Wiretap laws govern the legality of audio recordings and vary state to state. Here, we summarize the various states’ wiretap laws, the remedies or punishments that can be exacted for violation of a wiretap law, and the applicability of these laws to patient safety initiatives. Through case examples, we provide guidance for how to manage clinical situations where wiretap laws may be applicable.
INTRODUCTION TO WIRETAPPING LAWS
In the United States, many federal and state laws have connections to patient safety of relevance for anesthesia professionals (including, but not limited to the various public health laws,1 the United States’ Patient Safety and Quality Improvement Act of 2005,2 and peer review law3). A recent publication on wiretap laws and the perioperative physician in the Journal of Clinical Anesthesia highlights an important legal concept that has potential applications to both routine clinical practice and patient safety.4
Wiretapping laws or “eavesdropping” statutes govern whether an audio recording—of face-to-face conversations, telephone calls, or any other oral or wire (hence the name) communications— was made legally. Most of the wiretapping statutes in the United States were passed in the 1960s and 1970s, when accessibility to recording devices was not as prevalent. These laws still remain in place today with some amendments and modifications, at a time when easily concealable recording devices (namely, our cellphones) are ubiquitous.
Wiretap Laws Vary from State to State
Within the United States, wiretap laws vary from state to state and can be classified as being one-party, all-party, or “mixed.” One-party consent jurisdictions require only one party to consent to an audio recording, whereas all-party consent jurisdictions require all present parties to consent. It is worth emphasizing that “all-party” is truly descriptive; if not all parties consent to the audio recording, either the recording has to cease, or the nonconsenting party has to remove themselves from the area of recording.4
Thirty-seven states require one-party consent, nine require all-party consent (California, Florida, Illinois, Maryland, Massachusetts, Montana, New Hampshire, Pennsylvania and Washington), and the remaining four (Connecticut, Michigan, Nevada, and Oregon) have mixed wiretap statutes (Figure 1).4 Depending on the state, criminal punishments are classified as felonies or misdemeanors, and include fines ranging from $500 to $100,000, incarceration (ranging from 6 months to 20 years), or both. Civil recoveries range from $100 to $25,000, or recovery of civil remedies including damages, attorney fees, and litigation costs are also possible.4
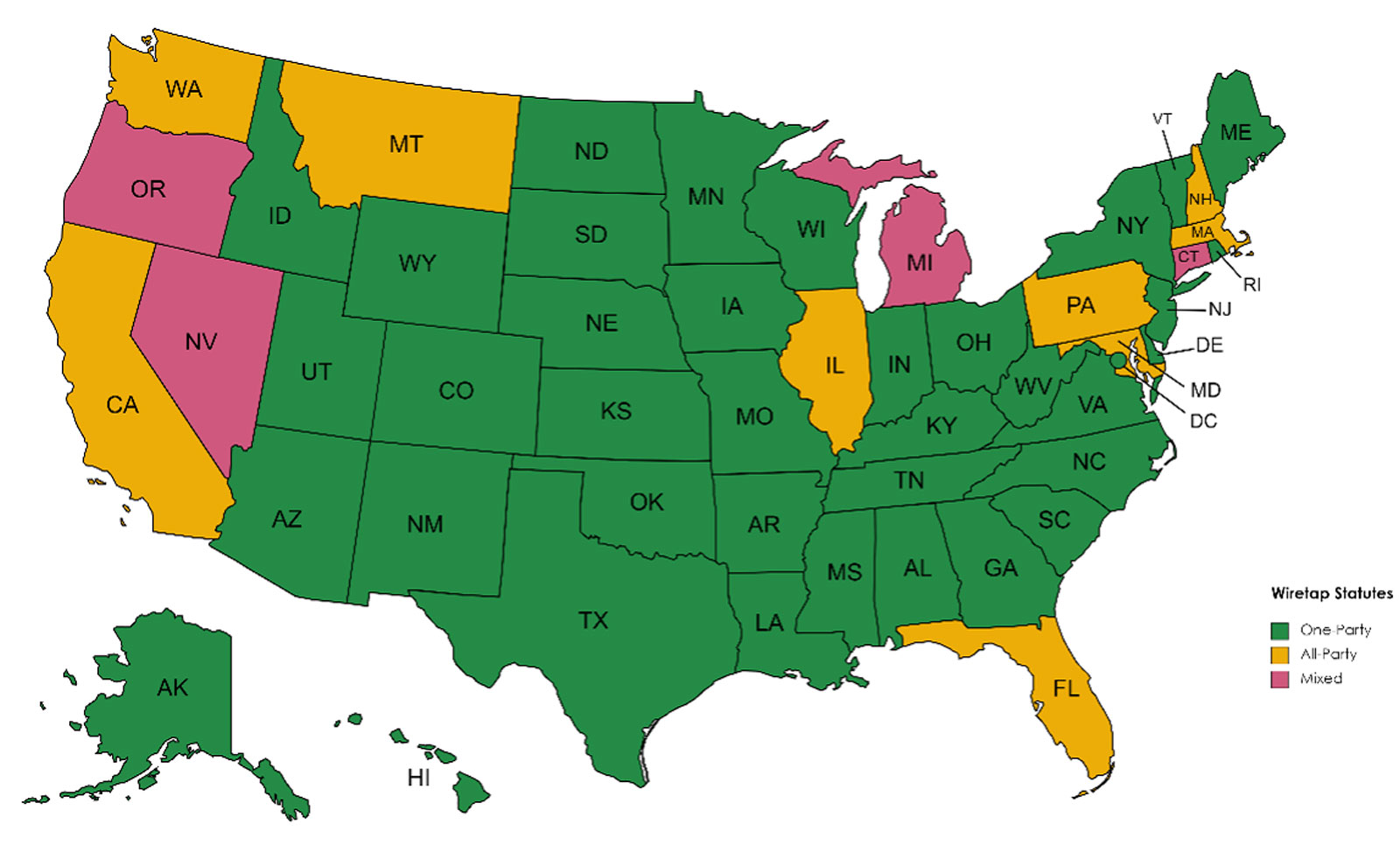
Figure 1: Classification of wiretap statutes as one-party, all-party or mixed, based on “Wiretap laws and the perioperative physician—the current state of affairs.” de Menses et al. J Clin Anesth. 2023.4 Map created using mapchart.net
Wiretapping laws are distinct from the Health Insurance Portability and Accountability Act (HIPAA), which protects patients from being photographed or videotaped.5 While there are potential situations where both laws may be applicable, wiretapping laws apply to the unconsented audio recording of any individual, including clinicians. For example, patients or family members can record clinicians, clinicians can record patients, clinicians can record one another, or nonclinical hospital employees could make a recording—and all of these situations may consequently be subject to the various states’ wiretap statutes.
Additionally, clinicians must be aware that even if a recording is made without appropriate consent, that recording may still be admissible in court—with the proviso that the recorder may be deterred because, in so doing, they would be submitting evidence that, in some states, constitutes a felony, and may subsequently be charged with violation of a wiretap statute.4
While hospital policy may help guide clinicians and patients as to how to act when faced with a recording or a request to record, the relevant state law trumps hospital policy. In other words, even if a hospital allows audio recording, the individuals are ultimately subject to the applicable state’s wiretapping laws regarding the legality of a recording.
APPLICABILITY TO CLINICAL WORK AND PATIENT SAFETY
Audio recordings have many potential safety implications. Anesthesia professionals, who work in multiple areas of the hospital may be exposed to audio recordings at any time. For instance, with the ubiquity of cellphones, patients may wish to make audiovisual recordings of clinic visits, provider instructions (such as discharge instructions), discussions held during rounds (such as in the intensive care unit), or certain events in the hospital, such as the birth of their child.6-8 These recordings can certainly be valuable: patients can improve their recall and understanding of the discussed medical information, and can share the information with family members.8,9 When patients share an understanding of their medical care and have the support and encouragement of their family members, this has the potential to improve compliance with medical instructions. Additionally, allowing patients to record clinical interactions may theoretically improve the patient-clinician relationship, increase the patient’s trust in the anesthesia professional, and may also make them more likely to follow medical instructions.10 Compliance with medical instructions is associated with improved patient outcomes across multiple medical specialties and health care measures.
Patients who do not share the same language as their health care provider are particularly vulnerable. Recording the interaction, including the interpretation, allows patients to carefully listen to the translation and potentially even verify the accuracy of the interpretation.
Telemedicine and medical transcription services, used in areas such as intensive care units or in clinics, have burgeoned since the pandemic. The use of these services have their own implications on patient safety, such as increasing accessibility for patients who may be remote from care.11 However, all of these services need to take into account relevant wiretap laws.
Similar to the desire to record egregious incidents in the community (such as interactions with police and other public officials), patients and clinicians may wish to record a clinical event in the hospital. This may include an unprofessional interaction, medical error, or an adverse event. Awareness of an event may induce change for the better and may improve patient safety. While wiretap laws may restrict such recordings, it is important to bear in mind that laws can change. For example, in Massachusetts, which has one of the strictest all-party wiretap consent laws in the country, allowing the recording of police is currently being contested in the courts.12 Similarly, wiretap laws in all-party consent states could be amended to allow recording adverse events in clinical situations, with the goal of improving patient safety.
Additionally, there are various published initiatives that advocate recording clinical practice to improve patient care and safety: for instance, to allow families to watch surgeries as part of family- and patient-centered care.13,14 Another example is in the use of an operating room Black Box to record surgeries with the intention of characterizing intraoperative errors, events, and distractions.15 Such technology has the potential to improve care and patient safety by decreasing medical errors or improving communication. Importantly though, wiretap laws still remain applicable. For example, using a Black Box in an all-party consent state becomes legally complicated, as all present parties (which may change over the duration of the surgery or recording) need to consent to being audio recorded; the hospital cannot provide blanket consent. Clinicians that do not consent would need to leave and may need to be replaced, which has vast implications given current physician and nursing staffing shortages.14 A potential solution is to exclusively utilize image-recording and not audio recording, recognizing that this would limit the ability to characterize communication errors.14
In summary, anesthesia professionals in daily practice, as well as any patient safety and quality improvement initiatives that leverage the use of audio recording, should all take into account relevant state wiretapping laws, and the legal limitations to audio recordings they pose.
PRACTICAL SUGGESTIONS
Many may feel that if the intention behind the recording is good—for example, if it is made for personal private use, or to capture (and later report) an error, adverse event, or hostile interaction—the recording may be warranted. However, if the appropriate consent is not obtained prior to making an audio recording, it potentially demonstrates violation of a state’s wiretap laws. As an illustrative example, when a high school student in an all-party consent state recorded a bullying incident and presented the video to their school principal, they were charged with violation of their state wiretap law.16 While those charges were later dropped, this example highlights that audio recording without appropriate consent can be contrary to the law.
While there may be scenarios where anesthesia professionals can expect to address wiretap laws (such as in the case of medical transcription), there are many times the wiretap laws can become relevant unexpectedly. It can be challenging to step away and consult legal help, and consequently it is imperative that all clinicians are not only aware of and understand how their state’s wiretapping laws affect audio recordings, but also how they may choose to respond to a particular situation. Some individuals may feel indifferent to being recorded, while others may be strong advocates of being recorded; these feelings can change depending on the situation at hand.
The following are some hypothetical situations where wiretapping laws may apply as well as recommendations for how to react. These recommendations are a balance of multiple factors, including educating all present about the law (since most individuals tend to be unaware of wiretapping laws), allowing those involved to make a decision regarding their legal rights, and maintaining the patient-clinician relationship.
Situation 1: You are the anesthesia professional wheeling a patient into the operating room. You notice a film crew videotaping you as you walk in. When you inquire about the filming, the surgeon informs you that they are there to film the entire surgery, including aspects of the anesthesia care “to improve safety.” They’ve “already obtained consent from everyone,” but this is the first time you are learning about this.
Situation 2: You are placing an epidural for a laboring patient. The significant other has remained in the room, as is customary at your institution.
As you complete the procedure and prepare to administer the test dose, you look up and notice the significant other is standing to your side and is holding up their cellphone which is pointed at you. You ask whether they have been filming, to which they respond uncomfortably that they are not, and put their phone away.
Situation 3: You are seeing patients via telemedicine in your chronic pain clinic. You discuss the use of medical transcription services with your next patient. They provide consent to being recorded, after which they ask if they, too, can record the clinic visit for their own personal use.
Suggestions: If aware of a video recording (Situations 1, 2 and 3), we recommend verbalizing that the recording is occurring. In an all-party consent state, it may be helpful to inform all present that every person has to consent. For example: “I see that you are recording. In our state, everyone present has to consent to recording. I do/do not consent to recording.” If all parties do not consent to being recorded, either the recording has to stop, or those who do not consent have to leave the area. Individuals who feel uncomfortable with being direct may find it useful to cite hospital policy (if one exists at their institution): “It is hospital policy not to allow video recordings.” While citing hospital policy can be helpful to diffuse an uncomfortable situation, bear in mind the hospital cannot consent on others’ behalf (Situation 1).
In the situation where the individual is lying about recording or is secretly recording (Situation 2), it can still be helpful to state whether you do/do not consent to being recorded. While the recording may be admissible in court, the individual may be deterred from doing so as they would be submitting evidence that they may have violated a state law (particularly if in an all-party consent state).
It may be helpful, particularly if in a one-party consent state (where the recording individual has the right to record even without everyone’s consent), to explore the reasons why the individual is pursuing the recording (Situations 2 and 3), and to suggest alternate ways to provide them with this information (such as requesting their medical records).
In the situation of medical transcription (Situation 3), we recommend similarly informing all parties about the recording and obtaining consent, particularly since the parties may be in different states, which could include an all-party consent state. Depending on the locations of the respective individuals (i.e., the patient(s) and clinician(s)), one-party or all-party wiretap laws may apply.4
Deciding whether to consent to a recording is up to each individual person. We feel it is important to bear in mind the relationship with the recording individual, whether there are alternative ways to provide satisfactory information that do not entail recording, and how likely consenting to being recorded may end up in litigation—something that, in reality, is completely out of your control once you consent to being recorded.

CONCLUSION
Anesthesia Professionals Need to Be Aware of Wiretap Laws
While currently all of the described situations are potentially governed by wiretapping laws, as technology continues to improve, there may be additional scenarios where wiretapping laws could become applicable. Therefore, in the daily practice of anesthesiology, and additionally in considering initiatives that may involve audio recording, all anesthesia professionals need to be aware of wiretap laws, how a particular state’s laws may impact the legality of any audio recordings, and the potential criminal punishments and civil remedies that can be imposed for violations. Unless a major overhaul of United States wiretapping laws were to occur, it behooves all anesthesia professionals to be well versed in the multitude of situations where wiretap laws are or could be applicable, and how they would react to these scenarios.
Karolina Brook is an anesthesiologist in the Department of Anesthesiology at Boston Medical Center, Boston, MA, and an assistant professor in the Department of Anesthesiology, Boston University Chobanian and Avedisian School of Medicine, Boston, MA.
Karolina Brook, MD, has no conflicts of interest.
REFERENCES
- Gostin LO. Public health law in a new century: part I: law as a tool to advance the community’s health. JAMA. 2000;283:2837–2841. PMID: 10838654.
- Office for Civil Rights (OCR). Patient Safety and Quality Improvement Act of 2005 statute and rule. Published May 7, 2008. https://www.hhs.gov/hipaa/for-professionals/patient-safety/statute-and-rule/index.html. Accessed October 30, 2023.
- Apold J, Daniels T, Sonneborn M. Promoting collaboration and transparency in patient safety. Jt Comm J Qual Patient Saf. 2006;32:672—675. PMID: 17220155.
- de Meneses FGA, Mulcahy BP, Brook K. Wiretap laws and the perioperative physician—the current state of affairs. J Clin Anesth. 2023;89:111178. PMID: 37327714.
- Office for Civil Rights (OCR). HIPAA for professionals. Published September 10, 2015. https://www.hhs.gov/hipaa/for-professionals/index.html. Accessed October 30, 2023.
- Elwyn G. “Patientgate”—digital recordings change everything. BMJ. 2014;348:g2078. PMID: 24620357.
- Elwyn G, Barr PJ, Castaldo M. Can patients make recordings of medical encounters?: What does the law say? JAMA. 2017;318:513–514. PMID: 28692707.
- Rodriguez M, Morrow J, Seifi A. Ethical implications of patients and families secretly recording conversations with physicians. JAMA. 2015;313:1615–1616. PMID: 25763514.
- Tsulukidze M, Durand MA, Barr PJ, et al. Providing recording of clinical consultation to patients—a highly valued but underutilized intervention: a scoping review. Patient Educ Couns. 2014;95:297–304. PMID: 24630697.
- Pearson SD, Raeke LH. Patients’ trust in physicians: many theories, few measures, and little data. J Gen Intern Med. 2000;15:509–513. PMID: 10940139.
- Khoong EC, Sharma AE, Gupta K, et al. The abrupt expansion of ambulatory telemedicine: implications for patient safety. J Gen Intern Med. 2022;37:1270–1274. PMID: 35048294.
- www.mass.gov. Massachusetts law about police conduct.https://www.mass.gov/info-details/massachusetts-law-about-police-conduct#%3E-massachusetts-laws. Accessed January 4, 2022.
- Quiñónez ZA, Pyke-Grimm KA, Char D. Could, should families watch their loved one’s surgeries and, if so, when? Anesth Analg. 2022;135:704–707. PMID: 36108184.
- Brook K, de Meneses FGA, Quraishi SA. Recording clinical interactions and wiretapping laws. Anesth Analg. 2023;136:e28–e29. PMID: 37205811.
- Jung JJ, Jüni P, Lebovic G, Grantcharov T. First-year analysis of the operating room Black Box study. Ann Surg. 2020;271:122–127. PMID: 29916872.
- Fairlie & Lippy, P.C. High school sophomore charged with wiretapping for recording bullying. https://fairlielaw.com/high-school-sophomore-charged-with-wiretapping-for-recording-bullying/. Accessed January 4, 2022.
