk of injecting a radicular artery or dorsal root ganglion by this approach is minimal. The evidence for the superiority of transforaminal epidurals is largely theoretical and is based mainly upon non-controlled case series.15,16 Avoid transforaminal injections when contrast dye is contraindicated. Make sure patients are aware of the risks associated with both types of injections.
Conclusions
Epidural steroid injections can be helpful for hastening recovery from radiculopathy following disc herniation and can provide temporary relief for patients with chronic radicular pain. There is little evidence that they are of benefit for patients with axial back pain or neural claudication associated with spinal stenosis. There is little evidence that they reduce the need for spine surgery or that they improve long-term outcomes. It is important that patients understand the risks and benefits of these procedures and that we do everything possible to prevent rare but catastrophic neurological complications.
References
- Friedly J, Chan L, Deyo R. Geographic variation in epidural steroid injection use in medicare patients. J Bone Joint Surg Am 2008;90:1730-7.
- Fitzgibbon DR, Posner KL, Domino KB, et al. Chronic pain management: American Society of Anesthesiologists Closed Claims Project. Anesthesiology 2004;100:98-105.
- Abbasi A, Malhotra G. The “swimmer’s view” as alternative when lateral view is inadequate during interlaminar cervical epidural steroid injections. Pain Med 2010;11:709-12.
- Hodges SD, Castleberg RL, Miller T, et al. Cervical epidural steroid injection with intrinsic spinal cord damage. Two case reports. Spine (Phila Pa 1976) 1998;23:2137-42.
- Tripathi M, Nath SS, Gupta RK. Paraplegia after intracord injection during attempted epidural steroid injection in an awake-patient. Anesth Analg 2005;101:1209-11.
- Simon SL, Abrahams JM, Sean Grady M, et al. Intramedullary injection of contrast into the cervical spinal cord during cervical myelography: a case report. Spine (Phila Pa 1976) 2002;27:E274-7.
- Brouwers PJ, Kottink EJ, Simon MA, et al. A cervical anterior spinal artery syndrome after diagnostic blockade of the right C6-nerve root. Pain 2001;91:397-9.
- Baker R, Dreyfuss P, Mercer S, et al. Cervical transforaminal injection of corticosteroids into a radicular artery: a possible mechanism for spinal cord injury. Pain 2003;103:211-5.
- Tiso RL, Cutler T, Catania JA, et al. Adverse central nervous system sequelae after selective transforaminal block: the role of corticosteroids. Spine J 2004;4:468-74.
- Houten JK, Errico TJ. Paraplegia after lumbosacral nerve root block: report of three cases. Spine J 2002;2:70-5.
- Glaser SE, Falco F. Paraplegia following a thoracolumbar transforaminal epidural steroid injection. Pain Physician 2005;8:309-14.
- Smuck M, Tang CT, Fuller BJ. Incidence of simultaneous epidural and vascular injection during cervical transforaminal epidural injections. Spine (Phila Pa 1976) 2009;34:E751-5.
- Smuck M, Leung D. Inadvertent injection of a cervical radicular artery using an atraumatic pencil-point needle. Spine (Phila Pa 1976) 2011;36:E220-3.
- Gardner WJ, Goebert HW Jr, Shegal AD. Intraspinal corticosteroids in the treatment of sciatica. Trans Am Neurol Assoc 1961;86:214-5.
- Schaufele MK, Hatch L, Jones W. Interlaminar versus transforaminal epidural injections for the treatment of symptomatic lumbar intervertebral disc herniations. Pain Physician 2006;9:361-6.
- Smith CC, Booker T, Schaufele MK, et al. Interlaminar versus transforaminal epidural steroid injections for the treatment of symptomatic lumbar spinal stenosis. Pain Med 2010;11:1511-5.