Color-coded medication labels are widely used in anesthesia to identify medications by their drug class. There is growing controversy regarding the safety of these medication labels. Several safety experts and organizations have raised concern that color-coded medication labels may actually contribute to medication errors by serving as a substitute to reading the label. In this pro-con debate, we argue that color-coded medication labels improve patient safety.
Related Article:
CON: Anesthesia Drugs Should NOT Be Color-Coded
PRO: Color-Coded Medication Labels Improve Patient Safety
In 2015, the American Society of Anesthesiologists released a statement supporting the practice of user-applied, color-coded medication labels.1 These labels come in nine distinct colors, each representing a specific drug class according to the American Society for Testing and Materials (Figure 1). However, the Food & Drug Administration2 and the Institute for Safe Medication Practices (ISMP)3 have voiced concern over the safety of color-coded labels. They suggest that color-coding may actually contribute to medication errors by acting as a substitute for reading the label. Additional concerns include a limited number of discernible colors, similar appearance of colors, poorly contrasting backgrounds, color-blind clinicians, and a lack of data supporting the practice of color-coding.3 Although these concerns are understandable, the benefits of color-coding are overlooked. We believe color-coded medication labels improve patient safety.
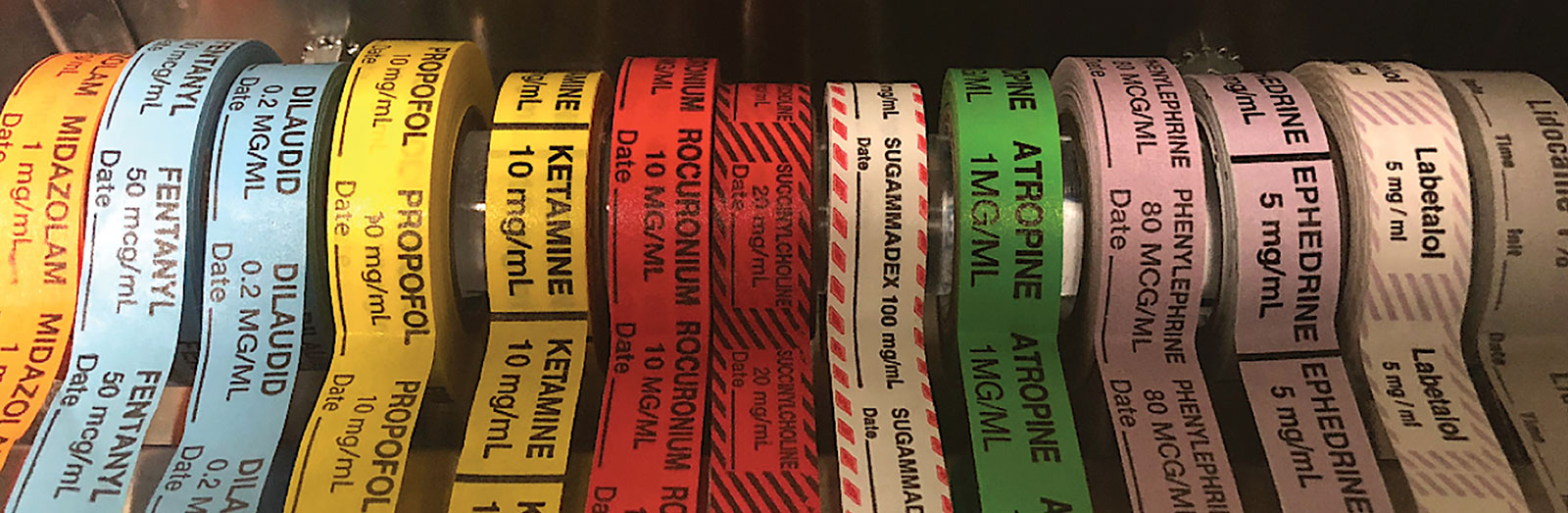
Figure 1. Color-coded medication labels used in anesthesia.
Research shows that color plays a vital role in the identification of objects. In a classic experiment, subjects were faster to identify objects in color than in grayscale. In turn, they were slowest to identify objects with incongruent color (e.g., blue strawberry).4 In another study, subjects shown a grayscale image during a functional brain MRI had such distinct activity in the visual cortex that independent experts could correctly determine the color of the object, even though the image was in grayscale (a phenomenon known as “memory of color”).5 However, you don’t need sophisticated studies to appreciate the importance of color in the interpretation of your surroundings—you live it every day. Road signs and traffic signals use color to convey meaning.6 Chefs use color-coded cutting boards to minimize allergy risk.7 Construction workers wear different colored hard hats to signify their role,8 and electricians use color-coded circuits.9 The Department of Defense,10 the Federal Aviation Agency,11 National Aeronautics and Space Administration,12 and virtually every other industry use color-coding to minimize human error. Why? Because color-coding is an essential component of human factors engineering.
Human factors engineering focuses on understanding human strengths, weaknesses, physical limitations, psychology, and fallibility, in order to create systems and devices that minimize human error. The goal of human factors engineering is to design a system that works in spite of human involvement, by decreasing reliance on memory, vigilance, and calculations. This goal is achieved by imposing the principles13,14 in Table 1.
Table 1. Principles Guiding Human Factors Engineering to Reduce Error
| Principle | Definition | Example |
| Standardization | Decreases variability of systems | Preflight checklist use in aviation |
| Forcing functions | Prevent performance of an undesired action | Impossible to shift gears of a car without applying the brake |
| Redundancy cues | Convey the same message through multiple routes | Both the color and location of the traffic light have the same meaning |
| Affordances | Communicate the intended use through inherent characteristics | A door with a push bar implies “push to open” |
| Natural mapping | Creates an obvious relationship between an object and its controller | Turning a steering wheel to the right turns the wheels to the right |
| Error Mitigation | Promotes early detection and correction of an error | Medication ordering systems alert a provider when ordering a medication with potential drug-drug interactions |
Color-coded medication labels serve two purposes. First, they act as redundancy cues in object recognition, by conveying the class of the medication through color in addition to lettering. Second, they promote error mitigation. Syringe swaps account for approximately 20% of all medication errors.15 Color-coded labels aim to contain syringe swaps to medications of the same class. Thus, if a syringe swap does occur, the initial management strategy is likely to be the correct one. For example, prior to performing a spinal you ask a colleague to give fentanyl. Soon after administration, the patient becomes somnolent and apneic. Would you suspect a narcotic overdose? If so, you’re not alone. This phenomenon is known as “anchoring bias,” in which our initial diagnosis is anchored to a recent event—in this case, the administration of what was believed to be a narcotic. Your first step would likely be to ventilate the patient and give naloxone, while further investigating the cause. After discovering a syringe swap occurred—hydromorphone was given instead of fentanyl—you continue with the current management. Even though the wrong medication was given, your corrective action was appropriate. Color-coded labels contained the error to a narcotic-related adverse event, allowing the “anchoring bias” to work in your favor, instead of against you. Now, imagine that a paralytic agent was actually the culprit. In that case, the initial corrective action may have resulted in a delay of the appropriate management.
Those opposed to color-coded labels argue that they serve as a substitute for reading the label. In fact, they would probably argue that the syringe swap example described above would have been avoided altogether if color labels were not used! By removing the color-coding, the provider would be forced to read the label to identify the medication. In other words, they hope to impose a forcing function at the expense of redundancy cues and error mitigation. There are two flaws in this logic. First, it assumes that color-coded labels lead to an increase in medication errors. If this were true, we would expect substantially lower rates of medication errors in hospital units where color-coding is not used. Yet, errors continue to occur in those locations.16 Even more telling are the results of a clinical trial with over 55,000 anesthetics, reporting zero cases of syringe swaps between drugs with the same color label.17 In fact, syringe size, not color, was most frequently associated with syringe swap errors.17 Second, their goal of “forcing” providers to read the label by removing color-coding is well-intentioned, but misguided. Labels with lettering alone are still subject to error. Medication names that are similar in length, share the same first and last letters, or have many characters in common are at risk for misidentification.18 The ISMP published a list of look-alike drugs, and advised using “tall man letters” to help distinguish these names.18 However, expecting anesthesia professionals who label their own medications by hand to use standardized “tall man lettering” is impractical.
It’s wishful thinking to believe errors would decrease if color labels were abandoned. Yes, we firmly believe every provider should read the label every single time. However, we would be foolish to ignore the lessons learned from human factors engineering and psychology research. How could any provider, at any level of training or experience, administer a medication without carefully reading the label first? Surely, these errors must be due to a lack of vigilance, intelligence, or experience… right? Well, if you have ever driven home only to realize upon arrival that you don’t remember going through a familiar intersection or traffic signal, then you’ve experienced the curious nature of human cognition. Decision-making occurs by two distinct processes: Working memory allows us to perform multiple routine tasks in parallel with little attention, while direct attention is responsible for single, complex tasks that require focus and precision.13 Faced with multiple simultaneous challenges such as hemodynamic instability, blood loss, metabolic disarray, the need to check labs, etc., the mind simply cannot use direct attention for every task at hand. Whether we care to admit it or not, some tasks will be performed with working memory. Redundancy cues, such as color-coded labels, aid working memory. If color-coded labels are removed, then other less reliable redundancy cues will be substituted to identify the medication, such as syringe size, orientation, and location.
James Reason, PhD, is the psychologist responsible for the famous “Swiss Cheese Model” of error.19 This model describes how multiple, small failures must align in order for an error to reach the patient. In anesthesia, we strive to create as many layers of defense as possible to prevent errors from reaching the patient. We insist on having two functional blades and handles for laryngoscopy, in case one handle or bulb malfunctions. We use multiple layers of defense in preventing a hypoxic gas mixture: color-coded gas supply lines, the pin-index system, an oxygen sensor, oxygen positioned as the most downstream gas, color-coded flowmeter knobs, and “fluted” oxygen knobs. Simply put, redundancy improves safety.
We share the concerns of the ISMP that there are a limited number of discernible colors, colors may look similar, poorly contrasting backgrounds may affect appearance, and color-blind providers may have a disadvantage. Regarding their claim that data is lacking in support of color-coded labels, we point to a study showing color-coded labels improve proper identification of IV bags, improve identification of errors, and reduce the average performance time of tasks.20 Color-coded labels may not be perfect, but let’s not throw the baby out with the bathwater. Just because a system is not perfect does not mean it has no value. Color-coded labels add “one more layer of cheese” to the defense against medication errors, which may be the difference between an uneventful case and an adverse event.
This pro-con debate is essentially arguing two sides of the same coin. Medication labels are only a small piece of a much larger issue. In addition to syringe swaps, errors result from mistakes in preparation, labeling, vial/ampule selection, route of administration, and communication.15 As anesthesia professionals, we have a duty to improve the system to minimize human error. Nowhere else in the hospital is a single provider responsible for prescribing, dispensing, preparing, labeling, and administering medications, as well as monitoring for adverse events. Point-of-care label makers, bar code scanning, and pre-filled syringes are important safety measures that off-load anesthesia professionals of some of these medication-related tasks and allow second-source verification, decreasing the chance of error. Unfortunately, these devices are not widely used, mainly due to cost constraints. Even with their aid, as long as humans are involved, errors will continue to occur. We support the use of color-coded medication labels, and urge all providers to always read the medication label prior to administration.
Dr. Janik is an anesthesiologist in the Department of Anesthesiology, Critical Care and Pain Medicine at NorthShore University Healthsystem and clinical assistant professor in the Department of Anesthesiology/Critical Care at the University of Chicago.
Dr. Vender is an anesthesiologist and past chairman in the Department of Anesthesiology, Critical Care, and Pain Medicine at NorthShore University HealthSystem and clinical professor in the Department of Anesthesiology/Critical Care at the University of Chicago.
Dr. Janik has no conflicts of interest. Dr. Vender is a consultant for Fresenius-Kabi.
References
- Asahq.org. Statement on labeling of pharmaceuticals for use in anesthesiology. American Society of Anesthesiologists (ASA). 2015; https://www.asahq.org/standards-and-guidelines/statement-on-labeling-of-pharmaceuticals-for-use-in-anesthesiology. Accessed November 9, 2018.
- Food and Drug Administration. Guidance for industry: safety considerations for container labels and carton labeling design to minimize medication errors. 2013; https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM349009.pdf. Accessed November 9, 2018.
- Institute For Safe Medication Practices. A spectrum of problems with using color. 2003; https://www.ismp.org/resources/spectrum-problems-using-color. Accessed November 9, 2018.
- Tanaka, J, Presnell, L. Color diagnosticity in object recognition. Percept Psychophys. 1999;61:1140–1153.
- Bannert MM, Bartels A. Decoding the yellow of a gray banana. Current Biology. 2013;23:2268–2272.
- Federal Highway Administration, Manual of uniform traffic control devices. 2009; https://mutcd.fhwa.dot.gov/pdfs/2009/mutcd2009edition.pdf. Accessed November 9, 2018.
- The Food Safety Company. Why colour coding is important. 2016; http://www.foodsafety.company/2016/11/why-colour-coding-is-important.html. Accessed November 9, 2018.
- BuildUK.org. Safety Helmet Colours. 2016; https://builduk.wpengine.com/wp-content/uploads/2016/04/Safety-Helmet-Colours-Build-UK-Standard.pdf. Accessed November 9, 2018.
- Osha.gov. (2018). Authority for 1910 Subpart S – 1910 Subpart S | Occupational Safety and Health Administration. https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_id=10135&p_table=STANDARDS. Accessed November 9, 2018.
- Department of Defense Handbook. Color and marking of army material (Metric); MIL-STD-1273B (MI) 1995; https://www.alternatewars.com/BBOW/Sources/MIL-HDBK-1473.pdf. Accessed November 9, 2018.
- Cardosi K, Hannon D. Guidelines for the use of color in ATC displays. Federal Aviation Administration, US Department of Transportation, Research and Special Programs Administration. 1999; http://www.tc.faa.gov/its/worldpac/techrpt/ar99-52.pdf. Accessed November 9, 2018.
- Standard for color code for shop machinery and equipment, John F. Kennedy Space Center. KSC-STD-0003, 1967; https://ntrs.nasa.gov/archive/nasa/casi.ntrs.nasa.gov/19670027339.pdf. Accessed November 9, 2018.
- Kohn LT, Corrigan JM, Donaldson MS. “To err is human: building a safer health system.” Committee on Quality of Healthcare in America. Institute of Medicine. 1999.
- Gosbee JW, Gosbee LL. Using human factors engineering to improve patient safety: problem solving on the front line. 2nd ed. The Joint Commission, 2010.
- Abeysekera A, Bergman IJ, Kluger MT, Short TG. Drug error in anaesthetic practice: a review of 896 reports from the Australian Incident Monitoring Study database. Anaesthesia. 2005;60:220–27.
- Wolfe D, et al. Incidence, causes, and consequences of preventable adverse drug reactions occurring in inpatients: A systematic review of systematic reviews. PLoS One. 2018;13:1–36.
- Fasting S, Gisvold SE. Reports of investigation: adverse drug errors in anesthesia, and the impact of coloured syringe labels. Can J Anesth. 2000;47:1060–1067.
- Institute For Safe Medication Practices. (2018). Special Edition: tall man lettering; ISMP updates its list of drug names with tall man letters. https://www.ismp.org/resources/special-edition-tall-man-lettering-ismp-updates-its-list-drug-names-tall-man-letters. Accessed November 9, 2018.
- Reason J. Managing the Risk of Organizational Accidents. Burlington, VT: Ashgate Publishing Company; 2000.
- Porat N, et al. Use of colour-coded labels for intravenous medications and lines to improve patient safety. Qual Saf Health Care. 2009;18:505–509.
