DEAR RAPID RESPONSE:
 Since the 1970s, the pulse oximeter (PO) has enabled noninvasive continuous assessment of arterial blood oxygenation as well as pulse rate. The pulse estimate is derived from the plethysmographic waveform and serves as a proxy for pulsatile perfusion. The audible tone supports rate and rhythm monitoring while the bedside clinician is multitasking, with a variable pitch to reflect oxygen saturation. Pulse oximetry based pulse rate monitoring offers an additional source of information since interference can cause ECG-based rate monitoring to be unreliable. The overall utility of PO monitoring is unquestioned, but the underlying technology is complex. Based upon the differential absorption characteristics of oxy- and deoxyhemoglobin and arterial pulsations, there are many factors that can interfere with the PO measurement, and extensive signal processing is required to obtain useful information. This report highlights clinical scenarios where the PO rate measurement and associated tone rate did not adequately change despite significantly altered arterial pulsations.
Since the 1970s, the pulse oximeter (PO) has enabled noninvasive continuous assessment of arterial blood oxygenation as well as pulse rate. The pulse estimate is derived from the plethysmographic waveform and serves as a proxy for pulsatile perfusion. The audible tone supports rate and rhythm monitoring while the bedside clinician is multitasking, with a variable pitch to reflect oxygen saturation. Pulse oximetry based pulse rate monitoring offers an additional source of information since interference can cause ECG-based rate monitoring to be unreliable. The overall utility of PO monitoring is unquestioned, but the underlying technology is complex. Based upon the differential absorption characteristics of oxy- and deoxyhemoglobin and arterial pulsations, there are many factors that can interfere with the PO measurement, and extensive signal processing is required to obtain useful information. This report highlights clinical scenarios where the PO rate measurement and associated tone rate did not adequately change despite significantly altered arterial pulsations.
The observations reported here occurred after a major update of bedside patient monitors in our center. The first observation occurred in patients on cardiopulmonary bypass (CPB), and the second was in non-CPB patients with life threatening arrhythmias. Our monitoring setup consists of a Masimo SET pulse oximeter (integrated SpO2 version MS:DSP:V05:03.01.08), set to 2–4- or 4–6-seconds data averaging with optical probe RD SET sensors, applied to a digit (or ear, in our asystole case) as per the manufacturer’s recommendation (Masimo Corporation, Irvine, California, USA). The PO is integrated into Mindray N1 monitoring, with the PO pulse rate set as the primary source of audible rate representation (Mindray Global, Nanshan, Shenzhen, P.R. China). The Smart Tone feature of the Masimo PO is enabled and cannot be disabled. This feature is designed to maintain a variable pitch saturation tone during low signal-to-noise conditions. However, in the CPB setting, false pulse rates are indicated by the PO in at least half of our patients during bypass, even during aortic cross-clamping. The reported rate was not linked to the CPB’s pump settings. Figure 1 shows two examples during a period of absent pulsatility where the PO reported a pulse rate close to the previous baseline in the mid-60s. The monitor’s audible tone kept a regular pace and stable pitch. We reported this experience to the manufacturer and an initial audit by the company did not identify any malfunctions. The manufacturer’s manual stated that “Masimo SET will continue to report accurate arterial oxygen saturation and pulse rate readings during motion and low perfusion, even when the plethysmographic waveform is suboptimal,” and that “It is important to note that even with ‘Low Signal IQ,’ the measurement has a high probability of being correct; otherwise the system would not display values at all.”1 In this CPB setting, however, we would suggest that the algorithm fails to correctly reflect the current pulse rate.
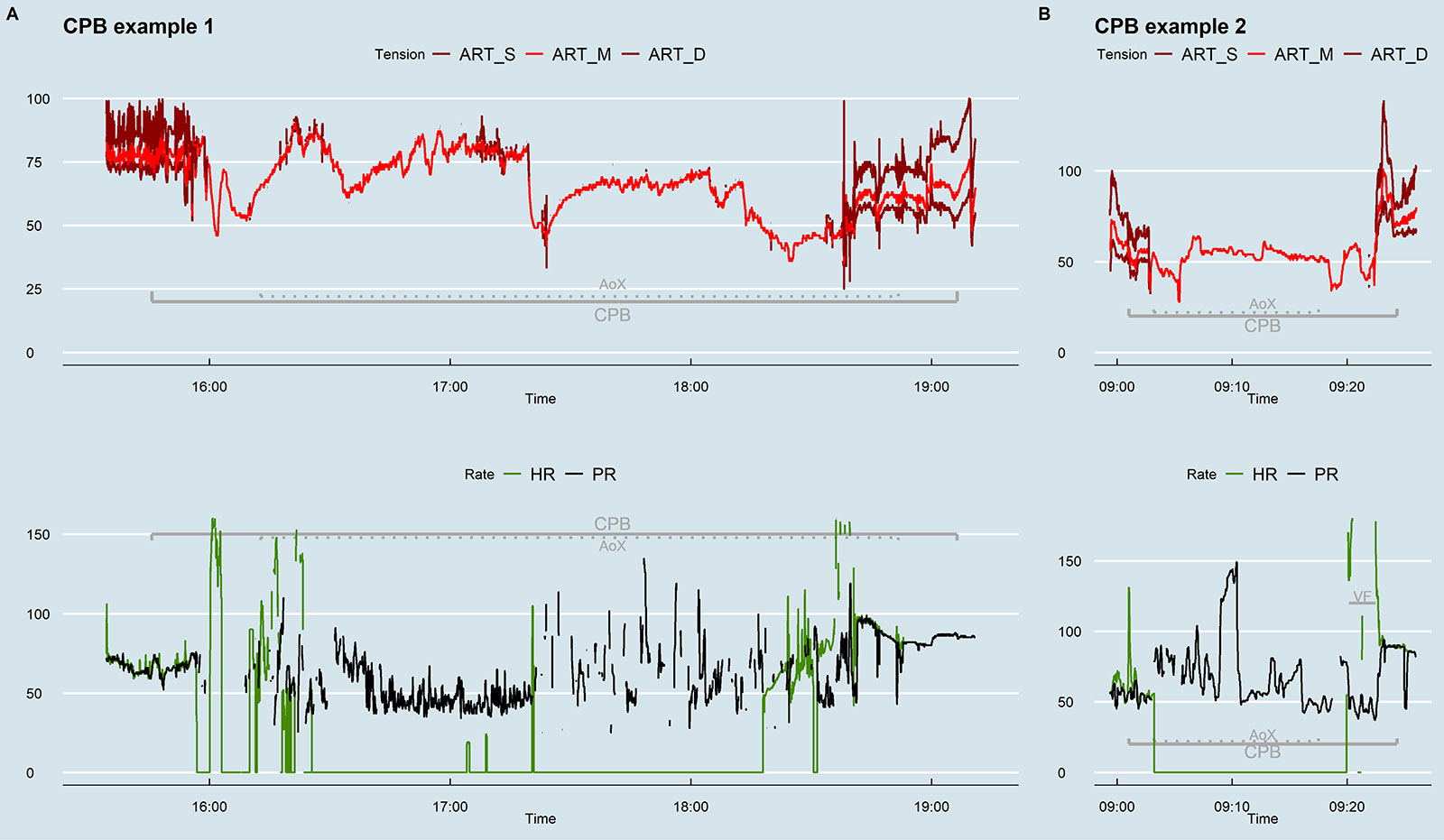
Figure 1: Arterial pressures, ECG-derived heart rate (HR), and pulse oximeter-derived pulse rate (PR) in two cases, during cardiopulmonary bypass (CPB) and aortic cross-clamping (AoX). Note that PR detection is also maintained during ventricular fibrillation (VF) after declamping in the second example.
The second observation involved patients with life-threatening arrhythmias where the Masimo PO pulse rate falsely indicated a stable heart rate and rhythm. We noticed this in one patient who suddenly developed ventricular fibrillation (VF) after CPB was terminated and in two patients with extreme bradycardia. The VF occurred after CPB for aortic valve replacement, during surgical hemostasis, with the sternum still open (figure 2, left panel). The resulting low cardiac output was evidenced by hypotension and a drop in end-tidal carbon dioxide. After 23 seconds, successful defibrillation restored hemodynamics.
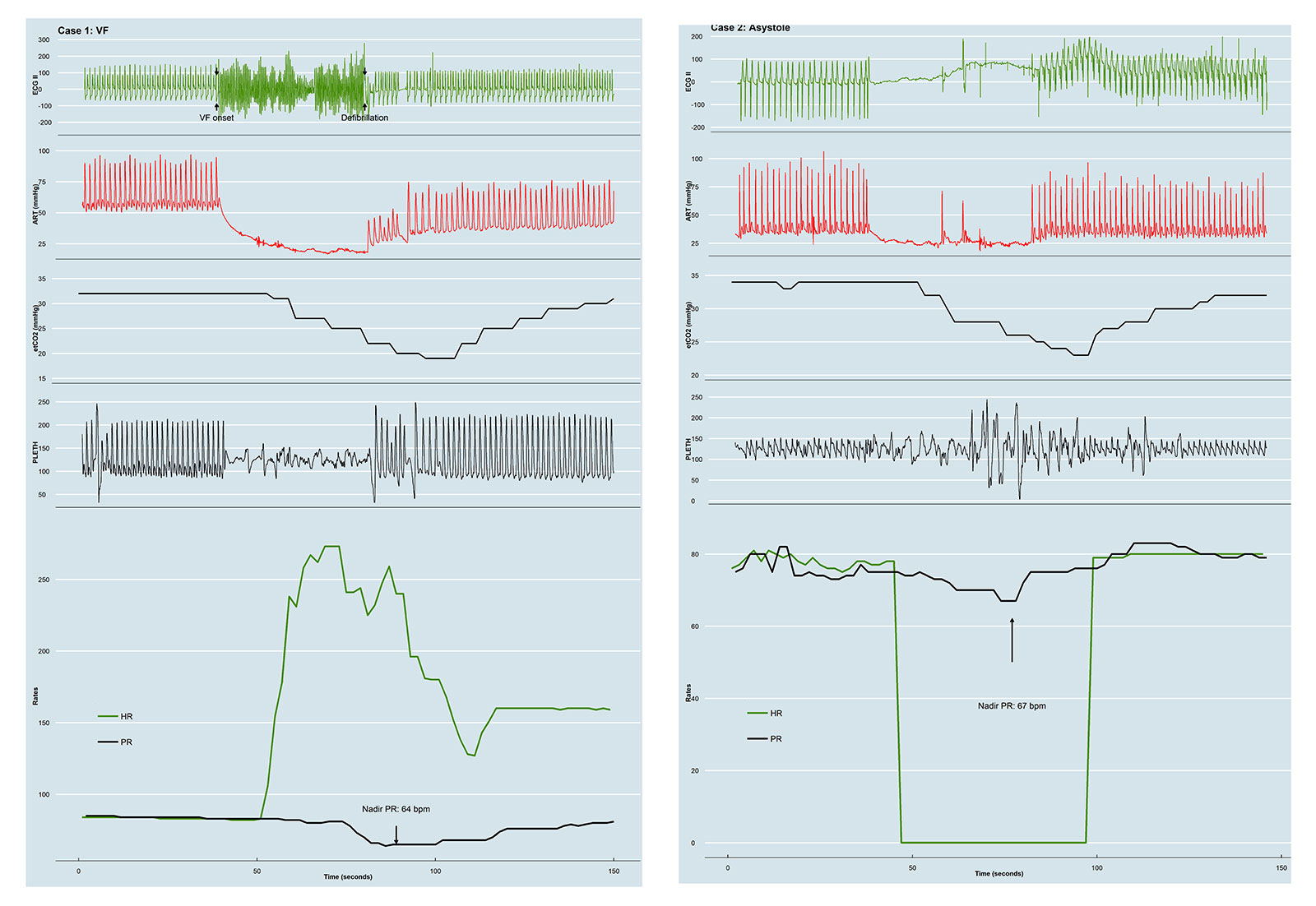
Figure 2: ECG, arterial pressure, end-tidal capnography, and pulse oximetry data, as well as ECG-derived heart rate (HR) and pulse oximeter-derived pulse rate (PR). Sudden onset ventricular fibrillation (left) and acute asystole (right) with hemodynamic effects, without significant effect on pulse oximetric pulse rate measurement.
Shortly after the VF began, erratic oscillations were captured by the PO sensor that did not exist before or after the VF and subsequent defibrillation, although the patient was lying still, and no major external movement was applied to the patient’s finger or PO. During this episode, the PO pulse rate exhibited only a moderate decline in pulse rate 15 seconds after the VF began, falling to 64 beats per minute after 24 seconds. Once again, the Mindray monitor’s audible tone reflected this moderate decline in pulse rate. Following the defibrillation, the waveforms of the ECG, arterial pressure, and plethysmographic waveforms show that the heart rate returned to its pre-VF rate; however, the ECG-based heart rate was double counting while the PO pulse rate accurately returned to the pre-VF rate.
In an asystole case (figure 2, right panel), similar observations are made. This occurred pre CPB, during jugular vein wire instrumentation for ECMO cannula placement. The PO plethysmographic waveform shows an erratic oscillating signal shortly after the asystole began. Despite the sudden asystole with hemodynamic collapse, nadir PO pulse rate reached 67 beats per minute. While the pitch dropped according to the decline in saturation, the ongoing audible rate was not in accordance with the asystole event.
DISCUSSION
The impact of patient movement and low perfusion states on the reliability of saturation readings is well known and is being addressed.2,3 The reliability of PO pulse rate measurement, however, remains under-investigated, especially during low or absent pulsatility states and when the audible tone is unaffected. Most comparisons between PO and ECG heart rate have taken place in the neonatal care setting, where pulse oximetry is known to underestimate heart rate in the first minutes after birth.4 Studies report up to 35% false bradycardia readings,5 and an overall sensitivity of (only) 89% for detecting a heart rate below 100 beats per minute.6
We reported our observations and concern for clinical consequences to both Masimo and Mindray corporations. Of note, similar observations were previously reported to Masimo in 2007,7 upon which Masimo adjusted their software allowing a disabling of the Smart Tone setting. Smart Tone was originally developed to minimize the impact of motion artifacts, but here we confirm that this algorithm may be misled by severe rhythm disturbances as well. In our current Mindray monitors, however, the Smart Tone feature is permanently enabled. This is probably the cause for the misleading audible tone rate, and the manufacturers are addressing this issue so that it can be suppressed in the Mindray monitor. In the meanwhile, we are extra vigilant and adjust the pulse rate measurement source to the arterial line whenever possible. In this setup, the pulse pitch is still derived from the PO signal, but the audible pulse rate is a reflection of the actual pulse rate.
Michael Vandenheuvel, MD, is a staff anesthesiologist in the Department of Anesthesia & Perioperative Medicine at the University Hospital of Ghent (Belgium).
Patrick Wouters, MD, PhD, is a professor and head of research in the Department of Anesthesia & Perioperative Medicine at the University Hospital of Ghent (Belgium).
Luc De Baerdemaeker, MD, PhD, is a professor and Head of Department of the Anesthesia & Perioperative Medicine at the University Hospital of Ghent (Belgium).
The authors have no conflict of interest.
REFERENCES
- Masimo Inc. Masimo Signal I.Q. whitepaper. 2010. www.asa-abstracts.com. Accessed September 4, 2023.
- Louie A, Feiner JR, Bickler PE, et al. Four types of pulse oximeters accurately detect hypoxia during low perfusion and motion. Anesthesiology. 2018;128:520–530. PMID: 29200008.
- Giuliano KK, Bilkovski RN, Beard J, Lamminmäki S. Comparative analysis of signal accuracy of three SpO2 monitors during motion and low perfusion conditions. J Clin Monit Comput. 2023:1–11. PMID: 37266709.
- Anton O, Fernandez R, Rendon-Morales E, et al. Heart rate monitoring in newborn babies: a systematic review. Neonatology. 2019;116:199–210. PMID: 31247620.
- Khoury R, Klinger G, Shir Y, et al. Monitoring oxygen saturation and heart rate during neonatal transition. comparison between two different pulse oximeters and electrocardiography. J Perinatol. 2021;41:885–890. PMID: 33250516.
- Kamlin COF, Dawson JA, O’Donnell CPF, et al. Accuracy of pulse oximetry measurement of heart rate of newborn infants in the delivery room. J Pediatr. 2008;152:756–760. PMID: 18492509.
- Forde RER, DeBros FM, Guimaraes EL, Sandberg WS. Misleading behavior of Masimo pulse oximeter tone during profound bradycardia. Anesthesiology. 2007;107:1038–1039. PMID: 18043086.
Pulse Rate from Pulse Oximeter Displayed and Audible Tone Generated During Absence of Physiologic Pulse—Masimo Response
IN REPLY:
Masimo carefully reviewed the report by Vandenheuvel et al., and identified important insights to share with the readers. In addition to submitting the report to APSF, UZ Ghent contacted Masimo to report cases where the pulse rate (PR) measurement and associated variable pitch tone from the Masimo SET board in a Mindray monitor did not indicate the actual pulse rate during cardiopulmonary bypass (CPB) and in the two non-CPB cases involving pulseless arrhythmias (ventricular fibrillation [VF] and asystole). Masimo was provided the pulse oximeter (PO) sensor used in the asystole case (RD SET E1 Ear Sensor), a digital dataset from the Mindray monitor, and alarm messages (plotted in Figure 3, top panel). Limited Mindray datasets (but not the sensors) were available for the VF and CPB cases. The compressed physiological waveforms shown in the report to APSF were also forwarded to Masimo.
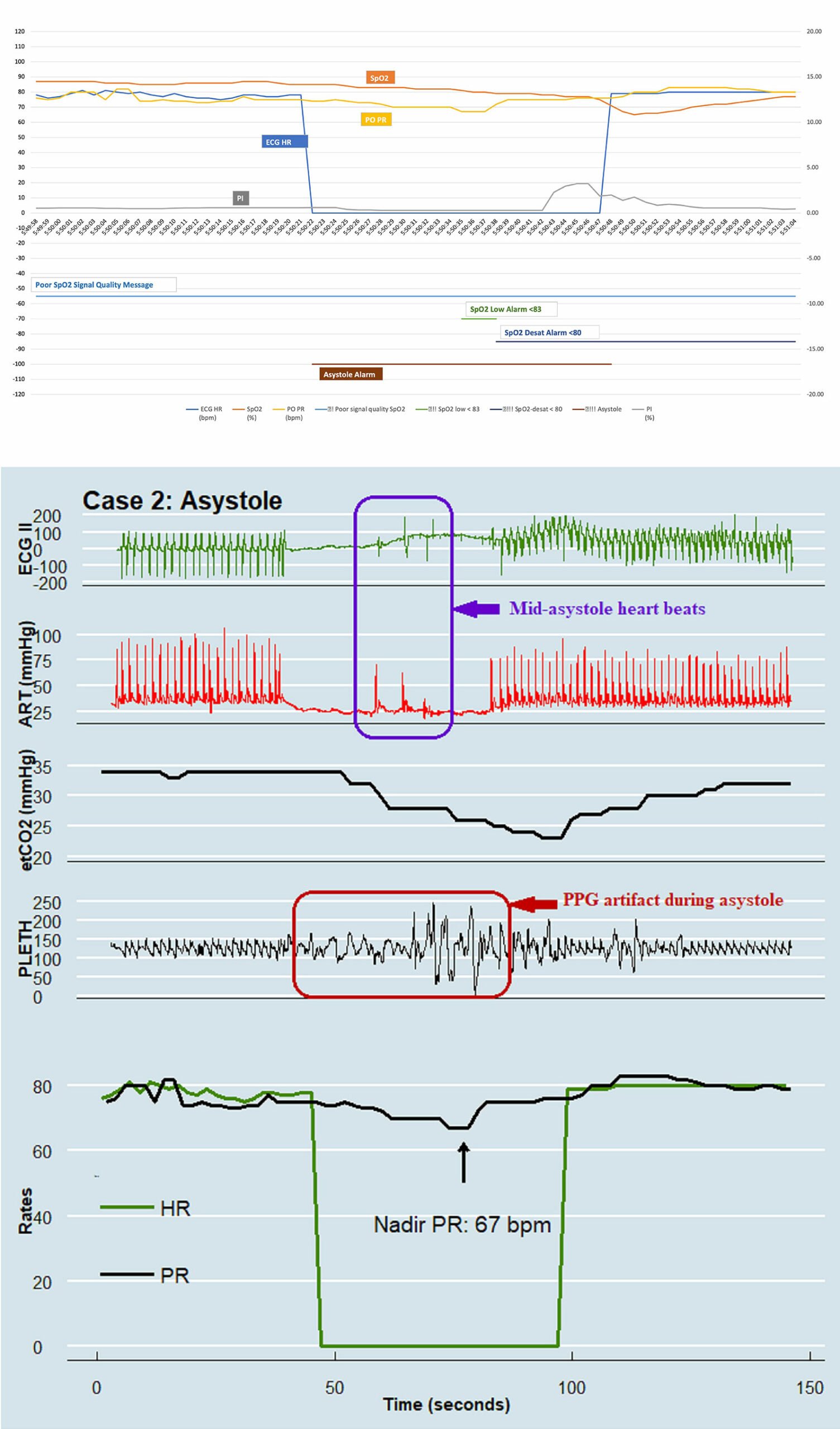
Figure 3 Legend: Top Panel: Plots of the displayed SpO2, PO PR, and ECG HR data as well as the technical alarm messages (description, timing, and duration) that were present during the asystole case. Note that ‘!Poor signal quality SpO2’ was displayed during the entire dataset, and the alarm for ‘!!SpO2 low <83’ occurred during 13–16 seconds into the asystole event, followed by the alarm for !!!SpO2 desat <80, which was displayed from 16 seconds into asystole event and continued until the end of the dataset.
Bottom Panel: Asystole case data from Vandenheuvel et al. Annotated with purple rectangle highlighting the mid-asystole heartbeats (evidenced by contemporaneous “spikes” in the compressed ECG waveform and pressure pulsations in the arterial line trace).
Masimo tested the ear sensor, which operated within specifications. The parameter and alarm data for the asystole case were compared with compressed waveforms provided for ECG, arterial pressure, EtCO2, SpO2 plethysmography waveform (pleth), and trend plots for ECG-based heart rate (HR) and plethysmography-based PR.
KEY FINDINGS:
- Per the UZ Ghent team, asystole started pre-CPB, during attempt to insert an ECMO wire/cannula into the jugular vein and ended 26 seconds after efforts ceased.
- The compressed waveforms show a few pulsatile beats during the asystole event on the ECG, arterial, and plethysmography waveforms.
- The Mindray monitor (with Masimo SET) messaged low SpO2 signal quality long before and after the event. This is important because low signal quality can impair timely, accurate measurements.
- The plethysmography waveform recorded an oscillating signal shortly after the asystole began. Given the PO sensor’s ear attachment, it is quite possible the physician actions, in proximity to head/neck/ear, during insertion and removal of the ECMO wire/cannula caused unintended motion and the resulting artifact seen in the plethysmography waveform that influenced the PO-based PR measurements. Masimo SET is designed to trigger an alarm in <8 seconds of an asystole in the absence of motion artifact. Timely recognition of the asystole event by the PO was likely impeded by the oscillatory artifact in the plethysmography signal and mid-asystole heartbeats visible in both the ECG and arterial waveforms (see purple box in Figure 3), impacting the accuracy of the PR estimate.
- The Mindray data show an SpO2 decline from 85% to 67%, and a low SpO2 alarm occurred ~13 seconds after the asystole began.
UZ Ghent did not provide Masimo with the sensor used in the VF case. However, they did send compressed parameter waveforms and 1 Hz parameter data, but no alarm message data. Key findings from the review of this data include:
- Ventricular fibrillation lasted ~24 seconds ending with defibrillation.
- The compressed waveforms show no visible artifact until a few seconds after the VF onset when an erratic oscillating signal appears on the plethysmography.
- The erratic plethysmography signal likely reflects motion artifact caused by clinicians during preparation and delivery of defibrillation, as this artifact was not present before or after the VF episode.
It is well recognized that different physiological monitoring parameters have unique accuracy, stability, reliability and confounder characteristics. For example, the HR post-defibrillation in the VF case highlights a signal-based limitation of ECG monitoring. The ECG tracing shows the HR return to its pre-VF rate of 78–80 BPM. However, presumably pronounced “T” or “P” waves in the post-defibrillation ECG caused the HR to double-count, while the PO-generated PR accurately returned to the pre-VF rate.
Similarly, the plethysmography waveform, which measures optical density changes in the sensor’s path, has limitations based on the origin of the signal. Specifically, in the absence of a true arterial pressure pulse, a confounding oscillatory signal that may mimic the shape of a true plethysmography (either clinician/motion or apparatus induced), can present a PR that is not representative of the ECG-derived HR.
It is important to note that Masimo’s plethysmography waveform reflects the raw signal recorded by its optical sensor; therefore, the waveform shape is representative of a true change in optical signal. Masimo SET’s unique signal processing algorithms are designed to accurately estimate pulse rate and oxyhemoglobin saturation during motion and low perfusion; however, the scenario in the asystole case, where there is no true arterial pressure pulse, but an oscillating plethysmography signal due to confounding factors, presents a limitation of pulse oximetry technology in general.
In the CPB examples, both cases show wide variability of mean arterial pressure during CPB. In the first case, both the ECG-derived HR and PO-derived PR are elevated when the heart is not pumping. The nonphysiologic plethysmographic waveform is likely due to a small pulse pressure produced by the CPB roller pump, a phenomenon long known by cardiac anesthesia professionals.1 Masimo SET is often capable of detecting these pulsations,1 but PO is not reliable during CPB. Indeed, Reich et al. reported that CPB accounted for over 30% of cases when PO data were unreliable for at least 10 minutes.2
Lastly, in Vandenheuvel et al’s discussion, the authors mistakenly say that Masimo’s “Smart Tone was originally developed to minimize the impact of motion artifacts.” Masimo’s SmartTone feature solely determines whether the variable pitch tone is enabled during low signal-to-noise conditions. If SmartTone is enabled, a tone reflecting the frequency of the PR and the pitch reflecting the SpO2% will be enunciated. If SmartTone is disabled, no pulse tone will be enunciated during low signal-to-noise conditions. The ability to hear the variable saturation pitch and PR frequency during low signal conditions is often well received in care areas where artifact is common and patients are consistently observed, and is less suitable in care areas where these conditions are not common.
The SmartTone feature is a configurable setting in Masimo monitors and defaulted to OFF to minimize the likelihood of SmartTone being enabled without a user understanding how it works and knowing how to turn SmartTone ON or OFF based upon the circumstances in their use case. However, in the current deployment on Mindray monitors, SmartTone is defaulted “ON” and cannot be turned “OFF.” Pursuant to learning about the experiences at UZ Ghent, Mindray considered the clinical and technical issues with an open mind, and they have agreed to make SmartTone a configurable setting defaulted to “OFF.”
In summary, the cases highlighted by the physicians from UZ Ghent provide insights and warnings for clinicians about confounding conditions that can affect PO-based PR and ECG-based HR measurements, as well as the potential downside in some clinical applications of a unique deployment of the SmartTone feature in a multiparameter monitor. Masimo and Mindray utilize feedback from our customers as vital inputs for potential opportunities to enhance user satisfaction of our products, as shown by the planned change in SmartTone deployment in Mindray monitors resulting from the collaboration with UZ Ghent physicians.
Sincerely,
Vikrant Sharma, PhD
Vice President, Optical Sciences, Masimo Corp, Irvine, CA
Steven J. Barker, PhD, MD
Chief Science Officer, Masimo Corp., Irvine, CA
Rick Fishel
President, World Wide OEM and Strategic Business Development Masimo Corp.,
Irvine, CA
Daniel Cantillon, MD
Chief Medical Officer, Masimo Corp., Irvine, CA
William C. Wilson, MD, MA
Executive Vice President, Clinical Operations, Masimo Corp., Irvine, CA
Disclosures: Vikrant Sharma, Rick Fishel, Daniel Cantillon, and William C. Wilson, are full-time employees of Masimo. Steven J. Barker is a part-time Masimo employee.
REFERENCES
- Irita K, Kai Y, Akiyoshi K, et al. Performance evaluation of a new pulse oximeter during mild hypothermic cardiopulmonary bypass. Anesth Analg. 2003;96:11–14. PMID: 12505915.
- Reich DL, Timcenko A, Bodian CA, et al. Predictors of pulse oximetry data failure. Anesthesiology.
1996;84:859–64. PMID: 8638840.
The information provided is for safety-related educational purposes only, and does not constitute medical or legal advice. Individual or group responses are only commentary, provided for purposes of education or discussion, and are neither statements of advice nor the opinions of APSF. It is not the intention of APSF to provide specific medical or legal advice or to endorse any specific views or recommendations in response to the inquiries posted. In no event shall APSF be responsible or liable, directly or indirectly, for any damage or loss caused or alleged to be caused by or in connection with the reliance on any such information.
